
Abstract
Objective:
This study compared glycemic variability in patients with type 2 diabetes given sitagliptin or voglibose.
Patients and Methods:
Seventeen type 2 diabetes patients were given sitagliptin 50 mg/day or voglibose 0.9 mg/day for 2 months and were hospitalized for a 4-day evaluation by continuous glucose monitoring (CGM). On discharge, they were crossed over to the other regimen for 2 months of treatment/4 days of evaluation. The CGM data were used to compare each parameter for glycemic variability.
Results:
The average glucose levels with sitagliptin and voglibose were significantly different at 138.6 and 152.6 mg/dL for 24 h (P=0.014) and 147.2 and 160.9 mg/dL for during daytime (P=0.050), respectively. The patients' glucose levels with sitagliptin and voglibose were significantly different at 125.3 and 139.7 mg/dL before breakfast (P=0.015) and 112.7 and 131.4 mg/dL before lunch (P=0.049), respectively. The time from before meal to postprandial peak glucose levels was significantly longer after dinner with voglibose than with sitagliptin (91.5 and 122.3 min, respectively; P=0.012). All of the slopes of glucose elevation were significantly lower with voglibose after each meal, with that after breakfast, lunch, and dinner being 1.16 and 0.86 mg/dL/min (P=0.031), 0.70 and 0.45 mg/dL/min (P=0.048), and 1.06 and 0.73 mg/dL/min (P=0.028), respectively.
Conclusions:
This CGM-based pilot study revealed that sitagliptin significantly lowered 24-h and daytime mean glucose levels and glucose levels before breakfast and lunch compared with voglibose, whereas the time from before dinner to peak postprandial glucose levels was significantly longer, and the slope of postprandial elevation of glucose level was significantly lower after each meal, with voglibose compared with sitagliptin.
Background
In white populations, patients with type 2 diabetes show characteristics of prominent obesity and high insulin resistance. However, Japanese patients with type 2 diabetes are relatively thin, and the main cause of diabetes is the impairment of insulin secretion rather than insulin resistance. At least early in the course of the disease, the initial response of insulin secretion is attenuated, and thus insulin secretion is delayed, resulting in a postprandial elevation of blood glucose before the hypersecretion of insulin occurs. 5 Because the basal secretion of insulin is normal in this stage, the fasting blood glucose level is not elevated, and in many cases a glucose tolerance test will show impaired glucose tolerance (IGT) conditions in which hyperglycemia develops only after the test.
The Funagata Study held in Japan demonstrated the 2-h glucose level from an oral glucose tolerance test (OGTT) was a predictive factor for cardiovascular events. 6 DECODE or DECODA revealed a high OGTT 2-h glucose level was an independent risk factor for cardiovascular diseases (CVDs). 7,8 The Diabetes Intervention Study showed that if the blood glucose level an hour after breakfast was 180 mg/dL or more, the mortality rate due to myocardial infarction significantly increased in type 2 diabetes patients. 9 Thus, the strong relationship between OGTT 2-h glucose level or postprandial hyperglycemia and CVDs was reported in these days, so the improvement of postprandial hyperglycemia may lead to the prevention of CVDs.
An α-glucosidase inhibitor (α-GI) lowers postprandial blood glucose levels by inhibiting disaccharidase in the small intestine and delaying monosaccharide absorption. The Study TO Prevent Non-Insulin-Dependent Diabetes Mellitus (STOP NIDDM) reported that new onset of diabetes or diabetes cardiovascular events for IGT patients was prevented by administering acarbose, which had already been shown to improve postprandial hyperglycemia. 10,11 The Voglibose Intervention Clinical Trial in IGT on the Reduction of Onset of type 2 Diabetes (VICTORY trial) revealed a noticeable decrease in the progression to diabetes when voglibose was administered to Japanese patients with IGT, leading to the approval of the drug for the prevention of diabetes in Japan. 12
Dipeptidyl peptidase-4 (DPP-4) inhibition enhances endogenous incretin action and also promotes glucose-dependent insulin secretion. Thus, DPP-4 inhibitor treatment can improve postprandial hyperglycemia. Sitagliptin is the first drug approved and launched as a DPP-4 inhibitor in Japan.
Of the clinical trials of sitagliptin conducted in a Japanese population to date, the Phase III trial compared sitagliptin 50 mg once a day or voglibose 0.2 mg three times daily for changes from baseline in glycosylated hemoglobin (HbA1c) and for decreases from baseline in postprandial 2-h and fasting glucose levels after 12 weeks of treatment in a total of 319 patients with no adequate glycemic control after 8 weeks or more of diet and exercise therapy who were allocated to either treatment. The change in HbA1c from baseline was −0.7% in those given sitagliptin versus −0.3% in those given voglibose, demonstrating a significant difference (P<0.001). Again, the change after 12 weeks of treatment in fasting glucose levels from baseline was −19.6 mg/dL in those given sitagliptin versus −8.9 mg/dL in those given voglibose, showing a significant difference (P<0.001), and the change in postprandial 2-h glucose levels from baseline was significantly greater in those given sitagliptin at −51.0 mg/dL than in those given voglibose at −32.2 mg/dL (P<0.001). 13 At the time of this study, however, there was no detailed investigation using a continuous glucose monitoring (CGM) device, which enables the measurement of a patient's blood glucose levels continuously. Therefore, we have conducted a crossover pilot study using CGM to reveal how these two oral hypoglycemic drugs with different mechanisms influenced the changes in blood glucose levels for Japanese patients with type 2 diabetes.
Patients and Methods
We included 17 subjects with type 2 diabetes from 20 to 80 years old, who had received nutrition/exercise therapy alone or nutrition/exercise therapy as well as drug therapy using oral hypoglycemic drugs (normal dosage of sulfonylurea, thiazolidinedione, or biguanide) over 2 months but did not have adequate blood glucose control (HbA1c range, 6.9% to <9.4%).
This study was approved by the ethics committee of the Jikei University School of Medicine, Tokyo, Japan.
Exclusion criteria of this study were as follows: type 1 diabetes; those who had severe ketosis, diabetic coma, or precoma within the past 6 months; those who had severe infection or severe trauma, preoperative or postoperative; those who had had laparotomy or ileus in the past; those who had chronic bowel disease with digestive or an absorption disorder; those who had Roemheld's syndrome, severe hernia, colon stenosis, or ulcers; those who were pregnant, had a possibility of being pregnant, or were in the lactation period; those who had renal dysfunction (creatinine clearance, <50 mL/min; if male, serum creatinine ≥1.5 mg/dL; if female, serum creatinine ≥1.3 mg/dL); those who had severe liver damage; those receiving insulin therapy; those who were taking glinide or another DPP-4 inhibitor; those who were allergic to sitagliptin or voglibose; and those who were judged inappropriate for this study by attending physicians because of medical grounds.
After written informed consent was obtained from the patients, they were randomly assigned to one of two groups: in Group A, patients received 50 mg of oral sitagliptin (alone or administered with sulfonylurea, thiazolidinedione, or biguanide) once daily after breakfast; in Group B, the patients took 0.3 mg of oral voglibose three times daily before each meal.
If they used oral hypoglycemic drugs before this study, they continued to take these drugs without changing the dose and added the other hypoglycemic drug until the end of this study. After 2 months of drug administration, they were hospitalized for 4 days and underwent CGM. When they were discharged from the hospital, Group A was switched to administration of 0.3 mg of oral voglibose three times daily before each meal, and Group B was given 50 mg of oral sitagliptin once daily. They continued to have treatments for 2 months and were then admitted to the hospital again for 4 days of CGM (Fig. 1).
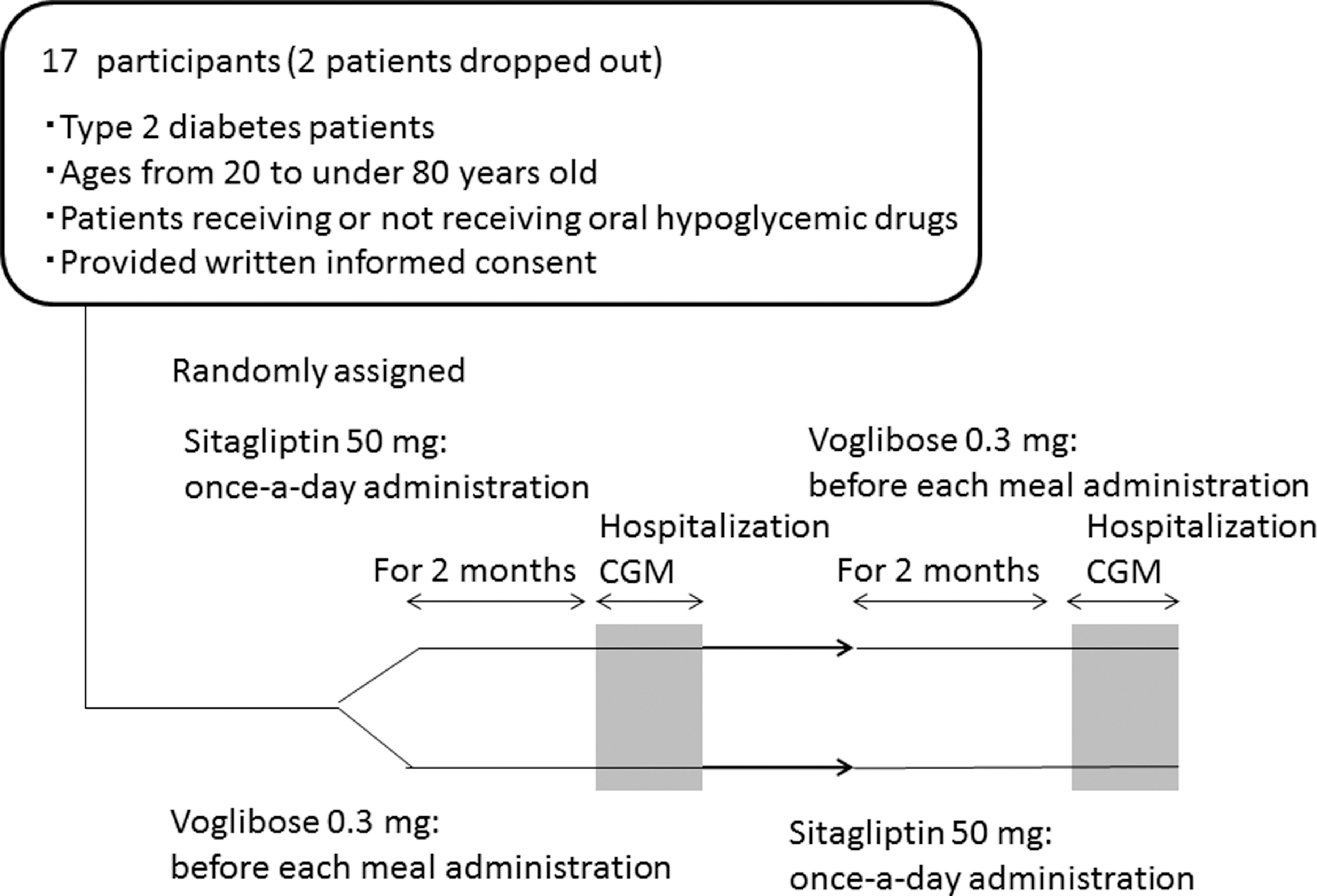
Study design. CGM, continuous glucose monitoring.
Ideal body weight was calculated for the subjects in both hospitalization periods. They had any one of three test meals: (1) 1,440 kcal/day, (2) 1,600 kcal/day, or (3) 1,840 kcal/day, on Day 2 and Day 3 of the admission. Their meals were selected according to ideal body weight (22×height squared [m2]) multiplied by 30, where, for any patient whose meal calories as calculated by this equation happened to fall between these calorie categories, the one closest to the calculated amount was chosen. The energy of each test meal was equally allocated to breakfast, lunch, and dinner. The energy proportion of the three major nutrients was as follows: carbohydrate, 61.0%; protein, 17.0%; and fat, 21.5%.
During the study period, additional administration of other diabetes drugs was not allowed. The patients were required not to perform excessive exercise and to maintain almost the same level of physical activity for the 4 days.
CGMS® System Gold™ (Medtronic, Northridge, CA) was applied to the abdomen during the 4 days of admission. A 5–10-min delay occurs if the measurement of the blood glucose level was compared with the interstitial fluid level measured by CGMS System GOLD. Furthermore, a low accuracy in the hypoglycemia range was also indicated. 14 However, there were no subjects who developed hypoglycemia in our study. Because the measurements were corrected with self-monitored blood glucose values more than four times a day, we considered the CGM results to be approximately equal to the blood glucose levels seen in venous fluid. 15
All 17 patients were put on CGM on Day 1 of their hospital stay and taken off CGM on the morning of Day 4. As a rule, CGM data obtained from these patients on Day 2 were used for current analysis, with the exception of one patient who had CGM sensor errors on both Days 2 and 3 and was excluded from analysis, two patients who had CGM sensor errors while on voglibose on Day 2 where CGM data obtained on Day 3 were used for analysis, and one patient who had CGM sensor errors on Day 2 while on sitagliptin where CGM data obtained on Day 3 were used for analysis. We had the CGM systems calibrated in all patients based on a total of four blood glucose measurements made before the three meals and before bedtime every day.
We compared the results obtained using the t test. The results included the following: the average glucose level under administration of both drugs on Day 2 of admission (if the sensor showed error, on the third day) for 24 h, during nighttime (0:00 p.m. to 8:00 a.m.), and during daytime (8:00 a.m. to 0:00 p.m.); the SD of the glucose level for 24 h, during nighttime (0:00 p.m. to 8:00 a.m.), and during daytime (8:00 a.m. to 0:00 p.m.); the mean amplitude of glycemic excursions 16 ; glucose level before each meal; peak glucose level after each meal; increased level of glucose range from before each meal to peak postprandial; the time from each before meal to peak postprandial glucose; the slope of glucose level elevation after each meal (divided the glucose level increase, which is from before each meal to peak postprandial by the time range from each before meal to peak postprandial glucose); area under the curve (AUC) where glucose level exceeded 140 mg/dL and 180 mg/dL; and AUC was from before each meal to 3 h postprandial.
We have used SPSS version 19 software (SPSS Inc., Chicago, IL) for statistical analysis.
Results
Among the 17 subjects, two patients dropped out: one because of drug-induced liver injury and one because of insufficient CGM data. The final analysis was performed on 15 patients (12 men and three women). The patients' background characteristics were as follows (given as mean±SD value): ages were 57±13.2 years old, duration of disease was 9.1±8.7 years, HbA1c level was 7.6±1.4%, and body mass index was 27.3±4.4 kg/m2 (Table 1). The concomitant drugs at start of the study were as follows: three patients took sulfonylurea (20%), and six patients took biguanide (40%) (Table 1).
Data are shown as frequency [n (%)] or average (±SD).
AHA, antihyperglycemic agent; BMI, body mass index; HbA1c, glycosylated hemoglobin; NGSP, formerly known as the National Glycohemoglobin Standardization Program.
After 2 months, the average glucose for 24 h (sitagliptin vs. voglibose, 138.6 vs. 152.6 mg/dL, P=0.014) and during daytime (8:00 a.m. to 0:00 p.m.) (147.2 vs. 160.9 mg/dL, P=0.050) showed significant lower values under the administration of sitagliptin. Values during the nighttime (0:00 p.m. to 8:00 a.m.) (121.5 vs. 136.0 mg/dL, P=0.052) also showed a similar trend (Table 2 and Fig. 2). The SDs of glucose levels for 24 h, during the nighttime, during the daytime, and for the mean amplitude of glycemic excursions did not show significant differences under administration of sitagliptin or voglibose (Table 2).

Changes in the average glucose level for 24 h in 15 patients with diabetes during administration of sitagliptin 50 mg or voglibose 0.9 mg.
Data are mean±SD values.
By t test with corresponding samples.
P<0.05 represents a significant difference.
AUC, area under the curve; MAGE, mean amplitude of glycemic excursions.
Glucose levels before breakfast (125.3 vs. 139.7 mg/dL, P=0.015) and before lunch (112.7 vs. 131.4 mg/dL, P=0.049) were significantly lower under the administration of sitagliptin, but no significant difference was shown before dinner (Table 2). Each peak postprandial glucose level and the glucose level increase from before each meal to the peak postprandial level did not show significant differences either (Table 2).
For the time from before a meal to peak postprandial glucose level, the after dinner values (91.5 vs. 122.3 min, P=0.012) were significantly longer during administration of voglibose compared with that of sitagliptin. The after lunch values (110.7 vs. 141.7 min, P=0.069) also revealed a similar trend (Table 2). All of the slopes of blood glucose elevation after every meal, including after breakfast (1.16 vs. 0.86 mg/dL/min, P=0.031), after lunch (0.70 vs. 0.45 mg/dL/min, P=0.048), and after dinner (1.06 vs. 0.73 mg/dL/min, P=0.028), were significantly lower under the administration of voglibose (Table 2). The AUC where glucose levels exceeded 140 mg/dL and 180 mg/dL and the AUC calculated from before each meal to 3 h postprandial did not show significant differences (Table 2).
Hypoglycemic effects of both drugs (sitagliptin for Group A and voglibose for Group B) were compared with regard to HbA1c level. For Group A patients administered sitagliptin first, the drug lowered HbA1c to 7.1±0.5% (mean±SD) over the 2-month period from the start of administration, whereas in Group B patients administered voglibose first, HbA1c decreased to 7.4±0.6% (mean±SD) over the 2-month study period. Although the baseline values were not identical at the start of the second part of the study, we confirmed that the hypoglycemic effects of both drugs were equivalent when we changed the drug administration regimen: sitagliptin first and voglibose next versus voglibose first and sitagliptin next.
Of the 15 patients available for analysis, 13 were included for follow-up on changes in all parameters examined from baseline, and two were lost to follow-up because of change of hospital after completion of the study. Among the 13 patients available for follow-up, their mean HbA1c value was 7.2±0.8% and 7.3±1.0% at 2 and 4 months after completion of the study, respectively. At hospital discharge, sitagliptin or voglibose was prescribed based on each patient's preference. As a result, of the 13 patients available for follow-up, nine opted for sitagliptin (Group S), three chose voglibose (Group V), and one chose neither. The mean HbA1c value 2 months after completion of the study was similar at 7.3±0.9% and 7.0±0.4% in Groups S and V, respectively, with no significant difference found between the groups (P=0.30). Again, the mean HbA1c value 4 months after completion of the study was similar at 7.4±1.1% and 7.1±0.4% in Groups S and V, respectively, with no significant difference found between the groups (P=0.25).
Discussion
We compared and investigated the changes in glucose levels under administration of sitagliptin (DPP-4 inhibitor) 50 mg/day and voglibose (α-GI) 0.9 mg/day by using CGM. Sitagliptin significantly decreased the average glucose level for 24 h and during the daytime (8:00 a.m.–0:00 p.m.) and glucose levels before breakfast and before lunch, compared with voglibose. We considered sitagliptin to have decreased the overall blood glucose levels because it inhibited DPP-4 activities to enhance incretin action and to improve glucose-dependent insulin secretion. Previous data indicated sitagliptin prevented the secretion of glucagon during nighttime. 17 Our results were consistent with the previous studies because the blood glucose levels before breakfast under administration of sitagliptin were lower than those of under voglibose.
Regarding the changes in glucose level after each meal, each drug revealed a distinctively different effect (Fig. 2). The changes in glucose levels after lunch were similar with both drugs; however, the glucose curve after breakfast, in particular after dinner, rose significantly rapidly under the administration of sitagliptin, compared with the findings for voglibose (Figs. 3 and 4). These results suggested voglibose had more significant effects for preventing an increase in postprandial glucose levels than did sitagliptin. An α-GI such as voglibose inhibits disaccharidase in the small intestine and delays the absorption of monosaccharide. Although it does not have an effect on improving fasting hyperglycemia, it moderates the postprandial increase in blood glucose levels. In contrast, sitagliptin, a DPP-4 inhibitor, acts to facilitate insulin secretion depending on the changes in blood glucose. Thus, we considered sitagliptin has less of an effect for preventing an increase of blood glucose levels compared with voglibose.

Changes in glucose level after each meal to 3 h after the meal during administration of sitagliptin 50 mg or voglibose 0.9 mg.

Changes in glucose level increase after each meal to 3 h after the meal during administration of sitagliptin 50 mg or voglibose 0.9 mg.
Recently, it has been suggested that the sharp increases in blood glucose levels (glucose spikes) such as postprandial hyperglycemia, rather than continuous hyperglycemia, might be a trigger related to the onset and progress of CVDs. 18 –21 A prior study indicated the importance of blood glucose management for improving blood glucose level changes as well as lowering levels of HbA1c, fasting blood glucose, and postprandial blood glucose. 22 We believe, based on these views, that voglibose's effect of moderating postprandial elevation of blood glucose levels may improve blood glucose control for 24 h.
This study revealed that sitagliptin improved fasting blood glucose levels and average blood glucose levels more than did voglibose, but voglibose moderated the slope of the postprandial blood glucose level more than did sitagliptin. It may be worthwhile to switch these drugs during treatment while observing the characteristics of blood glucose changes in the patients; that is, if the primary goal is to improve fasting blood glucose levels or average blood glucose levels, sitagliptin should be used, and if the primary goal is to moderate the slope of the postprandial elevation of blood glucose levels, voglibose should be used.
Furthermore, glycemic control with fewer excursions of blood glucose levels would be expected by co-administration of sitagliptin and voglibose, when taking into account the changes in blood glucose levels induced by each drug. This may be an effective treatment for preventing the onset and progression of diabetes complications including CVDs. Voglibose was previously reported as showing gastric inhibitory polypeptide reaction inhibition and glucagon-like peptide-1 reaction enhancement when the usual dose was administered to healthy subjects. 17,23 The amount of postprandial glucagon-like peptide-1 secretion was increased with miglitol, another α-GI. 24 Therefore, when an α-GI and a DPP-4 inhibitor are concomitantly used, the concentration of active-type glucagon-like peptide-1 is synergistically increased, and its action is likely enhanced. A previous study has already reported that the postprandial glucagon-like peptide-1 reaction was lower in patients with type 2 diabetes compared with healthy subjects, 25 so we consider that the combination therapy of an α-GI and a DPP-4 inhibitor might be an appropriate treatment for type 2 diabetes. Generally, premeal and nocturnal hypoglycemia remains a clinical concern in combination therapy with two different oral hypoglycemic agents. However, given that sitagliptin and voglibose are both less likely to cause hyperglycemia due to their unique mechanisms of action, it was thought likely that the risk for hypoglycemia could be minimized and better glycemic control could be obtained with their combined use in the 17 patients in this study. This needs to be further explored in a large number of patients, and approaches need to be explored in which to maximize their efficacy as single agents or combination therapy.
We compared the effect of sitagliptin and voglibose by using CGM and investigated the effect of a DPP-4 inhibitor and an α-GI on blood glucose changes. Limitations of this study include the small number of patients who participated and the applicability of data obtained during hospitalization, which might be different from that of daily life. The HbA1c level given was an average taken from a 2-month period of measurement. Because of the dietary control imposed following hospitalization, the blood glucose levels during this period were slightly lower as a whole than the average blood glucose level expected from the baseline HbA1c. Although sitagliptin 50 mg was used in the study, sitagliptin 100 mg is more commonly used in clinical practice. Thus, we plan to conduct a study involving the use of sitagliptin 100 mg for similar data analysis in the future.
We shall further investigate the effects on blood glucose level changes with a DPP-4 inhibitor and other oral hypoglycemic drugs and also continue to search for an optimal usage of oral hypoglycemic drugs and an ideal combination therapy for patients with diabetes.
Footnotes
Acknowledgments
The authors give special thanks to the study participants as well as Ms. Kimie Shida for data management. This study is supported by the Japan Diabetes Foundation.
Author Disclosure Statement
No competing financial interests exist.