
Abstract
Objectives:
An optimized metabolic control during delivery is mandatory to prevent maternal–neonatal complications. The primary aim of this study was to evaluate the efficacy and safety of continuous subcutaneous insulin infusion (CSII) during delivery in pregnant women with type 1 diabetes. The secondary aim was to assess the impact of real-time continuous glucose monitoring (RT-CGM) added to CSII versus CSII alone.
Research Design and Methods:
This was a multicenter observational retrospective study. A standardized protocol, to use CSII throughout pregnancy and delivery, foresaw three different insulin basal rates according to blood glucose level: profile A, the last basal rate in use; profile B, preventive 50% reduction of the last basal rate in use; and profile C, 0.1–0.2 U/h for blood glucose level <70 mg/dL, activated just before anesthesia or at the beginning of active labor. An alternative intravenous protocol (IVP) was given in case of complications and relevant metabolic deterioration. Blood glucose in the target range (70–140 mg/dL) throughout delivery and percentage of activation of the IVP were primary outcomes.
Results:
Sixty-five pregnant women with diabetes included in the study (56–86% cesarean section; 9–14% spontaneous/stimulated vaginal delivery). Mean blood glucose level was 102±31 mg/dL at 0 min, 109±42 mg/dL at 30 min, 120±48 mg/dL at 60 min, and 99±34 mg/dL at 24 h. Mean basal rate during delivery was 0.6±0.4 U/h (profile B). Mean capillary blood glucose (CBG) level was lower in the RT-CGM group relative to the CSII-alone group: 80±14 mg/dL versus 111±32 mg/dL at 0 min (P<0.01), 79±11 mg/dL versus 109±42 mg/dL at 30 min (P<0.02), and 98±20 mg/dL versus 125±51 mg/dL at 60 min (difference not significant). Eleven newborns experienced transient neonatal hypoglycemia. None of the women switched to IVP. No major differences were observed according to delivery procedure.
Conclusions:
CSII is possible and safe in different types of delivery in selected and educated women. RT-CGM helps to obtain better outcomes in terms of maternal peripartum CBG level.
Background and Aim
Even if few articles are available on this topic in type 1 diabetes, 11,14,17 –21 they all agree that the glycemia profile during delivery can influence the maternal–fetal perinatal outcome. Stenninger et al. 14 demonstrated an association between maternal glucose concentration within 120 min of delivery and the occurrence of postnatal hypoglycemia or the need of intravenous glucose treatment in infants. Currently there is no general consensus on the optimal peripartum glycemia target values that can allow good perinatal outcomes. Ranges between 70 to 120 or 70 to 140 mg/dL 11,18 –20,22,23 seem to be the most accepted therapeutic goals. Few studies have investigated the usefulness of using new technologies, such as CSII (insulin pump) and/or CGM, during delivery to obtain a good intrapartum glycemia profile and a subsequent good maternal and fetal outcome. 14 –16
The present study derives from a common observation that most of the pregnant women with type 1 diabetes referred to our centers would like to maintain during delivery the same therapeutic technique (CSII) that they have learned for pregnancy. Moreover, the majority of them deliver in different obstetric clinics, which implement different patterns of care during and after delivery with various outcomes in terms of glycemic control. 21 This fact is more frequent after cesarean section (CS) when it is particularly difficult but necessary to maintain stable glycemic profiles because of fasting and pain in the postpartum period.
The primary aim of the study was to evaluate the efficacy and safety of CSII use according to a specifically designed protocol during and after delivery in pregnant women with type 1 diabetes who previously had used CSII throughout gestation and were trained to maintain target metabolic goals. 13,24,25 The secondary aim was to assess the impact on maternal–fetal metabolic outcome of real-time CGM (RT-CGM) in association with CSII (RT-CGM group) versus CSII alone (CSII group).
Subjects and Methods
This is a multicenter observational retrospective study involving four specialist centers that previously shared a standardized protocol for insulin pump use, with or without CGM, throughout pregnancy and delivery. From 2009 to 2011, 65 white women with type 1 diabetes were enrolled, for data collection and analysis; 26 of them (40%) were already on CSII before conception, whereas the remaining 39 (60%) switched to CSII during pregnancy (at 11±5.8 weeks of gestation on average). Thirteen (33%) of them were previously treated with basal-bolus insulin therapy with glargine insulin at bedtime, and the others were using different intensive multiple daily insulin regimens. Eighteen (27.7%) self-selected pregnant women used RT-CGM with a protocol that foresees a frequency of utilization of three times a month, at least, from the baseline visit to the end of pregnancy and delivery. (Fifteen of them used a sensor-augmented pump [Paradigm® REAL-Time or Paradigm VEO]; three used a Guardian® REAL-Time CGM system [all three from Medtronic, Northridge, CA]. Other types of insulin pumps in use were the Animas [West Chester, PA] IR 1200/2020 and the ACCU-chek® [Roche Diagnostics, Indianapolis, IN] Spirit. (No complete data are available on the method of accessing pump therapy because a significant number of women had come from other outpatient clinics and were followed up in our centers for pregnancy only. All patients used only short-acting insulin analogs (lispro/aspart) when CSII therapy was started. Baseline characteristics of the study population were similar in the two groups examined, except for the third trimester glycated hemoglobin (HbA1c), and are summarized in Table 1. In the subgroup of women who started CSII during pregnancy, the HbA1c level was 7.1±1.3% at therapy start and 6.6±1.5% at the third trimester (difference not significant). There were no significant differences in the third trimester HbA1c between this subgroup and either group.
P for comparison of the continuous subcutaneous insulin infusion (CSII) group versus the real-time continuous glucose monitoring (RT-CGM) group.
P<0.01, c P<0.001 for pregestational versus third trimester glycated hemoglobin (HbA1c).
BMI, body mass index; NS, not significant.
In agreement with our usual clinical practice, a written informed consent was obtained from all the women attending our outpatient offices at the first visit in pregnancy regarding an anonymous use of their clinical data, which was later confirmed after delivery, at the time of the last clinical and metabolic evaluation.
CSII protocol
Pregestational counseling and pregnancy management were usually implemented according to the Italian “Diabetes and Pregnancy” Study Group guidelines 26 and American Diabetes Association recommendations 24 in terms of content and frequency of examinations. Patients were also asked to follow the same guidelines in their home management with the following metabolic targets: HbA1c <6%, as determined by the high-performance liquid chromatography method (reference range, 4.3–6.1%) in the third trimester; and capillary blood glucose (CBG) of 70–90 mg/dL (3.8–5 mmol/L) at fasting and 140 mg/dL (7.7 mmol/L) and 120 mg/dL (6.6 mmol/L) at 1 and 2 h after a meal, respectively. Body mass index was calculated on the basis of reported pregestational weight and the height measured at the baseline visit.
On the occasion of their first visit at our outpatient clinics, all patients entered an education program designed to teach them how to achieve and maintain good metabolic control and to operate the pump properly (also RT-CGM if used) during pregnancy. From week 28 onward, patients and their partners (or other caregivers) received a specific weekly training for insulin pump management during delivery. Moreover, the same written instructions were sent to their obstetric teams, in order to ensure correct pump and RT-CGM use during and after delivery. Target glycemia values were 70–140 mg/dL. Within the end of gestation, patients were educated to set up the pump with three different insulin basal rates (IBRs), activating the single most appropriate one, according to the current CBG values: profile A, IBR in use; Profile B, 50% reduction of the total amount of profile A, distributed as a constant hourly rate for the whole 24-h period; or profile C, 0.1–0.2 U/h. Profile B consisted of a 70% reduction of profile A, in the case of very high-dose insulin-requiring patients during the second half of pregnancy, or of 30% reduction of profile A, in the case of very low-dose insulin-requiring subjects.
The standardized protocol is shown in Figure 1. Profile A corresponds to the basal rate used from each patient during the last few days before delivery, and it is advised, if CBG values are in the target range, that profile A be used throughout the whole first phase of the procedure, when there are minimal changes in maternal metabolic demand. From the beginning of active labor or immediately before anesthesia, the insulin requirement shortly afterward tends to rapidly decrease because of increased energy expenditure of cervical dilatation, in the case of vaginal deliveries and rapid changes in maternal hormone concentrations that occur soon after the extraction of the fetus. In this period, the insulin requirement halves at least or reaches almost zero, compared with the prepartum dosage; therefore the protocol foresees the activation of profile B or C, respectively (Fig. 1). In the case of CS and CBG level >140 mg/dL (7.8 mmol/L) immediately before anesthesia, profile A was maintained for 60 min after anesthesia, and profile B was activated after that. The protocol started at the time of admission in the case of CS or spontaneous labor (SL) versus 2 h after the intravaginal administration of prostaglandin in induced labor (IL). At that moment all patients were also infused with isotonic saline solution. In the case of planned deliveries, such as IL and elective CS, women were instructed to maintain the usual meal regimen and insulin dose on the day preceding the procedure. The subjects who used RT-CGM were advised to connect the sensor over the same period of time. All the elective CSs were performed in the morning with the woman under epidural anesthesia. The fasting regimen started at admission in the case of CS or SL and after an early morning breakfast with the usual bolus in those undergoing IL. At the time of admission, all the patients were taught to change the infusion set, to check urinary ketones, and to monitor CBG hourly. From the second stage of labor or performance of anesthesia, CBG was monitored every 30 min until delivery, and intravenous glucose (5–10% in the case of CS or vaginal delivery, respectively) was infused (Fig. 1). The glucose administration was started early in the case of a prolonged first phase of labor (>5 h) or persistent CBG value <70 mg/dL. In the postpartum period CBG was checked every 2 h, and 150 g/24 h of intravenous glucose was administered until the resumption of oral feeding.
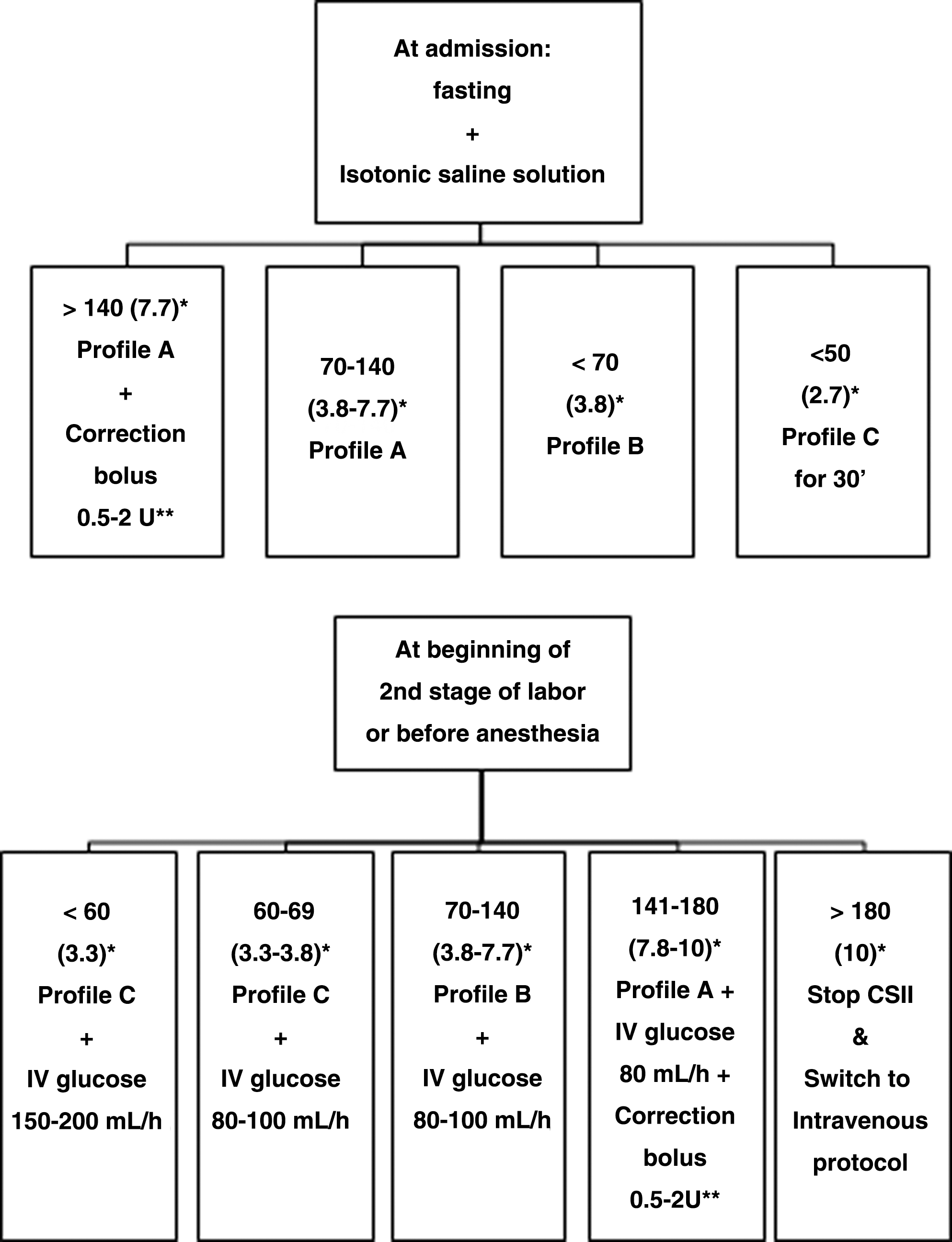
Insulin protocol applied to pregnant women with diabetes during labor and delivery. *Reference blood glucose thresholds expressed in mg/dL (mmol/L). **Correction bolus was calculated on the basis of the individual prepregnancy insulin sensitivity. CSII, continuous subcutaneous insulin infusion; IV, intravenous.
In the case of a noncompliant patient or obstetric team, in the presence of ketonuria and/or persistent hyperglycemia, defined as CBG >180 mg/dL (10 mmol/L) after two consecutive measurements and a corrective bolus, patients were switched from CSII to standardized intravenous insulin infusion (80 mL/h of 10% glucose±0–2 U/h of short-acting insulin) independently of the phase of the procedure. 11 In the case of maternal hypoglycemia (<50 mg/dL [2.7 mmol/L]), profile C was activated, or CSII was stopped for 30 min with 33% intravenous glucose being administered if deemed necessary. All mothers were encouraged to breastfeed as soon as possible. Additional oral feeding with formula was initiated 2 h postnatally and was continued every third hour thereafter. In asymptomatic infants, neonatal CBG was screened within 2–3 hours of birth and before each meal thereafter. Neonatal hypoglycemia was defined as follows: a glucose level of <36 mg/dL (<2 mmol/L), confirmed with plasma glucose measurement, despite an early oral feeding; or a glucose level of <45 mg/dL (2.5 mmol/L), in a symptomatic infant. The operational threshold for intravenous glucose treatment was 20–25 mg/dL (1.1–1.4 mmol/L). 28 Large for gestational age was defined on the basis of Italian standard curves of intrauterine growth. 29 Diabetes assistance was available by phone 24 h a day.
End points and statistical analysis
The efficacy of the protocol was assessed by maternal CBG values in the target range (70–140 mg/dL) in four specific moments (at admission, 0 min [immediately before anesthesia or at the beginning of the second stage of labor], 30 min, and 60 min) and by the frequency of neonatal hypoglycemia or cumulative respiratory disorders. 30 Safety of the protocol was assessed by the frequency of maternal hypoglycemia (CBG≤50 mg/dL [2.7 mmol/L]) throughout delivery and the number of women switching to the intravenous protocol (IVP).
Statistical analysis was performed by means of paired t test, unpaired t test, and χ2 test, as appropriate. A value of P<0.05 was considered statistically significant. All analyses were made with the statistical software package SPSS Windows (SPSS, Inc., Chicago, IL). Data are shown as mean±SD values unless otherwise specified. We evaluated the results in the whole population examined, and then we compared the data between the two subgroups, RT-CGM versus CSII.
Results
Maternal and fetal outcomes are shown in Table 2. Of 56 CSs, 16 (29%) were performed as emergency procedures. Five of 65 (7.7%) were SLs. Four of 65 (6.1%) were ILs. Sixteen of 65 (25%) were preterm deliveries (34.6±2 weeks), of which two (12.5%) occurred before week 34 of gestation and eight (50%) were spontaneous.
P for comparison of continuous subcutaneous insulin infusion (CSII) group versus real-time continuous glucose monitoring (RT-CGM) group.
IL, induced labor; LGA, large for gestational age; NS, not significant; SL, spontaneous labor.
In the case of vaginal deliveries, the lengths of the first and second stages of labor were 255±198 and 38±26 min, respectively, in SL versus 270±65 and 34±14 minutes in IL.
Mean maternal CBG level in the total population was 102±31 mg/dL at 0 min, 109±42 mg/dL at 30 min, and 120±48 mg/dL at 60 min, indicating the achievement of therapeutic goal at each time point considered. In particular, the goal at 0 min was achieved with a mean IBR (profile A) of 1.3±0.4 U/h (1.36±0.5 U/h in the CSII group; 1.2±0.5 U/h in the RT-CGM group; difference not significant), corresponding to 53% of the total daily dose, at the time of admission. After that, 56 patients activated profile B, which means 86% of the women were at target in that phase of delivery. At 30 min the IBR was additionally reduced with the activation of profile C in two SLs and four ILs. In these patients, profile C was maintained until the resumption of oral feeding that occurred 2 h after delivery, when they came back to profile B.
In women who underwent to CS (n=56), mean CBG value at 24 h after delivery was 99±34 mg/dL (5.5 mmol/L) with a mean IBR of 0.6±0.4 U/h; at 36 h, it was 107±36 mg/dL (5.9 mmol/L) with a mean IBR of 0.5±0.3 U/h. In these women, the resumption of oral feeding occurred after 51±18 h.
Mean CBG level was lower throughout the study in the RT-CGM group relative to the CSII-alone group: 80±14 mg/dL (4.4 mmol/L) versus 111±32 mg/dL (6.2 mmol/L) at 0 min (P<0.01), 79±11 mg/dL (4.4 mmol/L) versus 109±42 mg/dL (6 mmol/L) at 30 min (P<0.02), and 98±20 mg/dL (5.4 mmol/L) versus 125±51 mg/dL (6.9 mmol/L) at 60 min (difference not significant).
Table 3 shows CBG values and IBR variations in different stages according to modalities of delivery.
No statistically significant differences were showed between the different delivery modalities.
CBG, capillary blood glucose; IBR, insulin basal rate.
None of the mothers experienced hypoglycemia of <50 mg/dL during delivery or needed to be switched to IVP. Only one patient, who underwent CS, had hypoglycemia within the first 24 h after delivery, because of discontinued administration of intravenous glucose. No urinary ketones were found during any phase of the procedure secondary to any problem of the infusion set in all patients examined. Mean fetal CBG level in the total population at 3 h after birth was 48±19 mg/dL (46±2 mg/dL in the CSII group vs. 56±17 mg/dL in the RT-CGM group; difference not significant). Eleven newborns experienced neonatal hypoglycemia corresponding to a prevalence rate of 17% of deliveries; 10 episodes were reported in the CSII-alone group and just one in the RT-CGM group (difference not significant). All cases of neonatal hypoglycemia occurred in preterm deliveries; nine hypoglycemic episodes were definitively corrected within 3 h of birth with early oral feeding, whereas the remaining two episodes extended to 12 h and were corrected with intravenous glucose. Mean fetal CBG level at 12 h was 58±10 mg/dL (3.2 mmol/L) in the total population and 64±9 mg/dL (3.5 mmol/L) in the RT-CGM group (difference not significant). Cumulative respiratory disorders were recorded in nine (13.8%) newborns (two severe episodes, requiring oxygen in the first 24 h), of whom seven were in the CSII-alone group and two were in the RT-CGM group (difference not significant). None of the newborns had postnatal asphyxia (Apgar score of <5 at 5 min). Seven of the 65 mothers (10.7%) received antepartum administration of betamethasone in two intramuscular doses of 12 mg 24 h apart. 31 Neonatal intensive care unit admission occurred for eight of the 65 newborns (12%): seven in the CSII-alone group and one in the RT-GCM group (difference not significant).
Discussion
Our results demonstrate that CSII can be used efficiently and safely during delivery in well-trained, motivated patients. The efficacy of CSII is demonstrated by the maternal peripartum glycemic values, which remained stable and within the target range throughout the entire period in more than 80% of the women examined. Comparable and stable values were also seen in the group of women who underwent CS, who had been fasting at least for 2 days after delivery. Neonatal hypoglycemia occurred mainly within 3 h of birth and all in preterm deliveries, a well-known risk factor for this neonatal complication 32 ; moreover, the frequency of neonatal hypoglycemia recorded in the present study (17%) was comparable to that reported in other European studies. 20,33,34 We also recorded a low percentage of cumulative respiratory disorders in neonates. This last finding allowed the return to the ward and breastfeeding in the majority of newborns as demonstrated by the low percentage of neonatal intensive care unit admissions.
No mother needed to be switched to IVP, which testifies to the safety of the protocol. Moreover, we did not record any maternal intrapartum hypoglycemia or positive urinary ketones linked to problems of the set or site of infusion.
As additional data, all patients improved their metabolic control, as evidenced by a significantly better HbA1c at the end of gestation in comparison with the last measurement before pregnancy, with best results obtained in patients who also used RT-CGM. In our opinion, such improvement of HbA1c helped us to achieve good results in terms of peripartum CBG values, as shown elsewhere. 14
These data prompt the following additional considerations. In our population, only 24 women planned their pregnancies, and only 25 were already using the pump before pregnancy. The remaining 39 women started CSII at the end of the second month on average, showing a fast and efficient adaptation to their new therapy as demonstrated by the improvement of the third trimester HbA1c level, even if not statistically significant. These results clearly indicate that CSII is effective and safe even in unplanned pregnancies and in women who start CSII during gestation, allowing us to judge them suitable for the implementation of our peripartum protocol. The patients' high motivation derived from the gestational condition is certainly one of the major determinants of these positive outcomes, as is usually seen in many studies and clinical practice. Nevertheless, the implementation of a dedicated structured training program covering general management of pregnancy and specific use of the insulin pump throughout gestation, partum, and postpartum was crucial to reach the treatment goals. According to international consensus, we still consider the preconception counseling an essential step to minimize the risk of adverse outcomes in pregnancies complicated by diabetes, and we strongly believe that further efforts should be made in order to increase the number of planned pregnancies.
Nonetheless, based on results of the present experience, we agree with those results emerging from other studies 35 on the efficacy of structured education in reaching good metabolic targets even in unplanned pregnancies.
The analysis of the RT-CGM group shows promise for this intervention, although the low number of treated women and the self-selection criteria for its use prevent us from drawing definitive conclusions. Our data in fact showed that RT-CGM in combination with an insulin pump was more effective in reaching therapeutic targets with respect to CSII plus self-monitoring of blood glucose. Starting from comparable baseline metabolic characteristics, women who used RT-CGM showed better outcomes in terms of third trimester HbA1c levels, maternal peripartum CBG, neonatal hypoglycemia, and respiratory disorders, although these last two findings did not reach statistical significance. Our findings on the efficacy of RT-CGM to improve some metabolic targets or adverse outcomes of pregnancy (HbA1c levels, maternal peripartum CBG, neonatal hypoglycemia, etc.) are in line with those of other studies 8 –10,14 except for birth weight and percentage of large for gestational age, which in our results were similar in both groups. This last finding could be linked to a greater maternal weight gain observed in the RT-CGM group, even if not statistically significant, despite a better HbA1c level.
We hypothesize that this greater weight gain could be due to the possibility for the patient to control the postprandial hyperglycemic trend by administering additional boluses of insulin, which is facilitated by the use of the Bolus Wizard and/or continuous monitoring, thus allowing good glycemia control despite a larger food intake. Although this hypothesis needs to be confirmed because it was not the aim of our study, it suggests the importance of focusing on weight, food intake, and additional boluses during routine controls.
Conclusions
The results of our study showed the success of the use of CSII protocol even if compared with the well-known efficacy and flexibility of IVPs for the management of diabetes during delivery. 11,12 We know that our population is self-selected regarding the use of CSII or RT-CGM, and we acknowledge that this is a limit to the study in terms of demonstrating the efficacy of such new technologies themselves during pregnancy or delivery. Nevertheless, we believe that it could be also the strength of our results. In fact, the high motivation level of our patients allowed us to structure an education program in which the pregnant woman plays the main role and which becomes a “bridge” between the two teams, diabetological and obstetrical, raising the delivery room team's confidence in using the pump. Moreover, our results demonstrate the efficacy of CSII in easily achieving stable glycemic profiles during the postpartum period until the resumption of oral feeding, especially in women who underwent CS.
Finally, the support of RT-CGM, even if in a limited and self-selected group of women, allowed the diabetes specialist to better adapt the insulin treatment to the needs of the patient and the patient to accept and follow it more easily for a better outcome, particularly for changes in the nocturnal basal rate and in insulin dosage during delivery. Thus RT-CGM could be considered a useful tool in routine management of pregnancies complicated by diabetes in order to reach and maintain more restricted goals during every phase of gestation and delivery, targeting the normal glycemic profiles of healthy women in the same clinical situations. 13,36,37
Limits of the present study can be seen in the design itself (retrospective), in the self-selected population, and in the low number of vaginal deliveries, which did not allow us to verify the protocol during labor in a sufficient number of cases. Thus, we suggest that a multicenter prospective study should be performed in order to obtain further data and to verify our preliminary findings in different situations.
Footnotes
Author Disclosure Statement
No competing financial interests exist. R.F. researched data, contributed to the discussion, wrote the manuscript, and reviewed/edited manuscript. N.V. and E.A. researched data and contributed to the discussion. V.D.B. and M.A. contributed to the discussion. V.C., O.T., and S.A. researched data. M.B. researched data and submitted the manuscript. A.N. researched data, reviewed the manuscript, and contributed to discussion. R.F. is the guarantor for the content of the present article.