
Abstract
Background:
“Psychological insulin resistance” (PIR) is an obstacle to insulin treatment in type 2 diabetes, and patients' expectations regarding alternative ways of insulin delivery are poorly understood.
Subjects and Methods:
PIR and beliefs regarding treatment alternatives were analyzed in patients with type 2 diabetes (n=532; mean glycated hemoglobin, 68±12 mmol/mol [8.34±1.5%]) comparing oral antidiabetes treatment, subcutaneous insulin injections, or inhaled insulin. Questionnaires were used to assess barriers to insulin treatment (BIT), generic and diabetes-specific quality of life (Short Form 36 and Problem Areas in Diabetes, German version), diabetes knowledge, locus of control (Questionnaire for the Assessment of Diabetes-Specific Locus of Control, in German), coping styles (Freiburg Questionnaire of Illness Coping, 15-Items Short Form), self-esteem (Rosenberg Self-Esteem Scale, German version), and mental disorders (Patient Health Questionnaire, German version). Patients discussed treatment optimization options with a physician and were asked to make a choice about future diabetes therapy options in a two-step treatment choice scenario. Step 1 included oral antidiabetes drugs or subcutaneous insulin injection (SCI). Step 2 included an additional treatment alternative of inhaled insulin (INH). Subgroups were analyzed according to their treatment choice.
Results:
Most patients perceived their own diabetes-related behavior as active, problem-focused, internally controlled, and oriented toward their doctors' recommendations, although their diabetes knowledge was limited. In Step 1, rejection of the recommended insulin was 82%, and in Step 2, it was 57%. Fear of hypoglycemia was the most important barrier to insulin treatment. Patients choosing INH (versus SCI) scored higher regarding fear of injection, expected hardship from insulin therapy, and BIT-Sumscore.
Conclusions:
The acceptance of insulin is very low in type 2 diabetes patients. The option to inhale insulin increases the acceptability for some but not the majority of patients.
Introduction
To investigate psychological barriers to the initiation of an insulin treatment, questionnaires were developed and validated. 6,9 Although studies regarding PIR reported some interesting results, only a few of them used validated psychometric instruments, 7,10 whereas others used nonvalidated questionnaires or interviews. 11,12
It is quite evident that the negative treatment preferences of patients regarding insulin might be influenced by the view of insulin as a potential threat or burden when different treatment options are discussed. As a potential solution to this problem more recent studies investigated the effects of inhaled insulin (INH) on the patients' acceptance of insulin treatment. These studies suggested that the INH treatment option leads to an increased acceptance of insulin treatment. 13,14 If INH treatment was available, this option was the most preferred treatment option compared with no treatment change, oral medication, and standard insulin treatment. 13 But so far, to our knowledge, no study has systematically investigated the beliefs of type 2 diabetes patients who fail oral medication regarding different treatment options and the corresponding psychological barriers to treatments. Understanding the specific reasons why patients refuse a potential life-prolonging treatment is essential when considering different ways of overcoming obstacles to a rational decision regarding treatment.
The data were collected already in 2005, and we intended to publish the results in 2008. But, because the first inhalable insulin was withdrawn from the market, this article was not published. Now that new inhalable insulin devices are on their way and rising numbers of publications focus again on this topic, we think that our results are still of importance, and we decided to publish them now.
The aims of this study were the following: (1) to determine the psychological status and psychological barriers to insulin treatment of type 2 diabetes patients who fail oral antidiabetes drug (OAD) treatment; (2) to assess treatment-related beliefs of these patients when comparing the different options—OAD, subcutaneous insulin injection (SCI), or INH; and (3) to analyze psychosocial status and psychological barriers to insulin treatment in subgroups of patients according to their favored treatment option.
Subjects and Methods
Patients
The study was conducted in 2005 in 20 primary care practices nationwide all over Germany after approval by all responsible ethical review boards. Written, informed consent was obtained from all patients participating in this study. We included 532 type 2 diabetes outpatients who had a glycated hemoglobin (HbA1c) level that suggested the necessity of more intensive therapeutic interventions, including insulin treatment. Inclusionary criteria were the following: type 2 diabetes treated only with diet and/or OAD treatment, a stable treatment regimen for at least 6 months, age between 18 and 70 years, insufficient oral antidiabetes treatment defined as HbA1c >69 mmol/mol (8.5%) (treated with diet alone), HbA1c >64 mmol/mol (8.0%) (one OAD), or HbA1c ≥58 mmol/mol (7.5%) (two or more OADs).
Study design
The design of this cross-sectional study (Fig. 1) included an examination of the current medical and psychological status of the sample, including psychological barriers to insulin treatment. The second part of the study consisted of a two-step treatment choice scenario, wherein participants discussed optimization options with a physician and were asked to make a choice about future diabetes therapy options: in the first step, the physician recommended insulin treatment because of the failing OAD medication. The options were to continue with OADs or to move on to SCI. The physicians were instructed and trained to adopt a strictly objective attitude while delivering the information. He or she read aloud an information text about diabetes and the treatment options using OADs or SCI. Additionally, two pictures were displayed to compare an OAD blister and a life-size insulin pen. This was completed by a summary of written information on prod and cons regarding the different options as follows: • Advantages of OAD: no blood glucose testing needed, easy to take, easy dosage. • Possible disadvantages of OAD: less accurate dosage maybe with a less accurate blood glucose control, risk of hypoglycemia (with sulfonylureas), possible weight gain, risk of multiple side effects, loss of appetite, edema in the legs (with pioglitazone), slow onset of effect, usually with decreasing effects during the course of therapy. • Advantages of SCI: precise dosage (insulin units can be delivered accurately), immediate effect, maintained effects during therapy. • Possible disadvantages of SCI: risk of hypoglycemia, insulin must be delivered with injections, regular blood glucose monitoring necessary, possible weight gain.
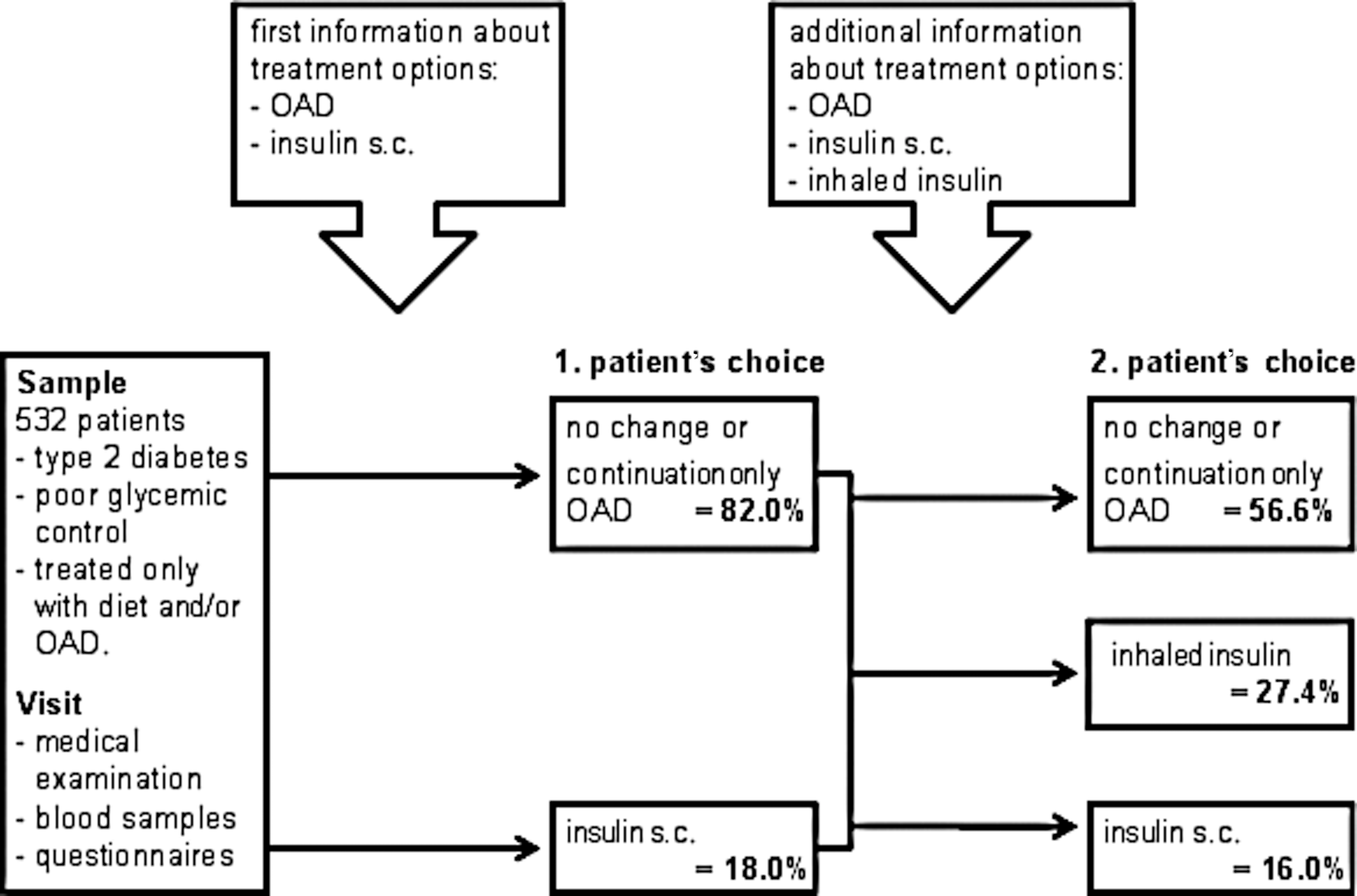
Study design and treatment choice of type 2 diabetes patients who were failing oral diabetes drug (OAD) treatment. s.c., subcutaneous.
Patients were given the opportunity to ask questions if they needed more explanations to understand the topics.
Following these explanations and recommendations, patients were asked which of the therapy options they would choose if they had to change their treatment now.
In the second step, patients again were informed about treatments, now including INH as an additional option. Again, an information text regarding INH was read aloud by the physician, and then a life-size picture of the inhaler for INH (Exubera® inhaler; licensed from Nektar; distributed by Pfizer Inc., New York, NY) was displayed. The written pros and cons for INH were delivered as follows: • Advantages: inhaled delivery instead of injections, precise dosage (insulin units can be delivered accurately), immediate effect, maintained effects during therapy. • Possible disadvantages: risk of hypoglycemia, possible weight gain, temporary coughing, changes in lung function (to be evaluated in long-term studies), slow-acting insulin (SCI) or OAD might be recommended additionally, regular blood glucose monitoring necessary.
Afterward, patients were asked for the second time which of the therapy options they would choose if they had to change their treatment now.
Psychological measures
Health-related quality of life was assessed by the German version of the Short Form 36 (SF-36). 15 Diabetes-related distress was measured using the German version of the Problem Areas in Diabetes (PAID). 16 Diabetes-related knowledge was assessed using the German Diabetes Knowledge Test. 17 PIR was assessed using the “Barriers to Insulin Treatment Questionnaire” (BIT) 6 with a sum score and the following subscales: Fear of injection and self-testing, Expectations regarding positive insulin-related outcomes, Expected hardship from insulin treatment, Stigmatization by insulin injection, and Fear of hypoglycemia. Coping styles were assessed using the Freiburg Questionnaire of Illness Coping, 15-Items Short Form, 18 with the following subscales: Active coping, Depressive coping, Distraction, Trivializing, and Doctor orientation/adherence. Diabetes-specific locus of control was assessed using the German Questionnaire for the Assessment of Diabetes-Specific Locus of Control (IPC-D), 19 with the following subscales: Internality (diabetes outcome depends on own efforts), Powerful others (outcome depends on behavior of healthcare providers), Chance (outcome depends on chance), and Unpredictability (outcome is not foreseeable). Self-esteem was measured by the German version of the Rosenberg Self-Esteem Scale. 20 Depression and anxiety disorders were assessed with the German version of the Patient Health Questionnaire. 21
Statistical analysis
Descriptive statistics were used to describe the psychological and medical status of the sample. As the subgroup of patients treated solely with diet or exercise was very small (5.3%, n=28), we merged the two treatment decision options A (no change of current treatment) and B (only oral medication) together into one group of oral medication choice for the analysis. The proportions of patients who chose the different treatment options were presented and analyzed using χ2 tests. Differences between subgroups in the theoretical treatment choice scenario were analyzed with χ2 tests for categorical variables. For continuous variables, analyses between subgroups were performed using t tests when the choice included two options and one-way analyses of variance for the comparison that included three options. Effect sizes for the differences between groups were calculated using Cohen's d with pooled SD. 22 The level of statistical significance for all analyses was set at α=0.05. Statistical analyses were performed by use of SPSS version 12.0.1 software (SPSS Inc., Chicago, IL) and ClinTools 23 (for Cohen's d).
Results
Characteristics of type 2 diabetes patients who failed oral antidiabetes treatment (Table 1)
Sociodemographic and medical characteristics
A clear overrepresentation of male patients (67%) was observed, whereas the distribution of the other sociodemographic variables represents roughly the average of the German normal population. The majority of the sample (91.4%) was overweight, and the HbA1c level of the sample (mean, 68±12 mmol/mol [8.34±1.5%]) demonstrates the poor metabolic control of the patients. The most commonly prescribed drug was metformin (79.7%), followed by sulfonylurea drugs (58.1%) and thiazolidinedione (17.5%), whereas 5.3% of the patients were treated with diet and exercise alone. Table 1 gives diabetes-related complications.
Higher values indicated a higher manifestation of the variables.
BIT, Barriers to Insulin Treatment Questionnaire; FKV-15, Freiburg Questionnaire of Illness Coping, 15-Items Short Form; HbA1c, glycated hemoglobin; IPC-D, Questionnaire for the Assessment of Diabetes-Specific Locus of Control; PHQ, Patient Health Questionnaire.
Psychological barriers to insulin treatment
The most important barrier to insulin treatment was the fear of hypoglycemia, which was reported as a serious concern in this patient group. Expected hardship of insulin therapy and fear of stigmatization by injections were indicated as moderately severe problems. Finally, fear of injection and self-testing was reported to be only a relatively minor problem. Despite these negative attitudes regarding insulin, there was a strong positive expectation with respect to insulin as an effective medication.
Other psychological variables
The health-related quality of life (SF-36) of the whole sample was slightly reduced compared with the general population, and diabetes-specific burdens (PAID) were described as moderate. On average, only seven diabetes-related questions out of 14 were answered correctly in the diabetes knowledge test. When asked about their diabetes-related coping styles, most patients reported a strong tendency to adhere to their treating physician's recommendations and to be active and problem-focused. The highest values regarding the perceived locus of control of the patients were observed for Powerful others and Internality locus of control, and the self-esteem of the patients was reported as moderate to relatively high. Depression was prevalent in 10% of the sample, and 6.6% were affected by anxiety disorders.
Treatment choice of patients
In the first step of the treatment choice scenario, wherein the treatment options included SCI therapy versus diet or exclusively OAD, the vast majority of the patients (82%) opted for the currently failing treatments, whereas only 18% followed the doctor's recommendation for SCI.
In the second step, in which INH was offered as an additional treatment option, the proportion of patients who refused insulin treatment decreased to 56.6%, and the acceptance of insulin rose to 43.4% (16% SCI and 27.4% INH).
Analyses of subgroups of patients according to their treatment choice
Results of the variance analyses are presented in Table 2.
BIT, Barriers to Insulin Treatment Questionnaire; CI, confidence interval; FKV-15, Freiburg Questionnaire of Illness Coping, 15-Items Short Form; HbA1c, glycated hemoglobin; HRQoL, health-related quality of life; INH, inhaled insulin; IPC-D, Questionnaire for the Assessment of Diabetes-Specific Locus of Control; OAD, oral antidiabetes drug; PHQ, Patient Health Questionnaire; SCI, subcutaneous insulin.
d is Cohen's d; P is calculated with two-tailed significance.
Sociodemographic and medical variables
Patients did not differ significantly regarding sociodemographic variables when we compared the three subgroups in the second step of the treatment choice scenario. As the only significant difference regarding medical variables, patients who opted for SCI had a slightly higher HbA1c value compared with those patients who opted for OADs.
Psychological barriers to insulin treatment and other psychological variables
In comparison with patients who were willing to take SCI, patients who opted for diet/OADs perceived their diabetes as somewhat, but significantly less, predictable (IPC-D); they also reported significantly more barriers to insulin treatment (BIT). This result was the case for the total sum score of the BIT as well as for the fear of hypoglycemia, the anticipated hardship from insulin therapy, and the lower positive insulin-related outcome expectation. The magnitude of these differences was small to moderate. No significant differences regarding the fear of injection and self-testing or the expected stigmatization by insulin injections were observed when we compared patients who opted for SCI with those patients who preferred diet/OADs.
When the differences were analyzed among patients who opted for INH and those who opted for one of the other diabetes treatment options, the following differences were significant: Fear of injection and self-testing, Expected hardship from insulin therapy, and the total BIT-sum score were significantly and substantially higher, and the positive insulin-related outcome expectation was significantly lower, in patients who chose INH compared with those who were willing to take SCI. Patients who chose SCI reported a significantly but only slightly reduced physical quality of life compared with the two other subgroups. Regarding all other psychological variables, no significant differences were observed among the three treatment option subgroups.
Discussion
The current study aimed to understand the psychological barriers of insulin treatment assessing the PIR. Furthermore, the effects of an additional treatment option, INH, on acceptance of insulin treatment were investigated by comparing patients' treatment choice in a theoretical scenario in which the INH option was given in addition to OADs or SCI or not, respectively.
The most striking result of our study was the fact that despite the doctor's explanation and recommendation of SCI, only a small minority of the patients (18%) were willing to change their currently failing oral treatment, whereas 82% opted for the currently failing treatments. This result differs considerably from other studies investigating treatment preferences. In a sample of Bangladeshi patients living in London, about 20% of poorly controlled diabetes patients were unwilling to begin SCI despite counseling. 24 Other studies with insulin-naive type 2 diabetes patients also revealed lower proportions of unwillingness to take insulin. In these studies about 30% of patients were unwilling to take insulin. 7,25 In a recent transnational study, Polonsky et al. 8 reported that patients unwilling to take insulin were quite rare in the entire sample (17.2%) and especially in the German sample (7.9%).
These dissimilarities may be due to methodological issues; studies demonstrating lower PIR were conducted as online surveys using an existing consumer panel 8 or including participants who were asked to fill out a questionnaire during a conference 7,25 independently of the metabolic status of the patients. Others included very specific ethnic subgroups of patients, limitating the generalizability of the results. 24 In contrast, we included only patients with a currently failing OAD treatment who were asked about their willingness to switch to insulin after a discussion with their physician who explicitly recommended this change. This situation with its high external validity might have activated the emotions and beliefs patients would have had in reality. Thus, the results of our study might represent an estimate of PIR that is closer to the real-life situation of patients.
The addition of INH as a treatment option increased the willingness to consider insulin therapy in our sample up to 43%; still, the majority of patients (57%) refused to take the recommended medication. These results are in accordance with previous studies of treatment preferences of poorly controlled diabetes patients. 13 In a study of type 2 diabetes patients the majority of patients (70%) treated with OADs would be reluctant to start SCI, but willingness to insulin therapy increased to about 83% with availability of INH. 9 Additionally, in a randomized controlled trial the availability of INH affected the acceptability of insulin treatment. In the group with INH as treatment option, 43.2% of patients opted for this treatment compared with 15.5% of patients who were offered standard therapies. 13
There are several possible reasons for the strong rejection of SCI. First, a remarkable ambivalence toward insulin was observed. On the one hand, patients in our study reported a very positive insulin-related outcome expectation. This result differs from the mostly negative expectations of diabetes patients in different countries. 5 On the other hand, negative attitudes toward insulin treatment were considerable and seemed to be more decisive for concrete behavior: in a ranking of different barriers to insulin treatment, the most important concern was fear of hypoglycemia, followed by expected hardship of insulin therapy and the fear of stigmatization by injections. It is interesting that fear of injection and self-testing was reported as a relatively small problem by the majority of the sample. These results are in accordance with another study in insulin-naive type 2 diabetes, which showed that fear of injections and injection-related pain were reported by about 40%, but these were less frequently mentioned than fear of hypoglycemia or restrictions due to insulin therapy. 7 In the above-mentioned transnational study, only 16.2% of patients endorsed a fear of injections which is similar to the present study. 8 Keeping in mind that both studies differed considerably regarding the willingness to insulin treatment, fear of injections as a commonly discussed barrier to insulin treatment in diabetes patients 26 seemed to be a serious concern only for a small subgroup of our patients and thus a weak predictor of treatment preferences.
Regarding the anticipated obstacles to the therapy alternatives, patients opting for OADs versus SCI reported more barriers to insulin treatment, but they did not differ in fear of injection and self-testing as would have been expected by results of other studies. 7,25 A recent study on INH and treatment preferences found that more frequent hyperglycemia, more poorly controlled diabetes, and more perceived treatment restrictions but not more negative beliefs about injections were associated with positive ratings of inhaled insulin. 14 In our sample differences in fear of injections and self-testing were only found in patients with a more positive attitude toward INH versus SCI, with patients choosing INH reporting more fear of injections and self-testing than those opting for SCI.
In the present study, patients with negative beliefs about SCI treatment reported significantly more barriers to insulin treatment and expected a lower positive insulin-related outcome. These findings are in line with the results of the transnational study by Polonsky et al., 8 in which unwilling patients reported significantly more negative and fewer positive beliefs about starting insulin treatment. Considering the glycemic control and decision making of the sample, most patients seemed to underestimate the severity of their prognosis. This finding is consistent with earlier results, where 24% of patients with longstanding type 2 diabetes thought that diabetes is a transient condition, and only 9% were aware of their reduced life expectancy. 27 Similar faulty estimation could be present in our study, too, as indicated by the relatively poor diabetes knowledge of the sample.
With regard to their diabetes, most patients perceived themselves as active and problem-focused, with a strong feeling of internal control and acceptance of the important role of their treating physicians. Finally, they reported a strong tendency to adhere to their treating physicians' recommendations. This outcome paints a somewhat surprising picture in light of the poor glycemic control and strong rejection of insulin despite the doctors' recommendations. These contradictory results may be explained partly by the interpretation that patients might think they follow their doctors' recommendations when in fact they don't. Misunderstandings during patient–doctor interactions are common, as indicated by a significant discrepancy between patients' and professionals' perceptions and recollections of the content of consultations. 28 Furthermore, “recommendations” are not identical to “collaborative goal setting,” which has been recognized as improving clinical outcomes 29 and includes an ongoing patient involvement in defining diabetes treatment goals and strategies.
As a limitation of our study, unrecognized selection biases might have occurred and affected our results in unknown ways. This is especially true for the application of our results to countries with a different sociocultural situation and/or with different healthcare systems. Therefore our findings might be limited to understanding the treatment preferences of patients in Germany or in similar European or Western countries. Also, the generalizability of our results is restricted to poorly controlled insulin-naive type 2 diabetes patients. Finally, we used a theoretical treatment choice scenario without offering an immediate change of treatment. Accordingly, the question remains as to whether the patients would have made the same choices in a real-life situation.
It also remains unclear if an initial treatment choice would be stable over time or change during the course of treatment.
In conclusion, PIR is a crucial point in type 2 diabetes patients who fail oral treatment. As this patient group often rejects the initiation of insulin treatment, the reasons for this behavior need to be explored for each patient, individually. INH might lower the barriers to insulin treatment for some patients but seems not to be a convincing solution for the majority. Patients might underestimate their poor prognosis because of a mixture of insufficient knowledge, overestimation of the quality of their own diabetes management, and communication deficits between doctors and patients.
Footnotes
Acknowledgments
This study was supported by Pfizer Pharma GmbH, Germany and Aventis Pharma Deutschland GmbH.
Author Disclosure Statement
E.S. was employed at Pfizer Germany up to 2008 and is currently an employee of ECHOconsult. F.P., A.P., and S.H. have no competing financial interests.