
Abstract
Background:
In an earlier continuous glucose monitoring (CGM)-based study, we reported that sitagliptin not only reduced 24-h mean glucose levels but also suppressed postprandial glucose increases, thus reducing the range of glycemic fluctuations in type 2 diabetes patients. In this study, we investigated whether sitagliptin might provide similar benefits in type 2 diabetes patients receiving insulin therapy by using CGM.
Patients and Methods:
The study included a total of 13 type 2 diabetes patients in whom stable glycemic control had been achieved after admission for glycemic control. Insulin regimens used included long-acting insulin preparations once daily in four patients and biphasic insulin preparations twice daily in nine, with the daily insulin dose being 19.0±12.7 U. During the CGM-based study, the patients were given insulin therapy alone on Days 1 and 2 and were given sitagliptin 50 mg/day as add-on treatment on Days 3–6, with their daily insulin doses maintained.
Results:
The add-on treatment with sitagliptin led to significant decreases in 24-h mean glucose levels and SDs of 288 glucose levels measured by CGM for 24 h, as well as in the indices for magnitude of glucose variability and proportion of time in hyperglycemia, compared with insulin therapy alone (P<0.01), whereas there was no significant change seen in regard to the proportion of time in hypoglycemia with or without add-on treatment with sitagliptin.
Conclusions:
This CGM-based study clearly demonstrated that insulin therapy alone, whether with long-acting or biphasic insulin preparations, does not provide adequate glycemic control in type 2 diabetes patients. In contrast, add-on sitagliptin was shown to narrow the range of 24-h glucose fluctuations in these patients, suggesting that add-on treatment with sitagliptin is effective for postprandial glucose control in type 2 diabetes patients receiving insulin therapy.
Introduction
Against this background, there is an increasing stress on the need to control diurnal glycemic variability that HbA1c fails to reflect, which has led to the need for assessing diurnal glycemic fluctuations in diabetes patients by using continuous glucose monitoring (CGM) being widely recognized in recent years.
Again, the range of insulin preparations available for glycemic control in not only type 1 but also type 2 diabetes has widened in recent years to include long-acting insulin whose efficacy is sustained over an extended period of time, as well as biphasic insulin, which includes soluble rapid-acting insulin along with an intermediate-acting protaminated rapid-acting insulin that provides coverage of prandial and basal insulin in a single injection, with the caveat, unfortunately, that long-acting insulin given once daily and biphasic insulin given twice daily before breakfast and dinner appear to produce far from sufficient control of diurnal glycemic fluctuations, including postprandial hyperglycemia.
In this situation, where increasing insulin doses in diabetes patients without increasing the number of injections designed not to compromise patient quality of life or treatment compliance may place these patients at risk of developing hypoglycemic episodes, addition of an oral hypoglycemic agent to insulin appears to represent a viable option for correcting postprandial hyperglycemia.
Of note is that the dipeptidyl peptidase-4 inhibitor sitagliptin has been shown to inhibit degradation of incretins (and thus enhance incretin action), to promote insulin secretion, and to inhibit glucagon secretion in a glucose-dependent manner. 3 In this regard, we previously reported in a CGM-based study that the use of sitagliptin in combination with other oral hypoglycemic agents helps correct diurnal glycemic fluctuations as well as narrow its range in type 2 diabetes patients. 4
In this study, we investigated how the use of sitagliptin in combination with insulin may affect 24-h glycemic fluctuations by using CGM.
Patients and Methods
Patients
This study was designed as a prospective, nonblinded, pilot study and has been approved by the Ethics Committee of Shinyamanote Hospital (Higashimurayama, Japan). All subjects were sufficiently informed about the study and gave informed consent to participate in the study prior to the conduct of the study.
Of all type 2 diabetes patients who had been admitted to our hospital for glycemic control and in whom stable glycemic control had been obtained with insulin therapy, those who met the following criteria were included in the study: (1) age at study entry of 20 years old or older but younger than 76 years old; (2) HbA1c (NGSP) at admission of 6.9% or higher but less than 10.4%; (3) urinary C-peptide level at admission of 10 μg/day or higher; and (4) receiving an insulin regimen, long-acting or mixed insulin only, with the daily insulin dose being 40 U/day or less. A subject was excluded from the study if he or she met any of the following criteria: (1) the subject had type 1 diabetes (glutamic acid decarboxylase antibody–positive, with the urinary C-peptide level being 10 μg/day or lower); (2) the subject was receiving an oral hypoglycemic agent or agents in addition to insulin; (3) the subject had a history of serious infection within the last 3 months; and (4) the subject had received oral steroid for treatment (e.g., had rheumatism) in the last 3 months.
Procedures
Once stable glycemic control had been achieved in the subjects with insulin therapy in addition to diet therapy after their admission, the subjects were monitored by using CGM (CGMS® System Gold™, Medtronic MiniMed Inc., Northridge, CA) for 6 consecutive days and were given sitagliptin once daily before breakfast from Day 3 of CGM onward. From CGM data obtained on Day 2 of CGM as well as on Day 4 of sitagliptin therapy (Day 6 of CGM), the following parameters were calculated: 24-h mean glucose levels and their SD values; mean amplitude of glycemic excursions; total area for the range of 24-h glycemic fluctuations; and proportions of time in hyperglycemia (≥180 mg/dL) and hypoglycemia (<70 mg/dL). All CGM data were analyzed by using CGMS Solutions™ software (Medtronic MiniMed).
Statistical analysis
All statistical analyses were performed by using SAS version 9.1 (SAS Institute, Cary, NC). CGM data available before and after sitagliptin therapy from Days 2 and 6 of CGM were compared by using the Wilcoxon signed-rank test.
Results
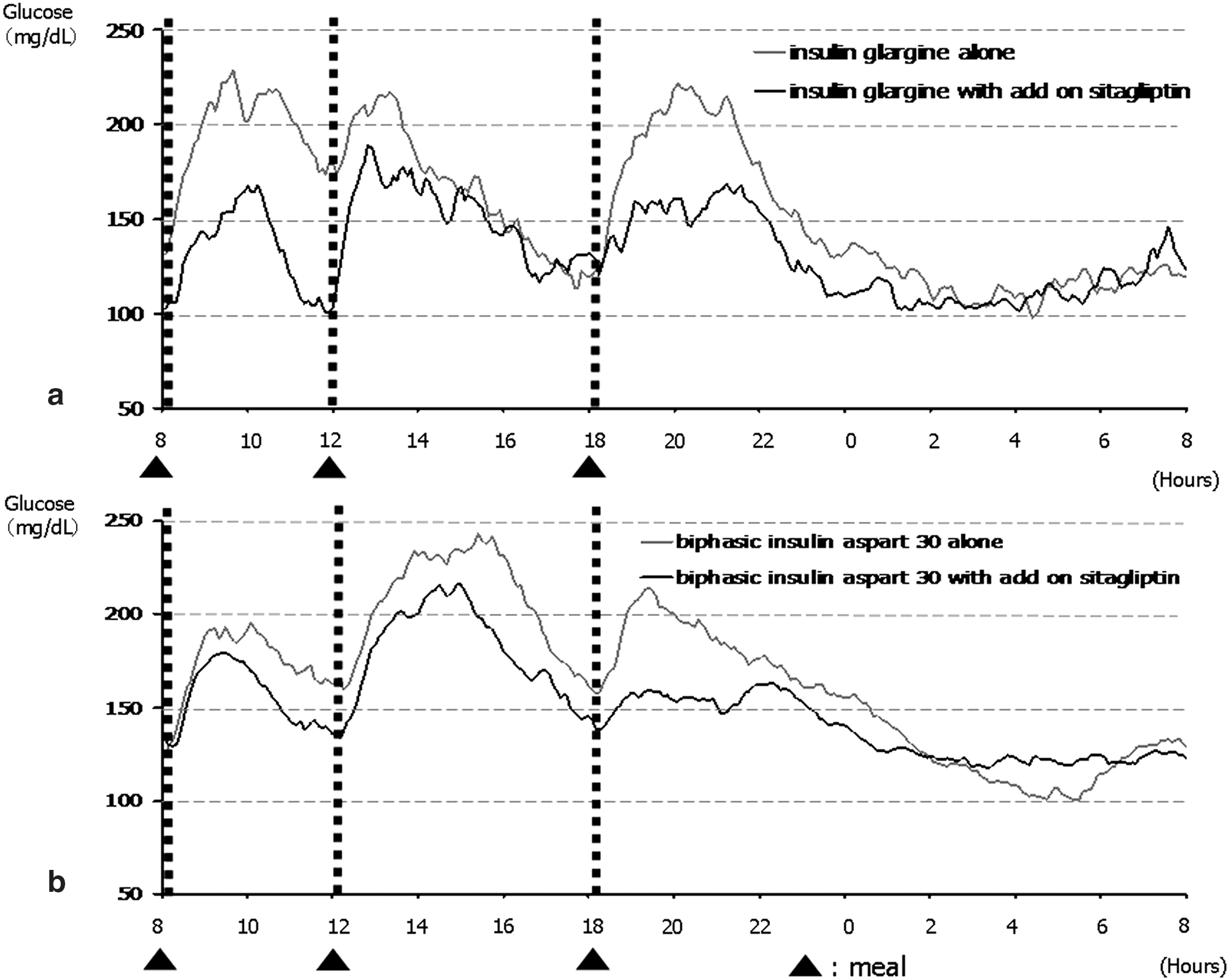
The mean age of the 13 patients (11 men, two women) included in the study was 65.2±11.7 years. Their mean body mass index was 25.0±3.5 kg/m2. Their mean HbA1c at admission was 9.5±1.0%. Their mean urinary C-peptide level was 64.0±43.7 μg/day. Insulin regimens used were long-acting insulin preparations (insulin glargine; Sanofi-Aventis, Paris, France) once daily in four patients and biphasic insulin preparations (biphasic insulin aspart 30; Novo Nordisk, Bagsvaerd, Denmark) twice daily in nine patients, with the mean daily insulin dose being 19.0±12.7 U/day.
The changes observed in diurnal glycemic fluctuations before and after sitagliptin therapy in four patients treated with insulin glargine once daily (Fig. 1a) and nine patients treated with biphasic insulin aspart 30 twice daily (Fig. 1b) demonstrated that hyperglycemia observed after all meals taken before sitagliptin therapy was improved and that hyperglycemia observed before meals was markedly improved in the patients after sitagliptin therapy. An analysis of glycemic fluctuations in the patients also showed that sitagliptin significantly (P<0.001) reduced the proportion of time in hyperglycemia (≥180 mg/dL) without increasing the proportion of time in hypoglycemia (<70 mg/dL) in these patients, which in turn led to significant reductions in indices for glycemic fluctuations, including the SDs of 24-h 288 glucose levels (P<0.001), mean amplitude of glycemic excursions (P<0.001), and the total area for the range of 24-h glycemic fluctuations (P<0.05), as well as in 24-h mean glucose levels (P<0.001) (Table 1).
The 24-h glycemic fluctuations in type 2 diabetes patients receiving
P<0.05, b P<0.001 versus insulin therapy alone.
MAGE, mean amplitude of glycemic excursion.
Discussion
Dipeptidyl peptidase-4 inhibitors are reported to inhibit degradation of the endogenous incretin hormones glucagon-like peptide-1 and gastric inhibitory polypeptide, enhance the mechanisms of action of the incretins that glucose-dependently promote insulin secretion as well as inhibit glucagon secretion, and help correct hyperglycemic states. 3 In this regard, our study results suggest that, through addition of sitagliptin, the incretins enhanced bolus insulin secretion in response to postprandial glucose increases and led to improvements in postprandial hyperglycemia and premeal glucose levels, which in turn led to decreases in 24-h mean glucose levels. In contrast, it is easy to imagine that increasing insulin doses to correct hyperglycemia after dinner such as that shown in Figure 1 could have led to nocturnal hypoglycemic episodes in these patients. Indeed, a study of type 2 diabetes patients with poor glycemic control despite insulin therapy randomized to add-on sitagliptin or dose-intensified insulin therapy for 24-h follow-up 5 showed that HbA1c was significantly decreased in those given sitagliptin compared with those given dose-intensified insulin, with significantly fewer hypoglycemic episodes and with no such weight gain as seen in those given dose-intensified insulin.
In this study, sitagliptin was shown to correct hyperglycemia after dinner only without affecting the nighttime glucose levels in those given sitagliptin as add-on to insulin therapy, in agreement with the study mentioned noted. 5 That is to say, promoting insulin secretion as well as inhibiting glucagon secretion in a glucose-dependent manner with sitagliptin is thought to be extremely useful for glycemic control in patients in whom endogenous insulin secretion is kept relatively intact, even when they are receiving insulin therapy. Given that sitagliptin has been shown to decrease mean glucose levels associated with narrowing of the range of glycemic fluctuations when used in combination with insulin, sitagliptin appears to be suitable for correcting postprandial hyperglycemia, with the potential to protect against macrovascular complications through its ability to improve postprandial hyperglycemia and glucose spikes that fail to be captured by HbA1c monitoring alone. 1,6
Conclusions
Study results showed that the dipeptidyl peptidase-4 inhibitor sitagliptin improves not only postprandial but also premeal hyperglycemia, thereby narrowing the range of glycemic fluctuations, even when used in combination with insulin therapy, in type 2 diabetes patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.