
Abstract
Background:
Accumulation of advanced glycation end products (AGEs) in tissues is a major risk factor for diabetes-associated complications. Skin autofluorescence (SAF) values measured by a specific noninvasive approach (AGE Reader; DiagnOptics Technologies B.V., Gröningen, The Netherlands) reflect the overall AGE exposure in skin.
Subjects and Methods:
In 16 adolescents with type 1 diabetes (age range, 11–18 years) we tested the association between SAF measured with an AGE Reader and the presence of glucuronic acid, 3-indoxyl sulfate, 3-hydroxybutyrate, phenol sulfate, and pentosidine in skin tissue determined with desorption electrospray ionization mass spectrometry (DESI-MS). These compounds are implicated in long-term diabetes complications.
Results:
SAF values significantly correlated with levels of compounds measured by DESI-MS (r>0.9 and P<0.001 for each).
Conclusions:
The strong correlation between adolescents' SAF values measured with the AGE Reader and some glycation products measured with DESI-MS indicates that SAF values may be used as surrogate markers of skin exposure to glycemic end products in type 1 diabetes.
Background
The analytical validation of SAF has been performed by determination of collagen-linked fluorescence in skin biopsy samples. 7 These results suggested that SAF is significantly correlated with the levels of pentosidine, carboxymethyllysine, and carboxyethyllysine. Here we present our observations supporting the proposal that SAF is also associated with some other compounds (glucuronic acid, 3-indoxyl sulfate, 3-hydroxybutyrate, phenol sulfate, and pentosidine) possibly implicated in diabetes complications. We measured levels of these analytes with the desorption electrospray ionization mass spectrometry (DESI-MS) technique, a recently developed noninvasive method suitable for the semiquantitative analysis of substances present in skin. 8,9
Subjects and Methods
This pilot study enrolled 16 adolescents (median age, 17 years; range, 11–18 years) patients (Table 1) with type 1 diabetes at the First Department of Pediatrics, Semmelweis University, Budapest, Hungary, with various durations of diabetes. Patients were treated in accordance with relevant national guidelines; at the time of measurements, each of them had been stable in condition for at least 4 weeks. Exclusion criteria included the presence of any serious comorbidity and dermatological disorder (for example, local dermatitis, psoriasis, or pigmentation disorders). Each patient and his or her parent gave a written informed consent to participate. Each of the patient was self-reportedly a nonsmoker.
Data are presented as mean±SD values except as indicated.
Median (range) for patient age and urinary albumin excretion.
ABPM, ambulatory blood pressure monitoring; BMI, body mass index; HDL, high-density lipoprotein.
AGEs were quantified with a specific device designed for the determination of SAF values (AGE Reader; DiagnOptics Technologies B.V, Gröningen, The Netherlands). The manufacturer's instructions were strictly adhered to (excitation range, 300–420 nm; emission range, 420–600 nm). This method is sensitive only for fluorescent AGE products.
DESI-MS measurements were done after the skin was cleaned using only distilled water; no soap or alcohol solution was used. We measured the skin levels of glucuronic acid, 3-indoxyl sulfate, 3-hydroxybutyrate, phenol sulfate, and pentosidine. In brief, mass spectrometric spectra were obtained using a modified OmniSpray (Prosolia, Indianapolis, IN) ion source mounted on either an TSQ Quantum triple quadrupole mass spectrometer (Thermo Fisher Scientific, San Jose, CA) or an LTQ Orbitrap Discovery Fourier transform mass spectrometer (Thermo Fisher Scientific GmbH, Bremen, Germany). Mass spectrometric peaks were identified based on their accurate mass determined at 30,000 full width at half-maximum nominal mass resolution and tandem mass spectrometry product ion spectra. In measuring the same skin area of the same person five times, the analytical reproducibility of the DESI-MS technique is comparable to that of other semiquantitative techniques, and the relative SD of peak intensities is approximately 20%, whereas the relative SD of peak ratios is <8.
For statistical analysis, Pearson analysis was used to test the association between SAF and individual DESI-MS data. Multiple regression analysis was used to adjust the associations for individual clinical parameters.
Results
The correlation between SAF and DESI-MS (Table 2) values of glucuronic acid, 3-indoxyl sulfate, 3-hydroxybutyrate, phenol sulfate, and pentosidine levels was significant (P<0.0001). It remained significant after adjustment to age, duration of diabetes, glycated hemoglobin levels, and lipid status with multiple regression analysis. These results are presented in detail in Figure 1.
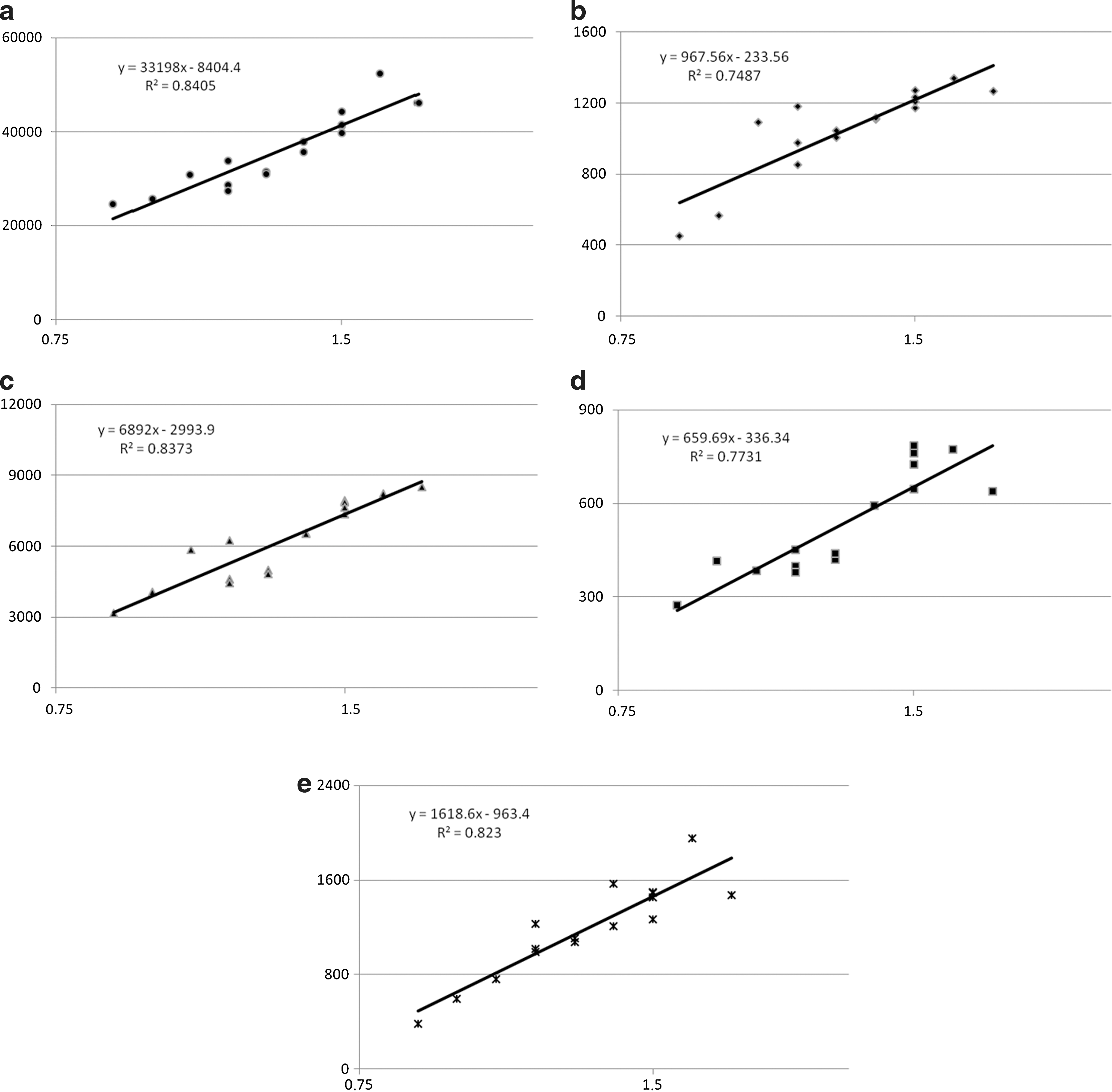
Association of desorption electrospray ionization mass spectrometry integrated ion signal intensity (vertical axis) with skin autofluorescence values (horizontal axis) for
CI, confidence interval.
Discussion
In this study we demonstrated a strong relationship between the relative mass spectrometric signal intensity of molecular ions of some selected compounds measured by DESI-MS and SAF in adolescents with type 1 DM. Previously each of these compounds was suggested as a possible contributor of diabetes complications. Of note is that heparane sulfate is composed of glucosamine and glucuronic acid disaccharides. The correlation between increased blood glucose level and urine heparanase suggests glucuronic acid as a predictive marker of diabetes complications. 10 Neuronal heparane sulfate proteoglycan plays a role in multiple microvascular diabetes complications. 11 According to recent results 3-indoxyl sulfate levels may be affected by alteration of metabolic pathways linked to kidney dysfunction. 12 Indoxyl sulfate modifies the balance between pro- and antioxidant mechanisms in endothelial cells contributing the thrombogenic state, 13 as it enhances proliferation of human aortic smooth muscle cells. 14
High triglyceride levels are important elements of cardiometabolic risk profile in patients with disturbed carbohydrate metabolism. 15 3-Hydroxybutyrate accumulates during ketotic conditions and may present a possible connection between subclinical dysglycemia and diabetes complications. 16 Volatile organic acid compounds like phenol sulfate in exhaled breath demonstrated the feasibility of accurately predicting blood glucose level. 17 Cresol sulfate has been found to be involved in cardiovascular disease and oxidative injury. 18 High levels of serum pentosidine are associated with arterial stiffness in diabetes patients. 19 The strong association with SAF may support the proposal that SAF may be used as a surrogate marker for the assessment of overall exposure to these agents. SAF has been reported to be an independent predictor of mortality in white hemodialysis patients. 20 In patients with diabetes and renal failure it is strongly and independently correlated with the progression of coronary heart disease. 21
It is important to emphasize that the measured mass spectrometric ion signal intensities provide only a semiquantitative estimation of the actual tissue levels. On the other hand, the lack of sample preparation allows the direct, noninvasive investigation of human skin, resulting in the strict detection of chemically labile species. As SAF values may be affected by clinical factors relatively prevalent in the adult population (hepatobiliary disorders with hyperbilirubinemia, connective tissue diseases, smoking), we aimed to enroll a pediatric diabetes population presumedly without apparent cardiovascular diseases, renal failure, and smoking.
The most important limitation of this study is the low number of patients. We believed, however, that this sample size was sufficient to assess the suitability of SAF values to gain some information on glycemic products in the skin of diabetes subjects. The strong association between DESI-MS and SAF even in this small sample size, however, demonstrates convincingly that SAF may be used as a surrogate marker for glycemic end product exposure of the skin. The usefulness of SAF in the evaluation of clinical conditions should be confirmed by further studies done on an appropriate number of patients.
Conclusions
Our present study indicates a strong concordance between SAF values and tissue exposure of several glycemic products, like glucuronic acid, 3-indoxyl sulfate, 3-hydroxybutyrate, phenol sulfate, and pentosidine, in adolescents with type 1 DM without significant comorbidity. This suggests that SAF values may be used as reliable surrogate markers for these analytes.
Footnotes
Acknowledgments
This project was done with the support of 17/2 PhD Programme at Semmelweis University.
Author Disclosure Statement
No competing financial interests exist.