
Abstract
Background:
Pregnancy and early motherhood are extraordinarily demanding periods for women with type 1 diabetes, who therefore need optimal support. This article describes the process of developing person-centered Web-based support for women with type 1 diabetes during the period of pregnancy through early motherhood. Important aspects of person-centeredness are a broader scope of medicine, viewing the patient as a person, shared decision-making to accomplish a therapeutic alliance, and the role of documentation.
Materials and Methods:
A participatory design was used in the development process to capture the target group's knowledge, experiences, and needs, and a systematic process map for Web-based support was used to describe the process.
Results:
Content and layout in the Web support were developed collaboratively by project managers, advisory and scientific reference groups, technical producers, and representatives for the target group. Based on needs assessment and evidence synthesis, three main components of complementary Web-based support were identified: (1) specific information about pregnancy, childbirth, and early motherhood in relation to type 1 diabetes; (2) a self-care diary, including a device for documenting and evaluating blood glucose levels, insulin doses, food intake, physical activities, and overall well-being; and (3) a forum for communication between women with type 1 diabetes in the childbearing period.
Conclusions:
Using a perspective of person-centered care, a participatory design and the process map were fruitful for developing person-centered Web support for self-care and self-learning. The developed Web support product will be evaluated in a randomized controlled trial and further developed based on this result.
Introduction
Five core areas have been identified in person-centered care: applying a broader scope of medicine, approaching the patient as a person, developing a therapeutic alliance, accomplishing shared decision-making, and expressing this in documentation. 8 Incorporating these core areas in care and support to women with type 1 diabetes in the episode of pregnancy, childbirth, and early motherhood is assumed to empower them to handle the illness in daily life and to ensure a secure transition to motherhood.
Based on indications in research on other patient groups, 9 –11 we believe that Web support, including possibilities for documentation and shared decision-making as a complement to usual healthcare organizational arrangements, may strengthen self-management capabilities. This could lead to improved behavioral change outcomes and thus improved health outcomes. The Internet is increasingly used in relation to diabetes 2 and to pregnancy and childbirth. 12 Use of Internet communication can among young women with type 1 diabetes enhance their sense of autonomy and be a way of managing the transition to motherhood. 13 To our knowledge the use of person-centered Web-based support has not yet been studied in relation to type 1 diabetes and childbearing. In summary, there is a need to develop person-centered models of care for women with type 1 diabetes in relation to pregnancy and childbirth, and it is suggested that directed Web-based support promotes self-care. In response to these hypotheses, the aim of this article is to describe the process of developing person-centered Web support for women with type 1 diabetes during the period of pregnancy through early motherhood.
Materials and Methods
Design and process framework
A mapping exercise was performed of existing Web sites in Sweden for women with diabetes with the focus on issues around pregnancy, childbirth, and early motherhood. Besides static but insufficient information, no integral Web support for this target group was identified, either on “diabetes” Web pages or on “parent” Web sites. The only similar national product was a Web prototype supporting childhood chronic disease management. 9
A research project, MODIAB-web (MOtherhood and DIABetes–web support), was established to develop and implement person-centered Web-based support and to test and evaluate it scientifically in a randomized controlled study. In order to enroll participants in the development process, approval was obtained from the Regional Ethics Board (protocol number 659-09).
We used a participatory design approach to develop the Web prototype. Participatory design is a research approach with its own ethics and flexible methods including three central parts: initial exploration of work, discovery process, and prototyping to capture a target group's knowledge, experiences, and needs and to involve users in the design process. 14 Deep commitments to democracy, including openness to contradictions and discussions of values in design and imagined futures, are crucial. 15
The development process was inspired by the systematic two-phase process map for systems development of Web-based support suggested by Elwyn et al. 16 in a scientific article published just after the process had started. The process map proposes key categories of participants who should be allowed to give input to and be a part of the development process: project managers, advisory and scientific reference groups, technical producers, and, certainly not least, stakeholders. Two general principles should guide a systematic process framework. First, the content specification phase includes needs assessment, evidence synthesis, and consensus on evidence. Second, the design phase includes storyboard, sandpit testing, usability testing, and field testing. 16
Setting and procedure
Initially, the Web-based support was developed for women with type 1 diabetes who were connected to one university hospital or one county hospital in the western part of Sweden. As suggested, 16 we identified key participants in the developmental process: researchers, mothers with type 1 diabetes, healthcare professionals representing different specializations in both diabetes and perinatal care, and Web designers. We conducted a Web-based survey and held dialogues with professionals and mothers who had type 1 diabetes and had recently experienced childbearing. We also performed iterative text formatting and reviewing. An online project platform was established that included project protocols of activities with planning, implementation, and evaluation. The whole process took 15 months from the first meeting of the research group until the Web site and a subsequent adaptation to both computer and smartphone technology was completed.
Results
Key participants
The Project Management Group with executive control over the project involved one scientific leader (M.B.) and two project leaders, one for each hospital (C.L.S. and A.A.). As the idea and structure of the Web-based support was developed, different groups were consulted to provide expertise; these included both professionals and patient representatives. Details on these experts are given in Figure 1.
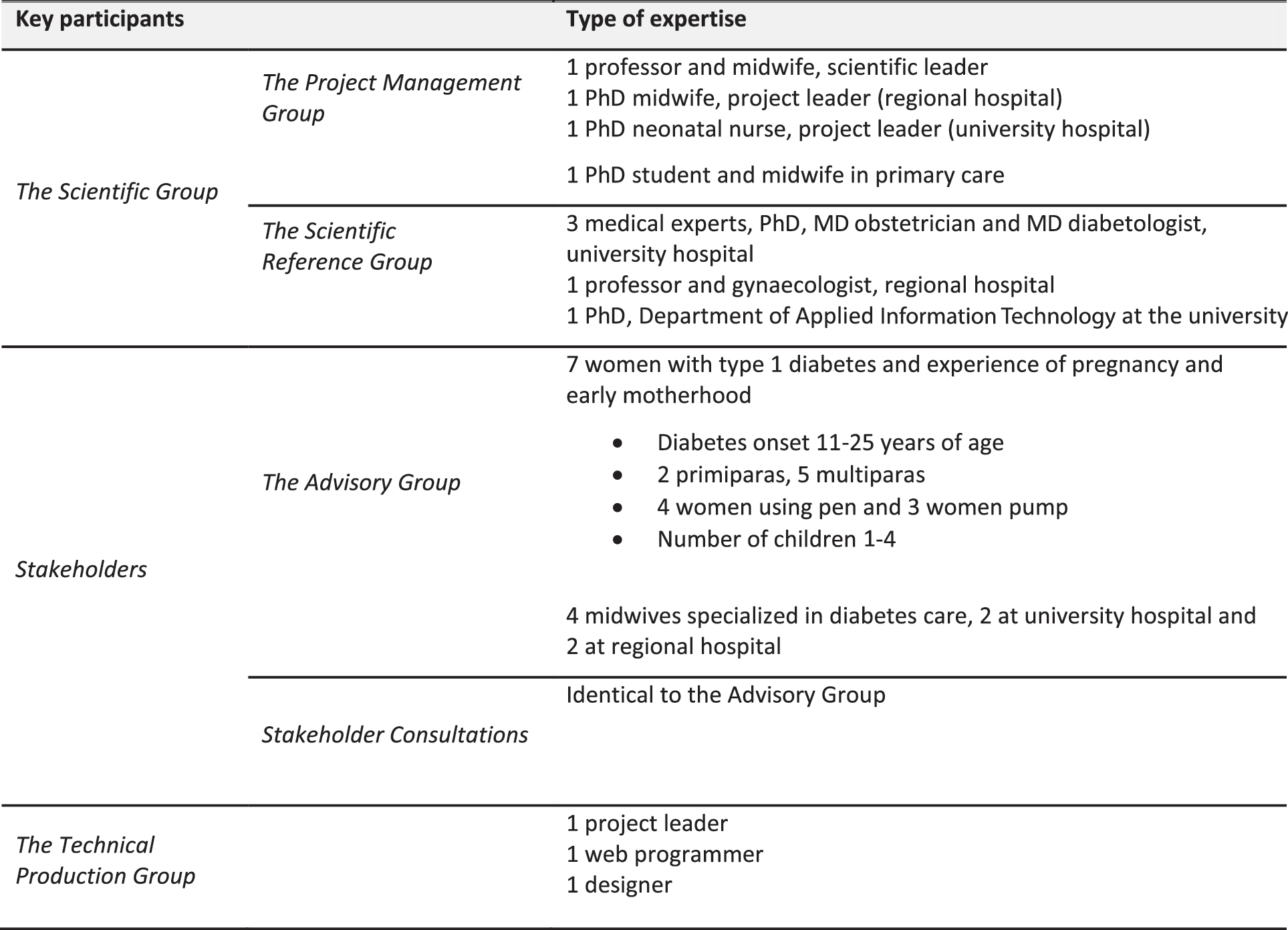
Key participants and types of expertise.
During the development phase, experts in the Scientific Reference Group were repeatedly consulted in relation to forming a main research project plan, discussing the Web site prototype, reviewing the content of information, and assessing the intervention as a whole. The Advisory Group provided input on dissemination strategies and advice about content, structure, and usability, while the Stakeholder Consultation Group contributed feedback on different versions of the Web site prototype. A Technical Production Group was established by a contracted company; their contract also clarified that the Project Management Group was the owner of the intellectual property (i.e., the Web site prototype as a whole). Later in the development process, the Technical Production Group disseminated strategies and gave advice about content, structure, and applicability.
Content specification phase
Step 1: Needs assessment
Needs of the target group—women with type 1 diabetes in the period of pregnancy through early motherhood, including breastfeeding—were identified in both our own 3,6,7,17 –19 and additional international research publications. 4,5,20 –26 An example of such an identified need was the women's call for sharing common experiences with others in similar situations, a need that could not be met within the healthcare setting.
Step 2: Evidence synthesis
According to Elwyn et al., 16 evidence should be synthesized in order to provide the core content for Web-based interventions. The identified scientific literature in Step 1 concluded that the period of pregnancy through early motherhood is challenging and demanding for women with chronic diabetes. There are increased risks for preeclampsia, malformations, fetal asphyxia, cesarean section and instrumental vaginal birth, perinatal mortality, and neonatal complications. 27,28 The most important factor for optimizing chances of having a healthy child is maintaining maternal normoglycemia 24 h/day during pregnancy. 3,6,17,27 Hypoglycemic episodes are frequent, and the body is experienced as changed and unpredictable, especially during the first trimester, probably related to lower blood glucose levels and to changes in hormonal secretion. 17,23,29 During a demanding pregnancy, feelings of stress, worry, pressure, and insufficiency are central and are combined with insecurity and unpredictability. 17,21,22 Pregnancy and childbirth involve extensive health care, but the mothers have experienced it as mainly focusing on fetal and neonatal health and not on their own well-being. 6 The duration of breastfeeding is shorter because of several aggravating circumstances. 18,24 –26
In Sweden there is a gap in organizational arrangements after childbirth, in that the mothers with diabetes are left in between maternity care and diabetes care. This makes their transition to motherhood challenging, as they try to structure a daily routine that includes caring for the newborn, establishing breastfeeding, and at the same time managing fluctuating blood glucose levels and adapting to lower insulin doses. 7 From the Internet, these mothers during the childbearing period need specific information related to having diabetes. 19 They also need peer support, including emotional and confirmative support, from other mothers with diabetes. 7,19,30
Step 3: Consensus on evidence
The synthesized scientific evidence identified three main components of complementary Web-based support to the target group: • Specific information about pregnancy, childbirth, and early motherhood in relation to type 1 diabetes • A self-care diary including a device for documenting and evaluating blood glucose levels, insulin doses, food intake, physical activities, and overall well-being • A forum for peer support through communication with other women with type 1 diabetes in the childbearing period.
Design phase
The creative design phase started with a half-day workshop, conducted in order to create a formal description of how the suggested three components, meeting the needs of the target group (storyboard), could be transformed into an operational and hosted Web site. A specification document was formulated listing requirements for site structure, layout, design, and content based on presumptive components in the suggested Web site. After evaluation of several offers based on the specification document, a contractual arrangement was settled with one company. The contract covered the cost and the specification details, the timetable, and Web hosting and support services. Next was the sandpit testing phase, which included several intensive discussions with stakeholders and the scientific group, where free thinking was encouraged in order to uncover innovative solutions. In this phase, a prototype structure was transformed to a Web site with the three main components: information specific to diabetes and childbearing; a self-care diary with documentation and visualization of measures; and a forum for peer support.
The next step in the design phase was usability testing by the Advisory Group. The experienced mothers tested and evaluated the prototype, 31 and the midwives specialized in diabetes care assessed it from a professional point of view. Examples of their opinions on the product under development are outlined in Figure 2.
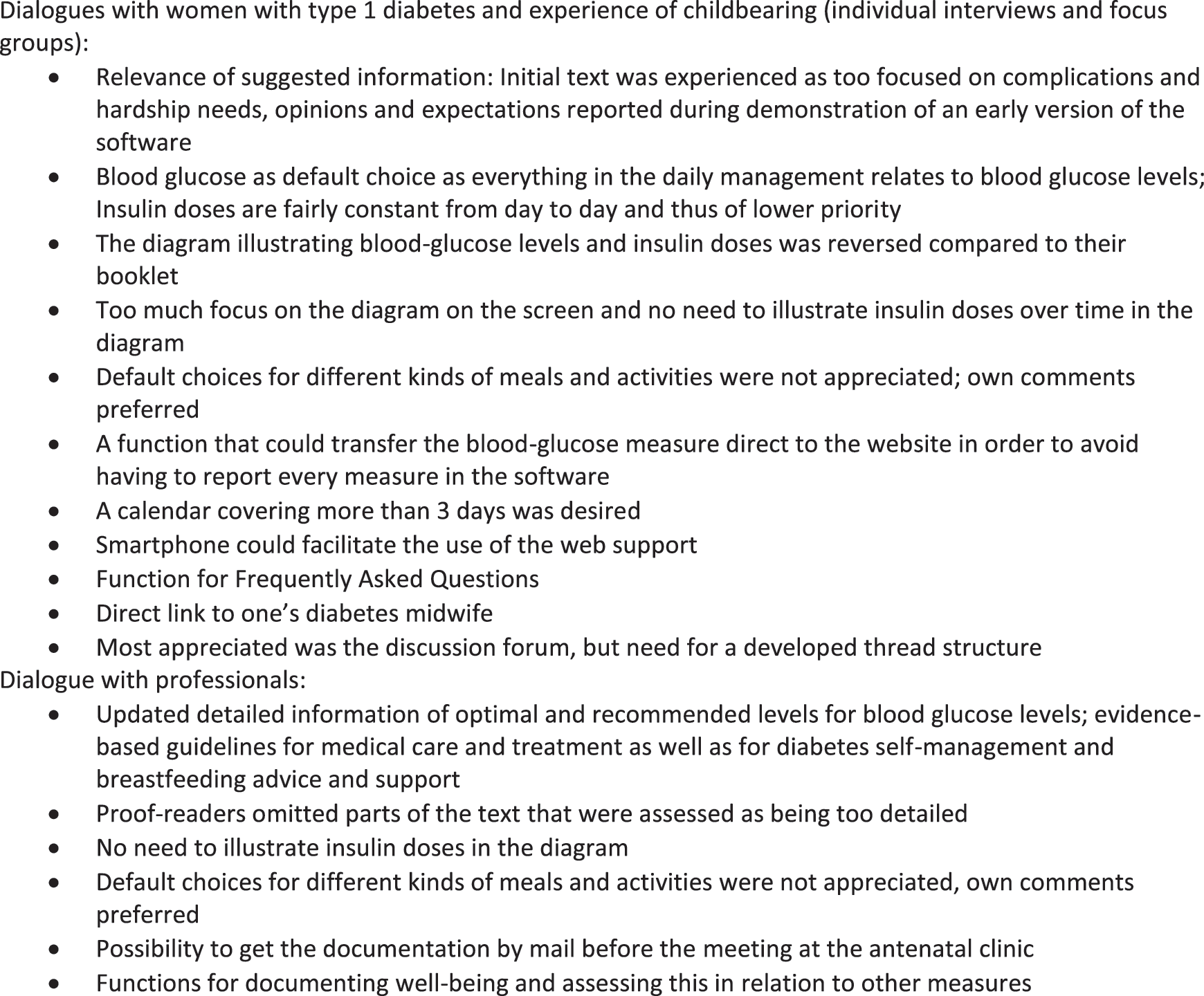
Usability testing: examples of evaluative responses from key stakeholders.
After several revisions of layout and design of the main components of the Web site, a final prototype was established in a last field-testing phase. An overview, taken from one of the pages on the Web site, is shown in Figure 3.
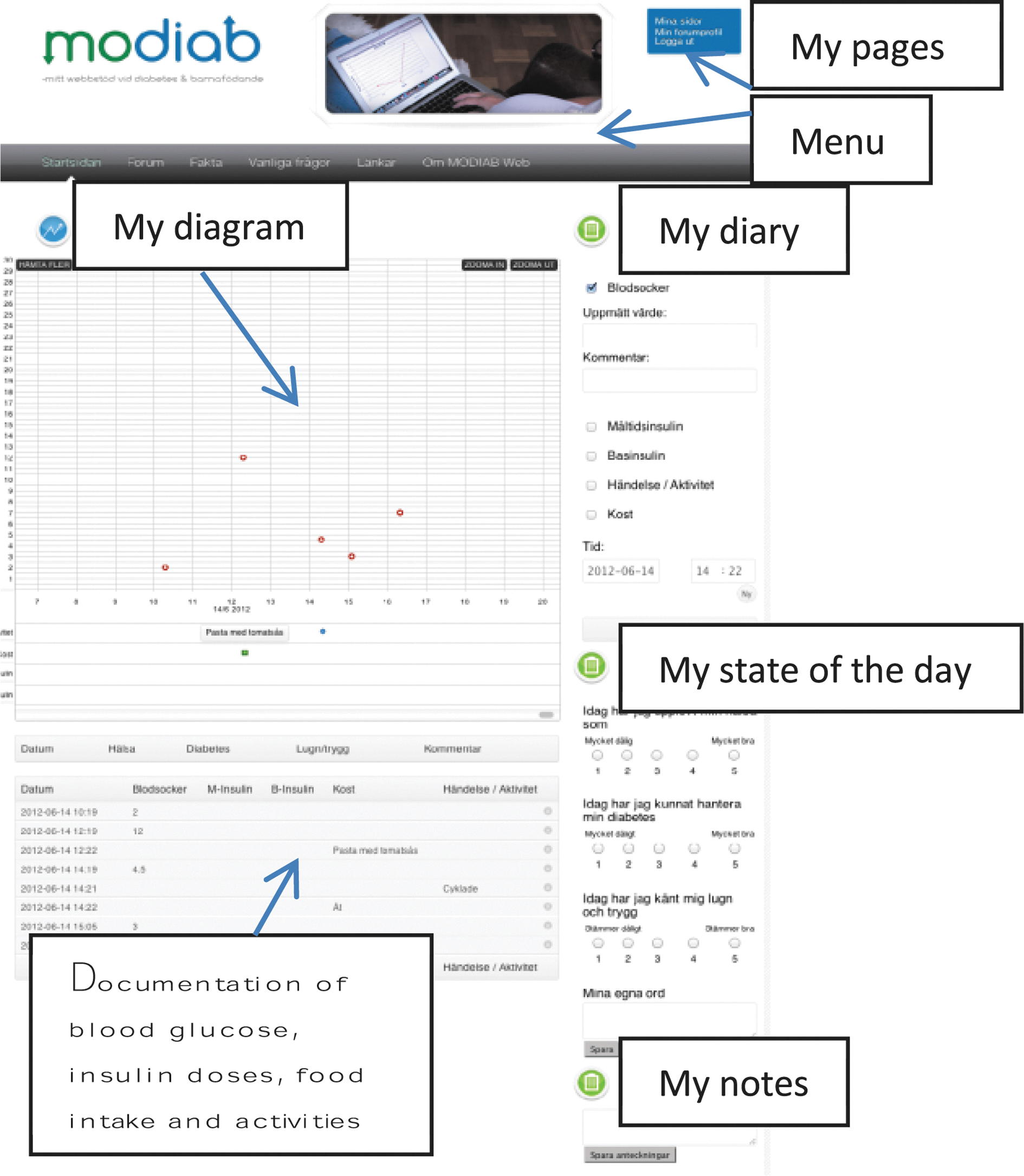
Overview of main functions in the final prototype of the developed person-centered Web site. The original text is in Swedish. The boxes, with explanations in English, are added for the international reader to get an overview of the main functions. The menu includes the following: Start page, Forum, Facts, Links, FAQ, About the MODIAB [MOtherhood and DIABetes] Web site. Color image available online at
Discussion and Conclusions
This healthcare program of person-centered Web-based support, including specific information, a self-care diary, and a forum for peer support, has been developed to bridge the gap between healthcare organizations and to support self-management for women with diabetes during the period of pregnancy through early motherhood.
The collaboration between researchers and key stakeholders, including the target group and the healthcare specialists, was an important but also time-consuming process. The perspective of person-centered care helped us apply a broader scope involving the patient as a person in both the process and the final product. The product's intention is to assist shared decision-making, building on a therapeutic alliance between the mother with diabetes and the healthcare providers, and on the woman's documentation. 8 Both the participatory design focusing on the person as a center of activity in the development process and, we believe, the product as such (Fig. 3) will strengthen the individual's self-care ability by promoting decision-making in daily life. 10,11 The diverse interaction with representatives from the target group—through focus groups, 31 individual contacts, and Web-based survey 19 —was necessary and fruitful. In a twofold way, it was also in line with person-centeredness. Involving patients and caregivers in the development as well as in the provision of support (for example, the peer support forum) also enhances a therapeutic alliance and is consistent with the participatory design approach. 14 Contributing to previous research with the intention to strengthen the unique patient with diabetes through various methods is aligned with an “empowerment agenda” 32 ; we here add experiences of design and technology use based on the specific theoretical perspective of person-centered care. 8
The process map developed by Elwyn et al. 16 was useful, although, despite their suggestion, it was not possible to develop a final tool. After using the Web support prototype for some months in a randomized controlled study, we have already made changes both in the information package and in the self-care diary technical device as a result of feedback from users and clinicians. The fourth step of the field test (practical use) in the final tool is thus an ongoing process. As concluded by Storni, 33 to enable appropriation of technology supporting self-care, there is a need to move beyond technological determinism in reflecting on whose interests the technology serves, thus taking seriously the ideal of person-centeredness. This includes adopting Web-based support according to the emergent experiences and needs of the women with diabetes.
Methodological considerations
The participatory design, 14,15 with participation of researchers, healthcare professionals, mothers with type 1 diabetes, and Web designers, was crucial in the pursuit of an optimal Web prototype. We have used the broad process map for development as described by Elwyn et al. 16 instead of a more specific one focusing, for example, on learning and community exchange such as that described by Ekberg et al., 34 and not including detailed phases with the selection of scientific data, principles for architecture, organization of prepilot usability testing, and clinical testing as proposed by Berry et al. 35 We nevertheless assess our chosen development process as effective in keeping the key participating actors in focus. On the other hand, our account of experiences (Fig. 2) did not allow for an evaluation of details in different conflicting or complementary perspectives among the actors. 36
The Web prototype developed does not provide an automatic electronic transfer of data from the blood glucose meters or insulin pumps when used. The challenge is to integrate the blood glucose meter data and the data on administered insulin dosages and on other events influencing blood glucose, such as food intake, physical activity, and personal mood. The current Web application adapted to smartphones can be further developed to transfer and integrate measures from different devices. For people with diabetes, the use of mobile software distribution platforms is decisive as they are easily accessible, decision-supporting tools in daily life. However, for visualization and evaluation of the user's daily documentation, computers are still more applicable in the clinical visits and form the basis of a partnership for decision-making.
Conclusions and practical implications
Taking a person-centered care approach 8 means that the women with diabetes must be treated and supported in ways that allow them to be people rather than objectified as individuals with a chronic illness, including an established therapeutic alliance with healthcare professionals. The application of a participatory design 14 and a general process map for development of Web-based support 16 has safeguarded person-centeredness for these women. Professional actors (researchers and clinicians in collaboration with technicians) were necessary in the development process, but more important were the representatives of the users, mothers who had type 1 diabetes and had recently experienced childbearing. The next step is ongoing: to test the developed Web support for self-care and self-learning in a randomized controlled trial.
Footnotes
Acknowledgments
This work was supported by the University of Gothenburg Centre for Person-Centred Care, the Swedish Diabetes Association, the Inger Hultman Foundation, and The Region Västra Götaland.
Author Disclosure Statement
No competing financial interests exist.