
Abstract
Background:
Recently, it has been found that diabetes patients have a higher incidence of colorectal cancer than the general population, but epidemiological studies examining a potential relationship between the two have produced inconsistent conclusions. Thus, we set out to perform a meta-analysis of cohort studies to evaluate the association between diabetes and colorectal cancer.
Materials and Methods:
Using “diabetes,” “colorectal cancer,” and associated key words, we performed a systematic review of published cohort studies in multiple databases, including MEDLINE, EMBASE, ISI Web of Knowledge databases, OVID, CNKI, CBMD ISC, WANFANG, and CQVIP. We then applied stringent inclusion and exclusion criteria to identify which studies to include in our analysis. STATA version 12.0 software (StataCorp., College Station, TX) was used to conduct statistical analysis, including consolidated statistics calculations, tests for heterogeneity, and publication bias evaluations.
Results:
We obtained a total of 532 potential articles. In accordance with our inclusion and exclusion criteria, we selected 29 articles for the meta-analysis. The analysis of extracted information indicated that diabetes is a risk factor for the development of colorectal cancer (relative risk 1.22, 95% confidence interval 1.19–1.26). Subgroup analyses by control populations, regions, gender, follow-up time, and colorectal cancer site also support this finding.
Conclusions:
The risk of individuals with diabetes to develop colorectal cancer is 1.22 times higher than that of individuals without diabetes. The positive association remains consistent for both men and women and for studies carried out in North America, Europe, and Asia, as well as for different follow-up times.
Introduction
The hyperinsulinemia hypothesis suggests that elevated levels of insulin and free insulin-like growth factor-1 promote proliferation of colon cells and lead to a survival benefit of transformed cells, ultimately resulting in CRC. 14 Hyperinsulinemia, insulin-like growth factor-1, and its related binding proteins play an important role in regulating CRC metabolism, proliferation, and apoptosis. 15 Insulin not only stimulates the growth of colon cancer cells, but also participates in mediating insulin cognate receptor and the insulin-like growth factor-1 receptor expression. 14 Some studies have shown that, compared with normal colon epithelial cells, insulin receptor density in colon cancer epithelial cells is significantly increased.
In addition, studies indicate an additional molecular mechanism linking DM and CRC. Glucagon-like peptide-1, a hormone secreted by intestinal endocrine L cells, contributes to the Wnt signaling pathway and, subsequently, expression of c-myc and cyclin D1 oncogenes. Because of insulin resistance, patients with type 2 DM have reduced glucagon-like peptide-1 secretion. This causes a compensatory activation of the Wnt signaling pathway and thus increases c-myc gene expression, promoting cell proliferation and CRC development. 16
Another potential link between DM and CRC is slow-transit constipation. Diabetic neuropathy may affect the intestines in such a way that DM patients are more prone to constipation (bowel movement less than once a day) and slow colon peristalsis. This extends the exposure of the intestines to cancer-promoting fecal content, such as bile acid, ammonium acetate, and fecal-associated bacteria. 15 However, there is a lack of definitive epidemiological evidence supporting a role for constipation in CRC development.
In addition to DM, large numbers of studies have shown that individuals suffering from chronic colorectal inflammation, including those with ulcerative colitis, Crohn's disease, and inflammation caused by chronic schistosomiasis, were susceptible to CRC. For example, individuals with ulcerative colitis have a 20 times greater incidence of CRC than the general population. Ulcerative colitis is associated with the development of the precancerous lesions of CRC. 17 In addition, evidence indicates that colorectal polyps, particularly those that result from adenomatous polyposis, serve as precancerous lesions for CRC. According to the analysis of data from the National Polyp Study, people who joined the colonoscopy testing program had a 75% decrease in the incidence of colon cancer compared with the general population of corresponding age, likely because of the removal of adenomatous polyps by the colonoscopy procedure. 18
Epidemiologists have investigated the association between DM and CRC using case-control and cohort studies; however, their findings have been inconsistent. For example, Hu et al., 19 Larsson et al., 20 and Seow et al. 21 all reported that DM is a risk factor for rectal cancer; Steenland et al., 22 Schoen et al., 23 and Bowers et al. 24 did not find this association. Given the differences in epidemiological study conclusions, we undertook a meta-analysis method to comprehensively evaluate cohort studies in the literature to gain a better understanding of the relationship between DM and CRC.
Materials and Methods
For this prospective evaluation we defined our study population as individuals with type 1 and type 2 DM without taking into consideration their gender, age, and race. We chose cohort studies with DM as the exposure factor and CRC as the research outcome. We used methodology in accordance with the Meta-analysis of Observational Studies in Epidemiology guidelines. 25
Search strategy
We used MEDLINE, EMBASE, ISI Web of Knowledge, OVID, and other English databases as well as CNKI and CBMD, the ISC, Wanfang Data, VIP, and other Chinese databases as the sources of literature. The start point for retrieval was when a database was built and ended on May 1, 2012. The Chinese literature search key words included “diabetes,” “colorectal cancer,” “colon cancer,” “colorectal cancer,” and “colorectal cancer, cohort studies.” English search key words included “diabetes mellitus,” “diabetes,” “colorectal cancer,” “colorectal neoplasm,” “colon cancer,” “colon neoplasm,” “rectal cancer,” “rectal neoplasm,” “cohort studies,” etc.
For MEDLINE, details are as follows: #1, “Diabetes” OR “Diabetes Mellitus” OR “DM” OR “insulin resistance” OR (“hyperinsulinism” OR “hyperinsulinemia”); #2, “Colorectal Neoplasms” OR “Colonic Neoplasms” OR “Rectal Neoplasms” OR “colorectal cancer” OR “colon cancer” OR “rectal cancer” OR “CRC”; #3, “Cohort Studies” OR “Epidemiologic Studies”; #4, #1 AND #2 AND #3.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) a cohort study; (2) exposure factors included DM; (3) study outcomes included the incidence of colorectal cancer, colon cancer, or rectal cancer; and (4) study results included relative risk (RR), hazard ratio (HR), or standardized incidence rate (SIR) of these indicators, and also the 95% confidence intervals (CIs), which can be calculated from the published data.
Exclusion criteria were as follows: (1) incomplete original data; (2) cross-sectional and case-control studies; (3) articles that did not specify the correction factors of the risk estimates in the study or variables, such as age, body mass index, physical activity, smoking, aspirin usage, fruits, vegetables, mammal meat intake, etc.; (4) articles that lacked a complete text; and (5) in the case of repeated reports in the literature, the most recent article was selected, excluding other literature.
Data extraction and quality assessment
We used the Newcastle-Ottawa Scale standards 26 to evaluate the quality of the studies retrieved though our literature search. Data extracted included the author, year published, the state, study time, the number of people studied (the number with DM), age, gender, DM information, the average visiting time, the adjusted RR (HR or SIR) and their 95% CIs, and control variables in studies. This process was carried out independently by two researchers (L.W. and J.T.), who also cross-checked each other's work with input from the corresponding author in cases of disagreement or uncertainty.
Statistical analysis
According to the type of control and the assessment of the relative risk indicators (RR, HR, or SIR), we divided the epidemiological studies into two groups: one group included studies with queuing within the population as a control in which RR or HR was used for the results of cohort studies, and the other group included studies with queuing outside the crowd, in which SIR was used for the findings of the cohort studies.
STATA version 12.0 (StataCorp., College Station, TX) was used to conduct the meta-analysis on the relationship between DM and CRC, using RR (SIR) and its 95% CIs for the merger of statistics, a statistical analysis model as the random-effects model (DerSimonian–Laird method), and a forest plot. Statistical heterogeneity was assessed using the Cochran Q test and I2 statistics; a Q-test P value of <0.10 or I2 a value of >50% was considered as a measure of statistical significance of the heterogeneity in the studies. We conducted subgroup analysis to examine potential sources of heterogeneity according to gender, region, follow-up time, the control type, and cancer subsite. For assessing publication bias, we used funnel plots to do the intuitive assessment. If no publication bias was included in the published study, the graphics would render an inverted funnel plot; if the funnel plot was asymmetric or incomplete, it indicates publication bias. In addition, we used Begg's adjusted rank correlation test and Egger's regression test for quantitative assessment of publication bias. If both tests yielded the same conclusion, then results are more likely reliable. Inconsistent results indicate publication bias, and in this case we used. Begg's test results as criteria.
Results
Literature screen
The DM and CRC literature search using Chinese and English databases retrieved 532 articles: 146 from the Chinese database and 386 from English databases. Based on our defined inclusion and exclusion criteria, our preliminary screen, which consisted of reading the title and abstract, excluded 412 articles (146 Chinese and 266 English ones). We then carefully evaluated the remaining 120 articles, which resulted in the exclusion of an additional 88 articles (including three studies that did not estimate the risk of DM and CRC). At the same time, we also eliminated three research queue articles that were duplicates. Eventually, 29 19 –24,27 –49 articles were included in our cohort study of DM and CRC. We then classified these articles by indicators of risk assessment: 24 articles used RR as a risk assessment indicator, whereas one article of these 24 and the other five articles used SIR to evaluate the research results (Fig. 1).
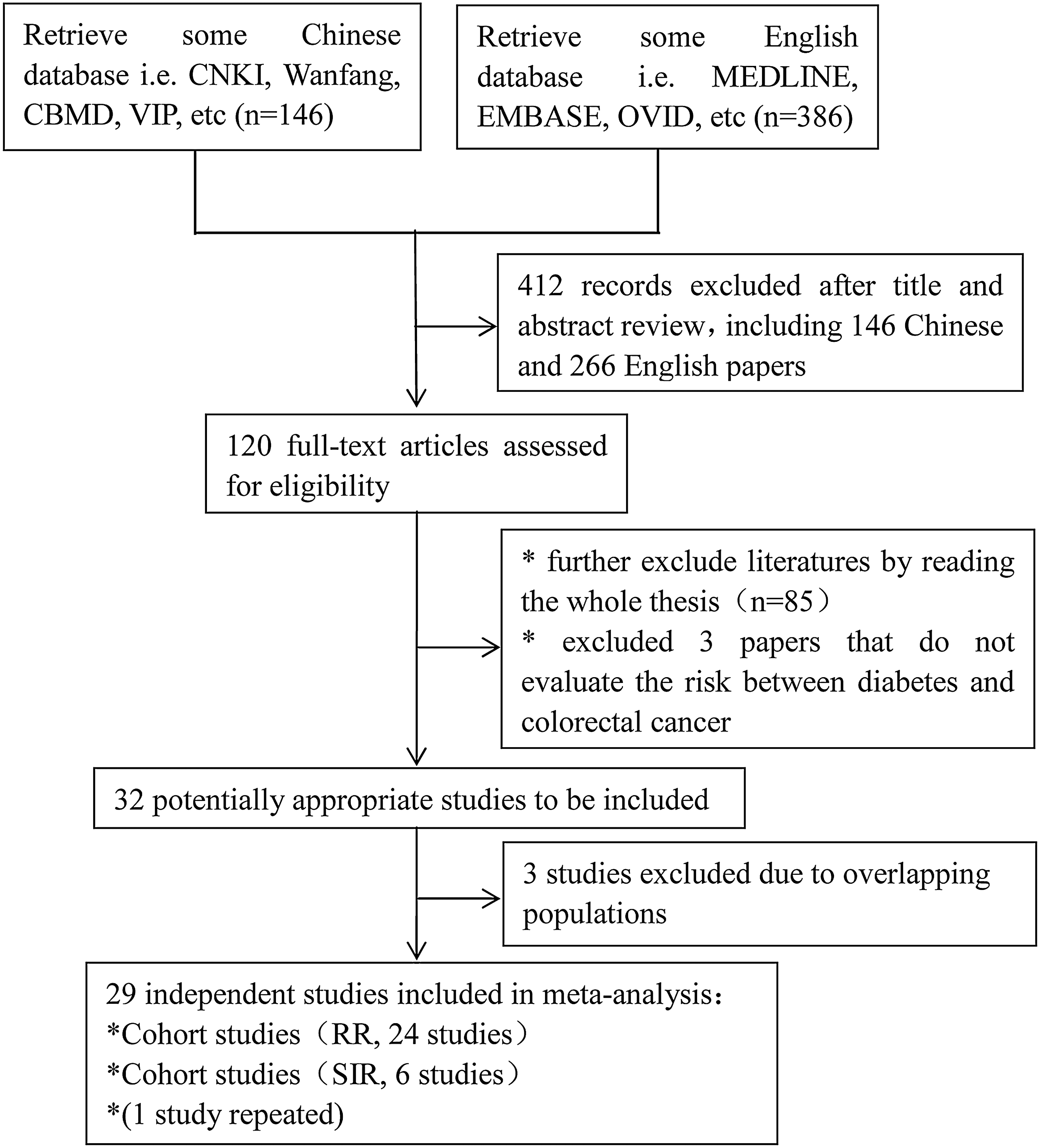
Flowchart of the article selection process. RR, relative risk; SIR, standard incidence rate.
Information on included literature
The vast majority of retrieved articles used for this analysis were published between 1982 and 2011. The merged objects of study totaled 8,246,514 people, with 786,739 patients listed as having DM. RR was primarily used as the indicator for risk assessment. However, although only a small number of articles used SIR as an indicator of risk assessment, the number of merger research objects in these articles was considerable, totaling 416,969 people. The study sites were mostly concentrated in North America, especially in the United States; China had no such cohort studies reported. DM information was mostly obtained from patients' self-reporting, but some articles used blood glucose levels as a criterion for DM. The CRC diagnosis was made in the vast majority of the articles through cancer registries or medical records. The longest average follow-up time was 19 years, whereas the shortest was 6 years.
To extract additional RR information from DM and CRC risk, we carried out a statistical analysis by gender and CRC site (proximal colon cancer, distal colon cancer, and rectal cancer), respectively. Of note is that published RRs represent corrected values. The correction factors or control variables in each article were slightly different and included factors such as age, body mass index, physical activity, smoking, aspirin use, and fruit, vegetables, and red meat consumption.
Comprehensive evaluation of the relationship between DM and CRC
We merged the 24 articles with RR as the risk assessment indicator and the six articles with SIR as the risk assessment indicator, to comprehensively evaluate the relationship between DM and the incidence of CRC. Using the Cochran Q test and I2 statistics, we identified heterogeneity within the studies (Q=48.56, P=0.013, I2 =40.3%). Therefore, we used the random effect model to estimate the CIs of the merger RR. The analysis showed that DM is a risk factor for CRC, with a merger RR equal to 1.22 and a 95% CI of 1.19–1.26. Results are shown in Figure 2.
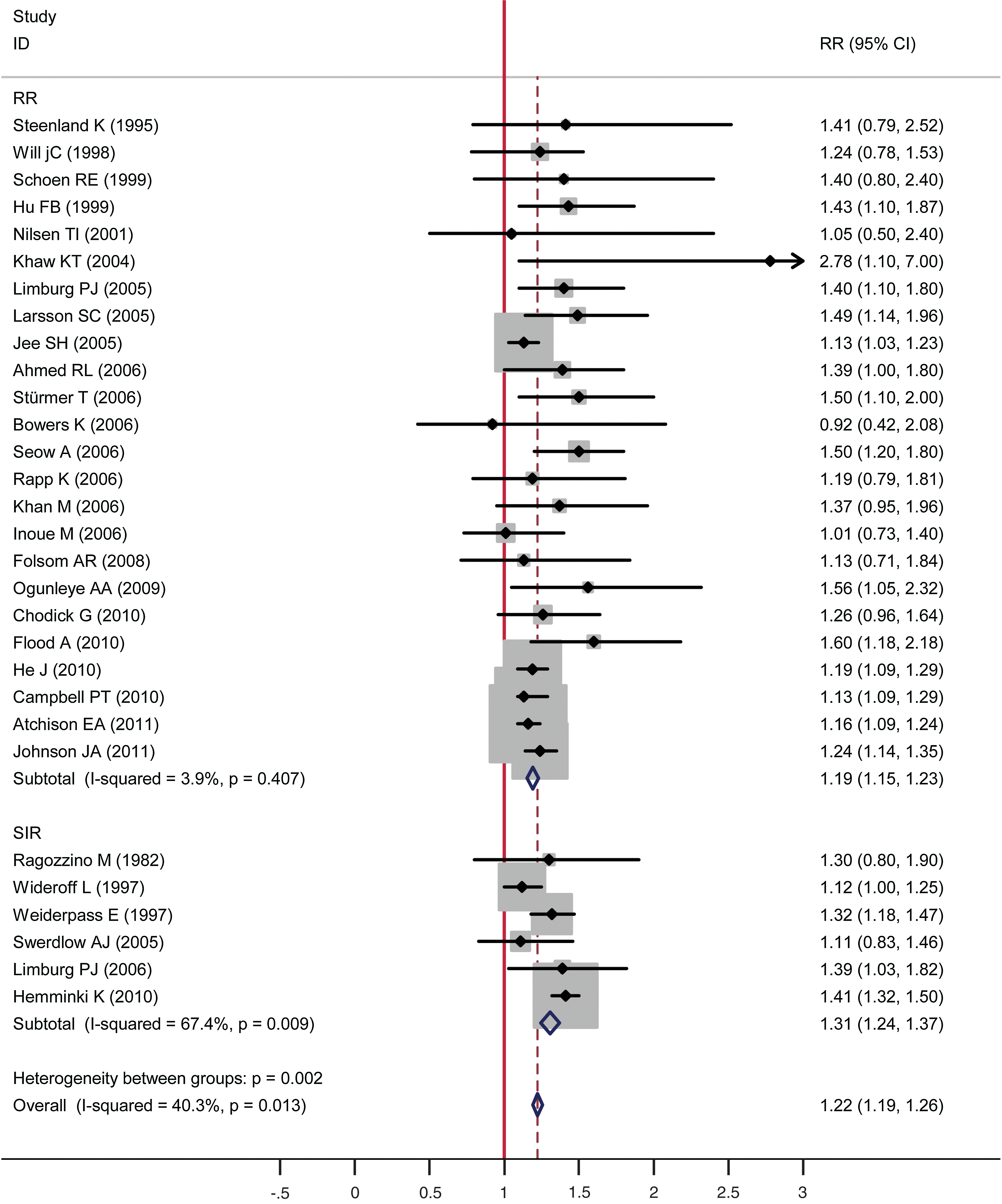
Forest plots of colorectal cancer incidence/standard incidence rate (SIR) associated with diabetes.
19
–24,27
–49
Squares represent the study-specific relative risk (RR). Diamonds represent the summary RRs (SRRs). Horizontal lines represent the 95% confidence intervals (CIs). (Color graphics available online at
To find the source of heterogeneity, we tested the stability of the combined RR value and conducted hierarchical analysis based on control groups, regions, follow-up time, gender, and CRC site. Control group stratified analysis showed that heterogeneity came mainly from the queue outside the crowd, so we conducted a controlled study. The literature queue within the population as a control did not have heterogeneity (Q=23.94, P=0.407, I2 =3.90%), the combined RR (95% CI) of the queue within the control population studies was 1.19 (1.15–1.23), and the combined RR value of the queue outside the control groups of was 1.31 (1.24–1.37). From different studies in different regions, the heterogeneity mainly existed in European studies. Nevertheless, research in North America, Europe, and Asia all suggested that DM is a risk factor for CRC, with RR (95% CI) equaling 1.20 (1.15–1.24), 1.31 (1.26–1.37), and 1.16 (1.07–1.25), respectively. We then stratified the data according to the follow-up time: 11 articles had a follow-up time of <10 years, whereas 19 articles had a follow-up time of ≥10 years. The heterogeneity between studies mainly came from the latter. In the two different follow-up studies, the pooled RR values were more stable. The result of CRC risk analysis on DM patients with different genders suggests a greater CRC risk for men with DM (RR=1.30) than women (RR=1.15). Heterogeneity mainly originated from the research that looked at males. For predilection sites of CRC, studies indicated a higher possibility of developing DM with colon cancer (RR=1.25, 95% CI 1.22–1.29) compared with rectal cancer (RR=1.15, 95% CI 1.11–1.20). Details are shown in Table 1.
CI, confidence interval; RR, relative risk.
We next evaluated the possibility of a publication bias in the articles included in our analysis. The funnel plot (Fig. 3) illustrates an even distribution of the points on both sides of the map, suggesting a lack of publication bias. Similarity, Begg's test and Egger's test results suggest that the articles included did not have a publication bias, with the former having Z value of 0.41, P=0.682 and the latter having t=1.39, P=0.175 as shown in Figure 4.

Funnel plot analysis of the included articles' publication bias about diabetes mellitus and colorectal cancer. RR, relative risk.

Begg's test and Egger's test of the included articles' publication bias regarding the incidence of diabetes mellitus and colorectal cancer.
Discussion
To comprehensively evaluate the relationship between DM and the incidence of CRC, we conducted a meta-analysis on a large number of studies that took place over a broad span of time and locations. The time span shows the history and reality of literature. Indeed, the studies spanned North America and dozens of countries in Europe and Asia. Results appear reliable and have universal applicability. To obtain comprehensive information, we used both Chinese and English databases to retrieve 512 articles. To ensure the authenticity of findings, we developed rigorous inclusion and exclusion criteria and eventually identified 29 studies to include in our analysis. Nearly 10 million research objects are merged. These studies were all cohort studies, and our analysis strongly indicates a relationship between DM and CRC.
Relationship between DM and the incidence of CRC
Results of the comprehensive evaluation of the 29 articles suggest that DM is a risk factor for CRC. Although we calculated a merged RR value of 1.22, we consider it a negligible result because it was obtained from a huge sample, and this result still exists in different genders, regions (North America, Europe, and Asia), follow-up times, and relationships between DM and CRC.
Epidemiological studies suggest that risk factors for the incidence of CRC include high-fat and high-protein diet and poor lifestyle, whereas risk factors of DM are almost the same. Thus, DM as a risk factor for CRC appears reasonable both in theory and in practice. 50,51
Accuracy and reliability of findings
We think that the results of the present article are accurate and reliable for multiple reasons. First, we based our analysis on a large number of articles and samples and used strict inclusion criteria adopted. Moreover, combined effect volume indicators are unified (RR, HR, and SIR). In particular, the analysis relied upon classical epidemiological prospective cohort studies. Results obtained were relatively stable, with a strong ability in analyzing the causal relationship between DM and CRC, and a smaller selection bias. Second, we conducted a stratification sensitivity analysis based on population, area, follow-up time, gender, and CRC site. The results confirmed that patients with DM are more prone to develop CRC. Third, as a meta-analysis, publishing bias can have a large impact; however, using a funnel plot, Begg's test, and Egger's test, we demonstrated that the selected articles lacked discernible bias. Fourth, the STATA statistical analysis software we used is powerful and has a wide range of applications. From the current reports, most meta-analyses use STATA's “meta. ado” module, as this software of meta-analysis not only can complete two categorical variables, continuous variables, meta-regression analysis, and the cumulative meta-analysis, but can also verify Begg's test and Egger's test for publication bias. 52
Limitations
Although our meta-analysis has man strengths, there are some limitations. First, the information from published articles is sometimes inadequate, limiting the conclusions that can be drawn. However, from the results of stratified analysis, we can conclude that factors such as gender, study location, and follow-up time may play a role in the heterogeneity included described in the literature; for example, in articles from the Khaw and Wareham groups, 29 its representation of outstanding ideals may be insufficient. Second, in most studies, the prevalence of DM was based on self-reports, which could lead to several DM patients being wrongly assigned to the nonexposed group. Although it has been shown that, compared with medical records, self-reporting for chronic disease is fairly reliable, 53 misclassification could lead to an underestimate of the strength of the link between DM and CRC. Third, we did not perform a separate analysis for type 1 DM and type 2 DM, which may have an effect on the results as some studies have shown that type 1 DM will not cause the occurrence of CRC. 54 At the same time, it should be noted that the incorporated patients were more than 30 years old, and thus likely all suffering from type 2 DM. Fourth, we did not take into account DM drug use, and some studies have suggested that the common antidiabetes drug metformin protects against the occurrence and development of certain types of cancer, 55,56 whereas DM patients using insulin or insulin analogs will have increased risk of certain cancers. Lastly, diet, obesity, smoking, physical activity, and other confounding factors may also affect the real link between DM and CRC, as confounding factors cannot be completely ruled out by meta-analysis.
The prevalence of DM will likely dramatically increase; the global population of 20–79 year olds with DM in 2007 was about 248 million with a prevalence of 5.9%, but by 2025, projections indicate a global DM population of 384 million individuals with a rise in prevalence to 7.1%. 1 In China, a 2007–2008 cross-sectional study showed that the prevalences of DM and prediabetes were 9.7% and 15.5%, respectively. 57 This phenomenon also indicates that colon cancer occurrence will also likely increase. Because of these trends, the association between DM and CRC will attract more and more attention, and as a way to examine the causal relationship between the two, the prospective cohort study and meta-analysis are important methods. However, we believe that these types of studies represent only one aspect, and to further explore the link between DM and CRC will require mechanistic studies. 58 –61
Footnotes
Acknowledgments
We are thankful to Prof. Qing Ye and Moira Hitchens for their critical review of the first draft.
Author Disclosure Statement
No competing financial interests exist.