
Abstract
Background:
Individual sulfonylurea agents differ in pharmacokinetic properties and clinical effects. This study aimed to describe the usage pattern, glycemic improvement, hypoglycemia, and change in body mass index (BMI) observed with commonly used sulfonylureas.
Subjects and Methods:
Patients of either gender with type 2 diabetes mellitus (T2DM), between 18 and 75 years old and requiring addition of a sulfonylurea to an ongoing regimen of oral antihyperglycemic agent(s), were enrolled. Glycosylated hemoglobin (HbA1c) and BMI were assessed at both baseline and the end of 12 weeks of follow-up. The hypoglycemia score was assessed at the end of follow-up only.
Results:
In total, 1,069 patients were enrolled in the study, of whom 950 were considered evaluable. After a mean follow-up of 14.34±2.80 weeks, the HbA1c level decreased by 0.86±2.28%, BMI increased by 0.13±0.78 kg/m2, and mean hypoglycemia score was 0.98±1.42. A weak negative, statistically significant correlation (r=−0.093; P=0.0044) between hypoglycemic scores and increase in BMI was observed. No correlation was observed between change in HbA1c level and change in BMI. Glimepiride was the most commonly prescribed sulfonylurea (75.3%). For patients on glimepiride, a weak positive, statistically significant correlation (r=0.098; P=0.0082) between its dose and the hypoglycemic score was observed.
Conclusions:
Various sulfonylurea agents appear to differ in their effect on glycemic control, tendency to cause hypoglycemia, and gain in BMI. Hypoglycemia caused by these agents appears not only to be dose related, but also correlates inversely with gain in BMI.
Introduction
As per the Indian Council of Medical Research guidelines for diabetes treatment, 4 sulfonylureas, alongside metformin, remain the mainstay of treatment for type 2 diabetes mellitus (T2DM). The Council also recommends that therapy should be initiated with the minimal effective dose and titrated upwards every 2 weeks until the desired control or maximal dosage is reached. Numerous drug utilization studies conducted across India indicate that sulfonylureas are indeed very extensively used to manage patients with T2DM, usually as first-line or as second-line agents. 5 –9
Although sulfonylureas have been the mainstay of pharmacologic management of T2DM for many decades, concerns related to their safety have been rapidly growing in recent years, particularly with respect to hypoglycemia and gain in body weight. 10 Different molecules within the sulfonylurea class differ in their clinical effects like glycemic efficacy, risk of hypoglycemia, and tendency to gain weight. 11 For instance, there are important differences in incidence and pattern of hypoglycemia associated with different molecules. 12 These differences in clinical effects could be attributed to underlying pharmacokinetic factors, including rapidity of onset of action, plasma half-life, presence or absence of active metabolite, duration of action, and affinity for sulfonylurea receptor. 11 Furthermore, most of these clinical effects are dose-dependent, and their mechanisms may be interrelated. 11 It has been suggested that weight gain with sulfonylureas is primarily due to reduction of glycosuria and increased calorie intake to prevent or treat hypoglycemia. 13
Hence, the current post hoc analysis of results of the Observational Study to Assess Correlation between Glycemic Control and Hypoglycemia in Patients with Type 2 Diabetes Treated with Sulfonylureas (OBSTACLE hypoglycemia study) aimed to describe usage pattern, glycemic efficacy, hypoglycemia, change in body mass index (BMI), and correlation between these parameters, observed with commonly used sulfonylureas in real-life clinical practice in India.
Research Design and Methods
Study setting
The OBSTACLE hypoglycemia study was a multicenter, prospective study involving clinical chart review, laboratory assessment, and a hypoglycemia questionnaire survey, conducted across 33 diabetes care clinics (see Appendix) from 18 cities of varying sizes, spread across 13 states and representing all zones of India.
Patient population
Patients of either gender with T2DM, between 18 and 75 years old and requiring addition of a sulfonylurea to an ongoing regimen of an oral antihyperglycemic agent or agents, were enrolled in the study. Patients who received insulin, sulfonylurea, or meglitinide in the 6 months preceding enrollment and those receiving dipeptidyl peptidase-4 inhibitors were excluded.
Study procedures
Consecutive patients meeting selection criteria and consenting to participate were enrolled by the treating physicians (study investigators) in this study. At enrollment, drug and dosage of sulfonylurea being initiated as per usual practice of investigator were recorded, along with baseline measurements of glycosylated hemoglobin (HbA1c) and BMI. Study patients were instructed to visit the physician for follow-up after 12 weeks. At the follow-up visit, repeat measurements of HbA1c and BMI were made and recorded, and the study investigator administered the Stanford Hypoglycemia Questionnaire in the most appropriate language to each patient. The Stanford Hypoglycemia Questionnaire, originally developed and validated in the Spanish language, is a patient-friendly tool that helps score hypoglycemia on the basis of presence or absence of seven common symptoms within a recall period of 1 week. Scores on this scale can range from 0 to 7, with a higher score indicating more hypoglycemia symptoms. For the purpose of this study, the questionnaire was made available in 11 languages (Hindi, English, Urdu, Punjabi, Oriya, Tamil, Telugu, Malayalam, Kannada, Marathi, and Gujarati). Patients reporting at least one of the any seven symptoms were considered to have experienced hypoglycemia. These episodes were further classified as mild (little or no interruption of activities and no assistance needed to manage symptoms), moderate (some interruption of activities and no assistance needed to manage symptoms), or severe (needed the assistance of others to manage symptoms or required medical assistance).
Outcomes
The primary objective of this study was to assess correlation between glycemic control (as measured by HbA1c) and hypoglycemia symptom score (as measured by Stanford Hypoglycemia Questionnaire) in patients with T2DM, 12 weeks after addition of a sulfonylurea to an ongoing regimen of an oral hypoglycemic agent or agents. The outcomes of interest of this post hoc analysis were (1) usage pattern of different sulfonylureas, (2) change from baseline in HbA1c levels and BMI, (3) hypoglycemia scores, and (4) correlation between (a) HbA1c level change from baseline and BMI change from baseline, (b) hypoglycemia score and change in BMI, and (c) hypoglycemia score and daily dose of sulfonylurea.
Statistical methods
Correlation analysis between HbA1c and hypoglycemic scores was performed based on Pearson's correlation coefficient. Correlation analysis was performed for multiple end points. All statistical hypothesis tests were performed at the 5% level of significance (two-sided test). Statistical analysis was performed for all enrolled patients. All statistical analyses were performed using SAS® version 9.2 for Windows (SAS Institute Inc., Cary, NC).
Sample size calculation
The study was powered to test the primary hypothesis of a positive correlation between improved glycemic control and hypoglycemia symptom score. Keeping the considerations of 0.70 as the anticipated sample correlation, 0.74–0.66 as the population correlation, 5% level of significance, and 80% power for a two-sided hypothesis, a sample size of 1,138 patients was considered adequate.
Ethical approval
The study was conducted in accordance with the principles enunciated in the Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Patients, revised at the 59th World Medical Association General Assembly, Seoul, Korea, 2008) and the 2006 Ethical Guidelines for Biomedical Research on Human Participants of the Indian Council of Medical Research.
All study documents were prepared, formatted, and submitted for review and approval by a central independent ethics committee.
Results
In total, 1,069 patients were enrolled in the study, with enrollment per center ranging from 10 to 52 patients. Of the enrolled patients, 984 patients returned for the follow-up visit, and 950 were considered as the “evaluable population.” The population of all enrolled patients who completed the study and had the values for HbA1c at Week 12 and hypoglycemia score without any major protocol deviation was considered as evaluable. Figure 1 presents the patient disposition in the study.
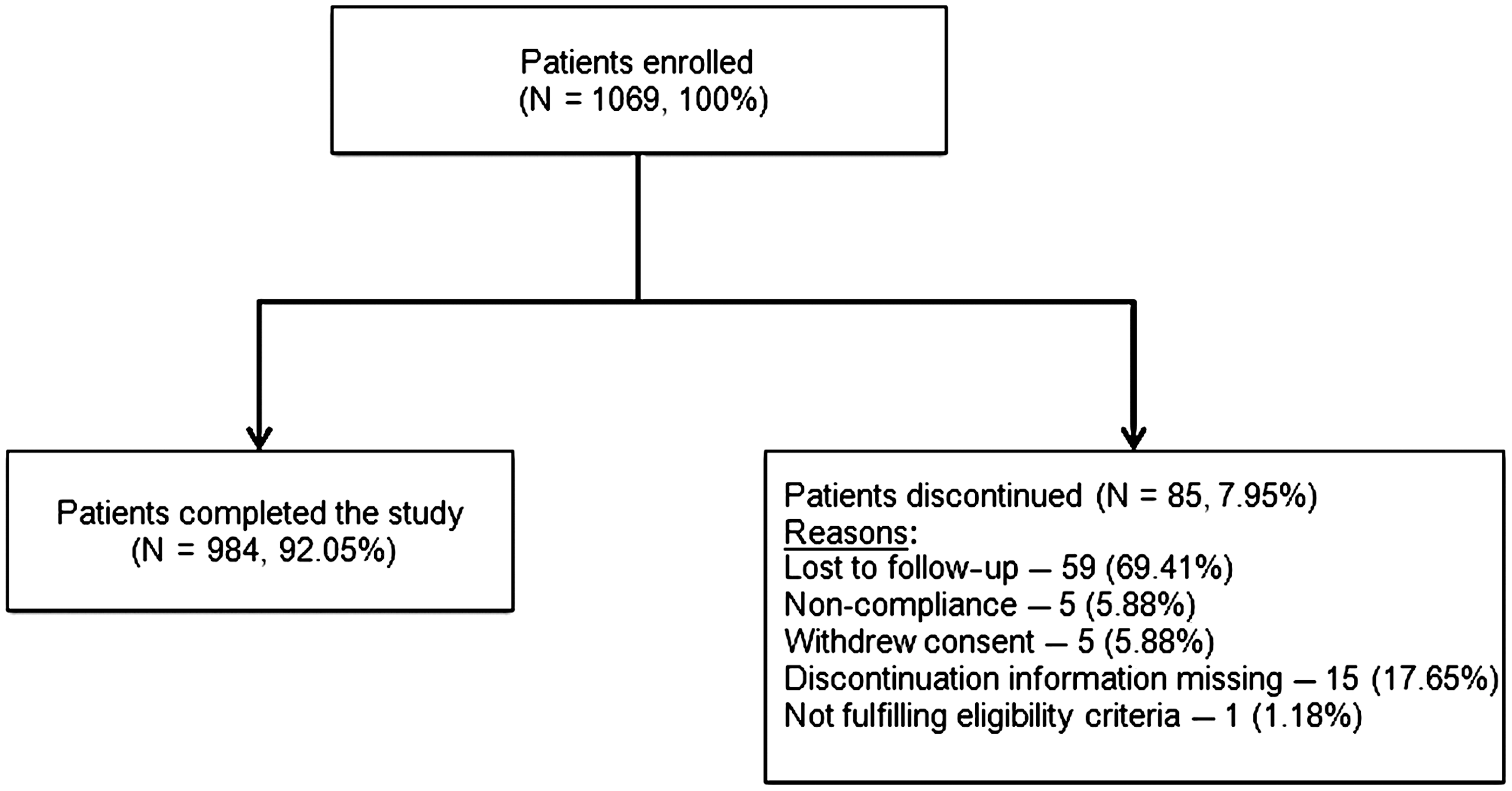
Patient disposition.
Baseline characteristics
Baseline characteristics of all enrolled patients are shown in Table 1. The mean age of the patients was 52.2 years and ranged from 19 to 80 years. The mean BMI was 26.37 kg/m2 and ranged from 14.2 to 45.5 kg/m2. Most of the included patients were recently diagnosed with diabetes, with mean duration of diabetes being 3.8 years. The mean duration of follow-up was 14.34 weeks. The mean baseline HbA1c observed in the study was 8.94%, ranging from 4.80% to 17.90%.
For one subject, age was missing; for eight subjects, gender data were missing; for six subjects, height data were missing; for six subjects, body mass index (BMI) data were missing; for 28 subjects, duration of diabetes information was missing; and for 54 subjects baseline glycosylated hemoglobin (HbA1c) data were missing.
Usage pattern
Glimepiride was the most commonly prescribed sulfonylurea (75.3%), followed by gliclazide (12.8%), glibenclamide (8.7%), and glipizide (2.4%). Sulfonylurea was initiated at low doses as evident from the mean and median doses for all four agents (Fig. 2). Metformin was the most commonly used (90.27%) background oral hypoglycemic therapy.
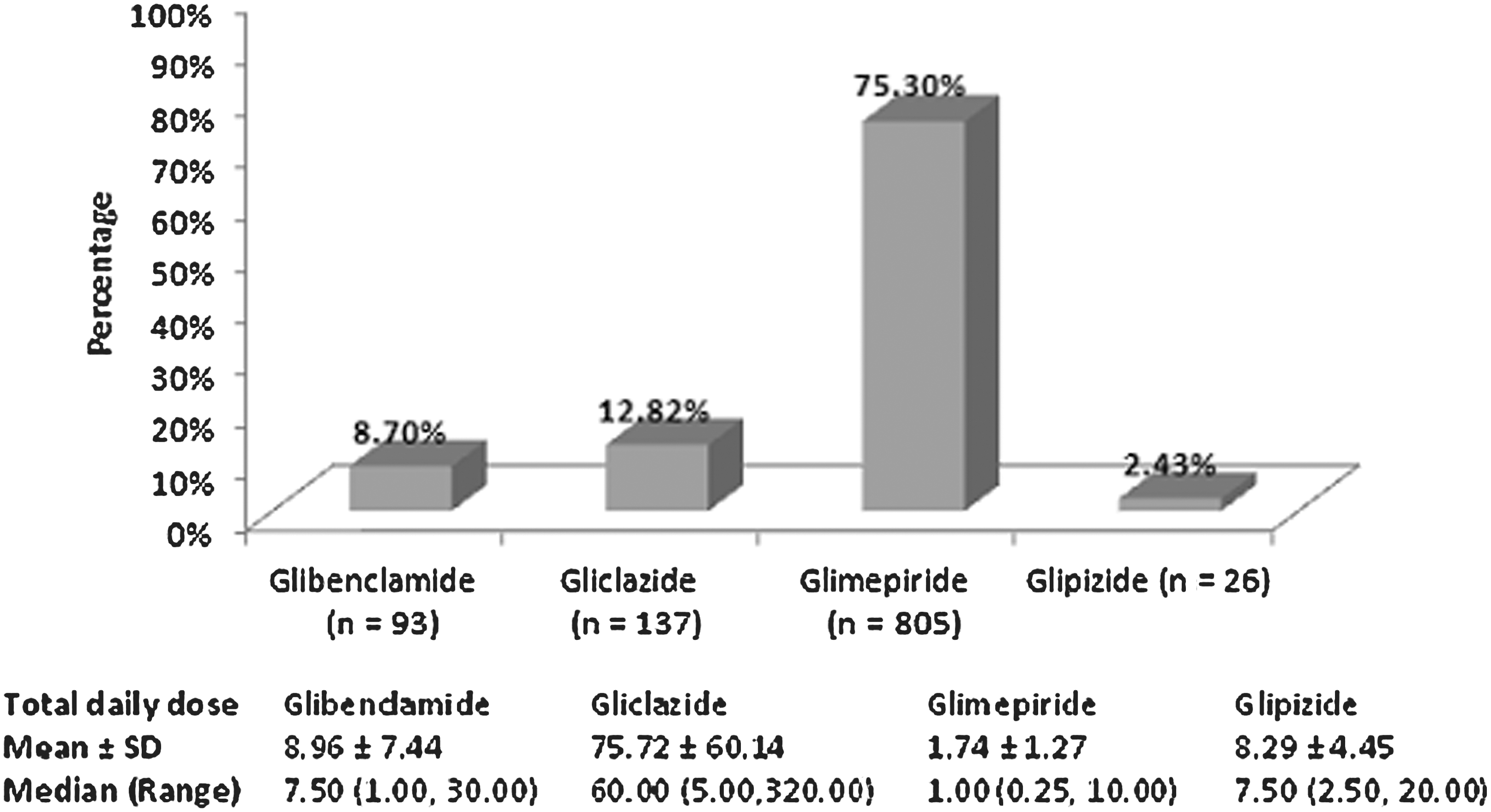
Usage pattern of sulfonylureas.
Change from baseline in HbA1c levels and BMI
The mean changes in HbA1c level and BMI are reported in Table 2. The mean change in HbA1c level was −1.31±2.43% from a baseline of 9.66±2.37% in the glibenclamide group, −0.99±2.03% from a baseline of 8.74±2.26% in the glipizide group, −0.83±2.27% from a baseline of 8.89±2.20% in the glimepiride group, and −0.72±2.25% from a baseline of 8.35±2.27% in the gliclazide group. The increase in BMI was highest in the gliclazide group (0.23±0.59 kg/m2), followed by the glibenclamide (0.14±1.01 kg/m2), glimepiride (0.12±0.77 kg/m2), and glipizide (0.04±0.98 kg/m2) groups.
BMI, body mass index; HbA1c, glycosylated hemoglobin.
Hypoglycemia
Proportions of patients reporting hypoglycemia episodes in different sulfonylurea treatment groups are described in Table 3. The mean hypoglycemia score for the study cohort was 0.98±1.42 (Table 4). The majority (n=557, 58.63%) of patients had hypoglycemia score of 0, followed by 129 patients (13.58%) with a hypoglycemia score of 1 and 95 (10.00%) patients each with a hypoglycemia score of 3 and 4. Only five patients (0.53%) had the highest observed hypoglycemia score of 6. The mean hypoglycemia score was highest in the gliclazide group (1.30±1.58), followed by the glibenclamide group (1.00±1.41). The glipizide cohort had the lowest hypoglycemia scores (Table 5).
Patient numbers in each subgroup were considered as the denominator for calculating percentages.
BMI, body mass index.
Correlation coefficient
For the evaluable population, no statistically significant correlation (r=0.04; P=0.2586) was observed between change in HbA1c level and change in BMI (Table 2). Correlation between change in HbA1c level and change in BMI was evaluated separately for all four sulfonylureas. There was no statistical or clinically significant correlation observed in any of the subgroups.
A weak negative, statistically significant correlation (r=−0.093; P=0.0044) between hypoglycemic scores at the follow-up visit and increase in BMI was observed (Table 4). Only the glimepiride group had enough patients to draw a meaningful correlation between the sulfonylurea dose and hypoglycemia score. A weak positive and statistically significant correlation (r=0.098; P=0.0082) was observed for glimepiride, between its dose and the hypoglycemia score (Table 5).
Discussion
Given the facts that India has a large burden of patients with T2DM 1 and that sulfonylureas are used extensively by Indian physicians for its management, as either first- or second-line agents, 5 –9 the potential implications of emerging safety concerns with sulfonylureas can be overwhelming in this country. However, there is a paucity of data on safety of sulfonylureas in real-life clinical practice in India. Furthermore, it is also known that different compounds within the sulfonylurea class differ in their clinical effects like glycemic efficacy, risk of hypoglycemia, and tendency to gain weight. 11 These differences might have an influence on the choice and dosing of sulfonylureas in clinical practice.
In our study, glimepiride emerged to be the most commonly prescribed sulfonylurea compound. It has a shorter plasma half-life and rapid renal elimination, both of which reduce the risk of hypoglycemia. 12 However, this higher acceptance of glimepiride among diabetes care physicians in India cannot be explained solely on the basis of its clinicopharmacological properties. Glipizide, which has a still shorter plasma half-life, 12 was the least commonly prescribed sulfonylurea in our study. Other pharmacological properties that differentiate glimepiride are its high affinity to the sulfonylurea receptor and rapid onset of action. However, neither of these is likely to provide any clinical advantage during long-term therapy (steady state), apart from reduced risk of drug–drug interactions. 11
In our study, all initiating dose of all the sulfonylureas were low. This practice is very much in line with general prescribing instructions for this class of drug and also with the practice guidelines. 4 Initiating sulfonylureas at low doses and up-titrating it gradually based on the glycemic response are known to minimize the risk of hypoglycemia. In our study as well, there was a positive, statistically significant correlation between dosage and hypoglycemia symptom score among patients receiving glimepiride (the only group having a sizeable population), reinforcing the supposition that sulfonylurea-induced hypoglycemia is dose related.
Weight gain with sulfonylureas is known to be primarily due to reduction of glycosuria and increased calorie intake to prevent or treat hypoglycemia. 13 In our study, we observed a negative, statistically significant correlation between increase in BMI and hypoglycemia scores. Although we did not measure glycosuria in our study, we could not establish any correlation between improved glycemic control (change in HbA1c level) and weight gain associated with sulfonylureas.
Although some important differences in clinical effects of different sulfonylurea compounds were noted in our study, because it was not designed and adequately powered to compare these, statistical evaluation of these differences was not performed.
In this study, it is important to note that almost half of the patients receiving sulfonylurea reported symptomatic hypoglycemia. The facts that initiation of sulfonylurea was the trigger for enrollment in this study and that experience of hypoglycemia is likely to be highest during initial weeks of sulfonylurea therapy could explain this high prevalence of hypoglycemia in our study. Considering that mean duration of diabetes in study patients was short and that risk of hypoglycemia is known to increase with disease duration, the proportion of patients experiencing hypoglycemia in real life could be still higher. In light of emerging findings on possible implications of recurrent hypoglycemia episodes, it is imperative to reconsider national treatment guidelines for T2DM in India, particularly in addressing the regimen for intensification. Hypoglycemia has been considered as the most important limiting factor in the glycemic management of patients with diabetes and a significant barrier in terms of adherence to medication and achievement of the life-long goal to attain euglycemia. 14
It has further been suggested that the presence (or fear) of hypoglycemia can limit the aggressiveness of drug therapy to achieve reduction of micro- and macrovascular complications, decrease adherence to diet, and reduce patients' willingness to take medications as directed. 14 Additionally, hypoglycemia causes recurrent morbidity in many patients with T2DM, worsens their quality of life, and is sometimes fatal. 15 It also impairs defenses against subsequent hypoglycemia because of autonomic failure (hypoglycemia-associated autonomic failure) and has even been causally linked to neurocognitive deterioration and detrimental changes in cardiac electrophysiology. 15
The revised guidelines need to describe pharmacokinetic differences between different sulfonylurea compounds and suggest newer, safer treatment alternatives like thiazolidinediones, dipeptidyl peptidase-4 inhibitors, α-glucosidase inhibitors, etc., so as to help treating physicians take a more informed decision. Also, the revised guidelines should put particular emphasis on a collaborative decision-making process between patients and the treating physician, during which all the available treatment options, along with their pros and cons, are discussed, and patients are educated on steps to minimize risk of hypoglycemia and weight gain. Guidelines may also encourage routine use of simple tools, for instance, the Stanford Hypoglycemia Questionnaire, to monitor undesirable effects of diabetes medications.
The results of this study are of interest not only because of its large size and geographical spread, but also because it provides the first preliminary clinical evidence of a correlation between hypoglycemia and weight gain.
Although this study was large, nationwide, and multicentric and conducted in real-life practice, some of its potential limitations that should be considered while interpreting its results are its observational, uncontrolled design and the fact that hypoglycemia episodes were not confirmed with blood glucose measurements. Furthermore, the fact that the Stanford Hypoglycemia Questionnaire was not administered at baseline may also be considered as a limitation. This step was excluded because patients on therapy with insulin or an insulin secretagogue (sulfonylureas or meglitinides) at the time of enrollment were not included, and they were considered not likely to experience hypoglycemia.
Our findings suggest that individual sulfonylurea agents differ in their effect on glycemic control, tendency to cause hypoglycemia, and weight gain. Hypoglycemia caused by these agents appears not only to be dose related but also correlates inversely with gain in BMI.
Appendix
The following investigators (with their corresponding sites in India) participated in this study: Dr. Sanjay Kalra, Karnal, Haryana; Dr. M.C. Deepak, Chennai, Tamil Nadu; Dr. A.P. Singh, Amritsar, Punjab; Dr. Sanjay Gupta, Delhi; Dr. Anuj Maheshwari, Lucknow, Uttar Pradesh; Dr. Pankaj Agarwal, Ghaziabad, Uttar Pradesh; Dr. Rajeev Awasthi, Lucknow; Dr. Rishi Shukla, Kanpur, Uttar Pradesh; Dr. P.C. Patra, Orissa; Dr. G.C. Reddy, Hyderabad, Andhra Pradesh; Dr. G.M. Prasad, Bangalore, Karnataka; Dr. K.N. Manohar, Bangalore; Dr. Neeta Deshpande, Belgaum, Karnataka; Dr. S. Paramesh, Bangalore; Dr. Syed Javaz, Bangalore; Dr. D. Venugopala, Mangalore, Karnataka; Dr. Balamurugan, Coimbatore, Tamil Nadu; Dr. Sreejith N. Kumar, Trivandrum, Kerala; Dr. M.G. Uvaraj, Salem, Tamil Nadu; Dr. Vinod Kumar, Cherthala, Kerala; Dr. Pichumani, Chengalpet, Tamil Nadu; Dr. Ravindranath, Trichy, Tamil Nadu; Dr. S. Satyanarayana Murthy, Nellore, Tamil Nadu; Dr. Vamsie Mohan, Chennai; Dr. Anand Swaroop Menawat, Rajasthan; Dr. Vaishali Deshmukh, Pune, Maharashtra; Dr. Manoj Saluja, Kota, Rajasthan; Dr. Navneet Agarwal, Gwalior, Madhya Pradesh; Dr. Sachin Gupta, Bhopal, Madhya Pradesh; Dr. Sanjay K. Jain, Indore, Madhya Pradesh; Dr. Sunil Gupta, Nagpur, Maharashtra; Dr. V.K. Abichandani, Ahmadabad, Gujarat; and Dr. Vidyut Shah, Rajkot, Gujarat.
Footnotes
Acknowledgments
This study was sponsored by and the writing of the manuscript was supported by an unrestricted grant from MSD Pharmaceuticals Pvt. Ltd., India. We would like to thank Mahendra Rai and Dr. Sunita Nair, Capita India, for providing editorial support to the manuscript.
Author Disclosure Statement
S.K., M.C.D., M.G.U., and N.A. are clinicians based in India and were investigators for this study. They have received payments for their services for the current study and have also previously received payments for other scientific services provided to MSD Pharmaceuticals Pvt. Ltd., India. P.N. and V.S. are full-time employees of MSD.