
Abstract
Background:
After approval of sitagliptin and >750 mg of metformin in Japan, a triple oral antidiabetes drug (OAD) regimen including sulfonylurea, metformin, and sitagliptin was sometimes described. However, in the real world of clinical practice, the daily dose of sulfonylurea tended to be decreased according to the warning from the Japan Diabetes Society for avoiding hypoglycemia, instead of increasing the dose of metformin for maintaining hemoglobin A1c (HbA1c) levels with this regimen. This study examined the impact of either a small dose of glimepiride or a high dose of metformin on HbA1c in triple OAD therapy with sitagliptin in a 3-month, single-center, open-label, randomized controlled study.
Subjects and Methods:
Fifty-six type 2 diabetes mellitus patients who had been treated with 50 mg of sitagliptin, ≥1,000 mg of metformin, and ≤1 mg of glimepiride with an HbA1c level of <7.4% during at least 3 months were enrolled in the study. The patients were randomly assigned to two treatment groups who either received a 50% reduced dose of metformin (n=27) or discontinued glimepiride (n=29), while sitagliptin administration continued in both groups. Twenty-six patients from the reduced metformin group and 27 patients from the discontinued glimepiride group completed the study.
Results:
Significantly greater changes were observed in HbA1c and glycated albumin levels in patients who discontinued glimepiride than in patients with a 50% reduced metformin dose, during the 2–3-month period than in the 1–3-month period.
Conclusions:
Glimepiride is important for good glycemic control in triple OAD therapy with sitaglitpin and metformin. This regimen may be useful for those patients who do not achieve satisfactory glycemic control with dual combination therapy.
Introduction
Sitagliptin treatment has been produced meaningful reductions in HbA1c as well as in fasting and postprandial glucose concentrations. In these clinical studies, sitagliptin has been used as monotherapy, 5 in add-on therapy to metformin, 6 or in initial combination therapy with metformin 7 or sulfonylurea. 8 In the ASSET-K study of Japanese T2DM patients, 31% of the study population was treated with triple OAD regimens including sitagliptin. 9 In Korean T2DM patients, add-on treatment of sitagliptin with metformin and sulfonylurea showed an improvement of 1.27% in HbA1c levels after the 14-week study period. 10 As a result of these studies, triple OAD therapy including sitagliptin has been used relatively frequently in clinical practice.
On the other hand, severe hypoglycemia occurred frequently in the patients with sulfonylurea and dipeptidyl peptidase-4 inhibitor in Japan, and the JDS warned that glimepiride should be decreased to ≤2 mg daily in combination with sitagliptin to avoid severe hypoglycemia in 2011. Thus, in real clinical practice, the daily dose of sulfonylurea tended to be decreased, instead of increasing the dose of metformin in triple OAD therapy, to avoid hypoglycemia while maintaining HbA1c levels. Actually, we had experienced that the average daily dose of glimepiride in the subjects enrolled in this study was decreasing from 2.1 mg to 0.96 mg, whereas metformin was increasing from 585 mg to 1,147 mg from the time of enrolling in the study with addition of sitagliptin to ongoing glimepiride and metformin, while their HbA1c levels were improving from 7.4% to 6.5% during this period.
We have previously reported on three patients who showed great improvement in their HbA1c levels with triple OAD therapy using sitagliptin, metformin, and sulfonylurea. 11 The HbA1c levels of two patients improved after an increased dose of metformin of ≥1,000 mg/day, even with a decreased dose of sulfonylurea. In addition, the third patient achieved good glycemic control after the addition of a small dose of sulfonylurea to ongoing sitagliptin therapy with 1,500 mg of metformin/day. Thus, we propose that metformin at ≥1,000 mg/day and a small dose of sulfonylurea may be necessary to add to sitagliptin therapy for good glycemic control in triple OAD therapy.
From these experiences, we have questions on whether sulfonylurea treatment can be stopped or whether the dose of metformin can be decreased again after achieving satisfactory glycemic control with triple OAD therapy. To solve these clinical questions, we conducted a single-center, randomized prospective study.
Patients and Methods
Setting and participants
We conducted a 3-month, single-center, open-labeled randomized controlled study to evaluate the impact of discontinuation of sulfonylurea or use of a lesser dose of metformin on HbA1c levels during triple OAD therapy. Prospective adult T2DM patients for enrollment in this study were screened at the Health Education Center Science Clinic (Yokohama, Japan). Their type of diabetes was determined on the basis of the criteria for the diagnosis of diabetes of the JDS, 12 which are almost identical to those of the World Health Organization. 13 In brief, patients who were permanently insulinopenic and ketosis-prone (idiopathic type 1 diabetes mellitus) or those who were positive for autoimmune destruction markers, such as glutamic acid decarboxylase (immune-mediated type 1 diabetes mellitus), were diagnosed with type 1 diabetes mellitus and excluded.
Patients were eligible for the study if they had been treated daily with 50 mg of sitagliptin, ≥1,000 mg of metformin, and ≤1 mg of glimepiride and had HbA1c levels of <7.4% during at least 3 months with <5% variation. In total, 59 patients were assessed as eligible and were enrolled in this study. The study flow diagram is shown in Figure 1. Glimepiride is a third-generation sulfonylurea drug and is most commonly used drug of this class in Japan. Therefore, glimepiride was chosen for use in this study.
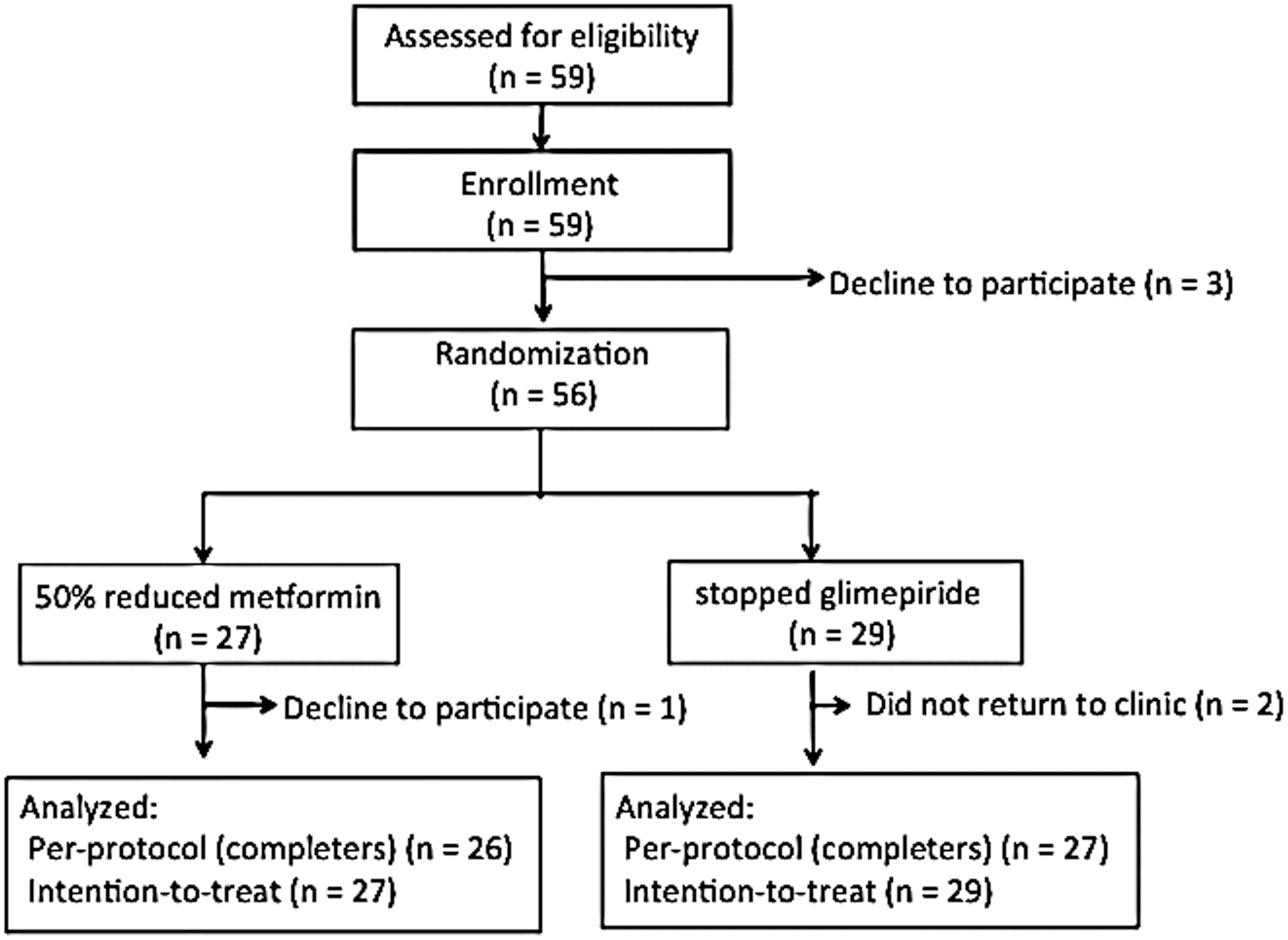
Diagram for study flow. In total, 56 patients with type 2 diabetes mellitus were randomly assigned to one of two treatment groups either with a 50% reduced dose of metformin (n=27) or who discontinued glimepiride (n=29). Of these groups, 26 and 27 patients, respectively, completed the 3-month study period.
The study was approved by the Ethics Committee of the Health Education Center Science Clinic, which includes lawyers and ethics experts as external members. All patients provided informed written consent prior to participating in the study, in accordance with the “Guidelines for Epidemiological Study” of the Japanese Ministry of Health, Labour and Welfare.
Randomization and intervention
In total, 59 patients with T2DM 54–90 years old, were enrolled in this study from July to November 2011. Three patients declined participation after enrolling, and the remaining 56 patients were assigned by random number table selection into two groups. One group of subjects received a 50% reduced daily dose of metformin (n=27), and the other group discontinued glimepiride (n=29). All other OADs were not changed, and no other drugs were newly prescribed during the study. Patients were encouraged to visit the clinic every month during the study period. Blood samples were taken from all subjects in a fasting state at baseline, after a 3-month period, and in either the fasting or postprandial state at the 1- and 2-month time points. Patients were discontinued from the study if they had an HbA1c level of >8.9%, a fasting plasma glucose (FPG) level of >250 mg/dL, or a postprandial plasma glucose level of >350 mg/dL that was measured twice sequentially (Fig. 1).
After the end of the study period, treatment that was stopped during the study was resumed in all patients excepting those who were maintaining satisfactory glycemic control.
Assessments and end points
The primary end point to determine whether changes in drug treatment had a significant effect was the change in HbA1c levels (%) from baseline time point (randomization) to the 3-month time point. HbA1c levels were measured by high-performance liquid chromatography at baseline and at the 1-, 2-, and 3-month time points. HbA1c levels are expressed as NGSP values and were calculated using the following formula: HbA1cJDS (in %)+0.4%, where HbA1cNGSP (in %)=1.019×HbA1cJDS (in %)+0.30, according to the guidelines of the JDS. 14 Also, we calculated the percentage of the patients who could achieve an HbA1c level of <7.0% between the two groups.
An additional end point was the change in glycated albumin (GA) levels (%) from the baseline time point to the 3-month time point. GA levels were analyzed to establish if they supported the trend of changes in HbA1c levels in case the length of the study period was not sufficient to observe a significant change in HbA1c levels. GA levels were measured by an enzymatic method.
Measurement of covariates
Demographic variables, including age, sex, height, body weight, and duration of diabetes, were collected for each patient before he or she was enrolled in the study. Weight and height were measured by standard techniques and equipment, and these data were used to calculate the body mass index (BMI). Plasma glucose level was measured by the glucose oxidase method. Plasma fasting C-peptide immunoreactivity (CPR) and the immune-reactive insulin (IRI) level were measured by the chemiluminescent immunoassay method at the baseline and 3-month time points. The CPR index (CPI) was calculated as follows: CPI=CPR (in ng/mL)/FPG (in mg/dL)×100. 15,16 Homeostasis model assessment-β-cell function (HOMA-β) and homeostasis model assessment-insulin resistance (HOMA-IR) were calculated as {fasting IRI (in mU/mL)×360}/{FPG (in mg/dL)−63} (in %) and FPG (in mg/dL)×fasting IRI (in mU/mL)/405 to assess β-cell function and insulin resistance, respectively. 17,18
Statistical analysis
Unless otherwise stated, all data were analyzed in the intention-to-treat population, comprising all of the randomized patients including those who did not complete the study because of a discontinued criterion or follow-up failure.
Mean intergroup HbA1c values were subjected to repeated-measures analysis of variance and the Bonferroni's multiple comparison test. At baseline, continuous variables (HbA1c, BMI, age, duration of T2DM, FPG, CPR, IRI, CPI, HOMA-β, and HOMA-IR) were compared between the two groups using the Mann–Whitney U test because sample size was small, whereas the χ2 test was used to compare categorical variables such as the proportion of men to women. The intergroup comparison of covariates, such as BMI, FPG, CPR, IRI, CPI, HOMA-β, and HOMA-IR, were subjected to Wilcoxon's sign-ranked test. Variables are presented as median (interquartile range) values.
All statistical analyses were performed using SPSS version 13.0J for Windows software (SPSS Inc, Chicago, IL). P<0.05 was considered to be significant.
Results
In total, 56 patients were randomly assigned either to a group who received a 50% reduced dose of metformin (27 patients) or to a group who stopped glimepiride (29 patients). Fifty-three patients completed the 3-month study. One patient in the reduced metformin group declined to participate, and data collection was discontinued. Two patients in the glimepiride-withdrawal group were discontinued from the study because they did not return to the clinic (Fig. 1). Baseline characteristics were not significantly different between the two groups (Table 1).
Data are median (interquartile range) values unless indicated otherwise.
CPR, C-peptide immunoreactivity; HbA1c, hemoglobin A1c; HOMA-β, homeostasis model assessment-β-cell function; HOMA-IR, homeostasis model assessment-insulin resistance; IRI, immunoreactive insulin.
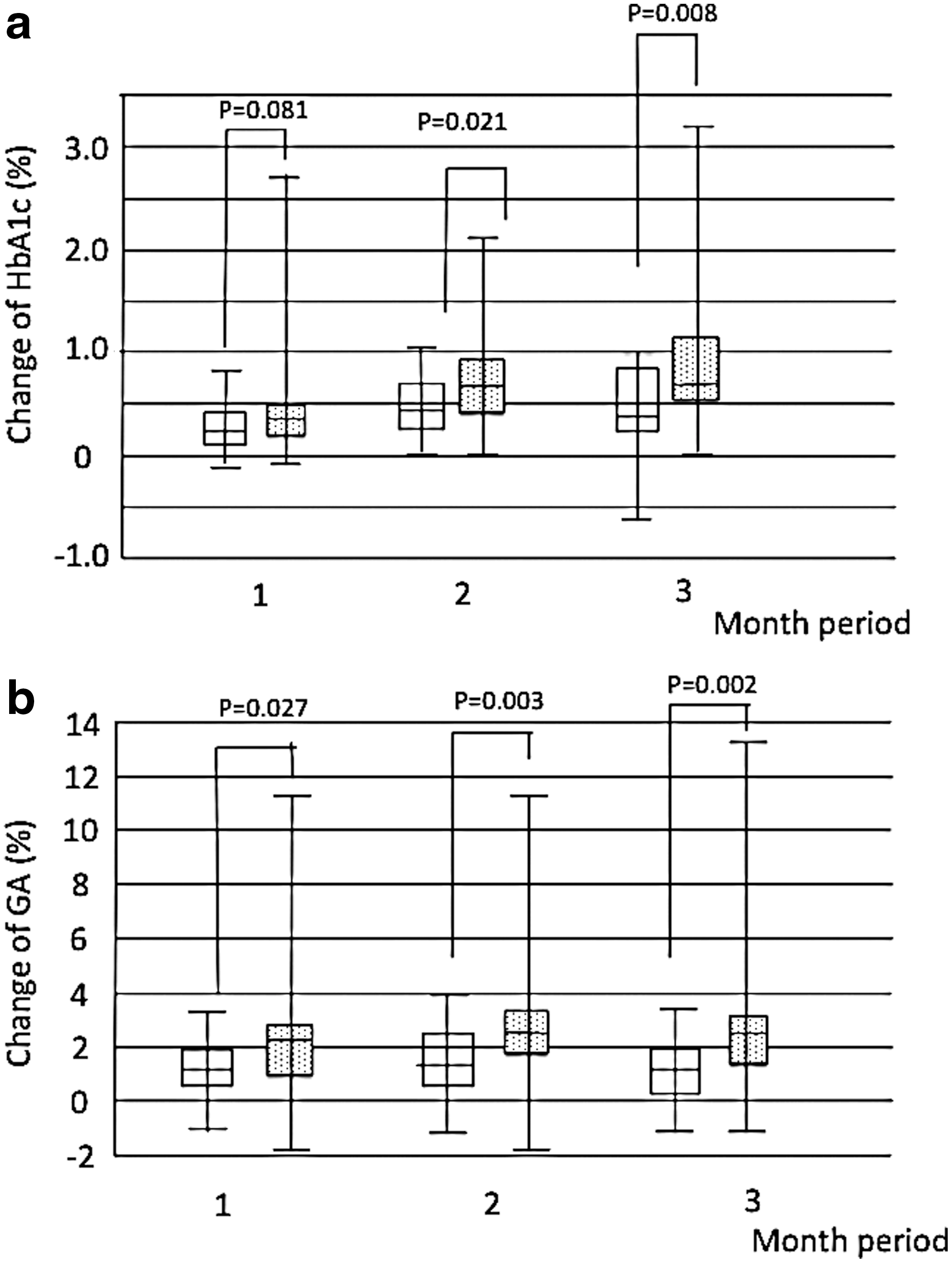
The HbA1c levels (given as median [interquartile range]) at baseline and at the 3-month time point were not significantly different: 6.5% (6.3–6.9%) and 6.4% (6.2–6.7%) at baseline and 7.0% (6.7–7.4%) and 7.3% (6.7–7.6%) at the 3-month time point in the 50% reduced metformin dose group and the discontinued glimepiride group, respectively. Similarly, the GA levels at baseline and at the 3-month time point were not significantly different: 16.8% (15.1–19.0%) and 16.2% (15.4–18.1%) at baseline and 18.3% (16.8–20.8%) and 18.5% (17.5–20.6%) at the 3-month time point in the 50% reduced metformin dose group and the discontinued glimepiride group, respectively (Tables 1 and 2). The change of HbA1c levels from baseline in the discontinued glimepiride group was more than in the 50% reduced metformin dose group at the 2-month (P=0.021) and 3-month (P=0.008) time points (Fig. 2a). GA levels showed changes similar to those in HbA1c levels from the 1-month (P=0.027) and 2-month (P=0.003) time points to the 3-month time point (P=0.002) (Fig. 2b). The numbers of patients who achieved an HbA1c level of <7.0% at the baseline and 3-month time points were 22 (81.5%) and 12 (44.4%) in the metformin reduction group and 26 (89.7%) and nine (31.0%) in the glimepiride-discontinued group (Tables 1 and 2).
Changes of
Data are median (interquartile range) values unless indicated otherwise.
P<0.05, b P<0.01, c P<0.001 versus 50% reduced metformin dose group.
CPR, C-peptide immunoreactivity; HbA1c, hemoglobin A1c; HOMA-β, homeostasis model assessment-β-cell function; HOMA-IR, homeostasis model assessment-insulin resistance; IRI, immunoreactive insulin.
The values for BMI, CPR, IRI, FPG, and HOMA-IR were not significantly different between the two groups at the 3-month time point, whereas the values for CPI and HOMA-β in the glimepiride-discontinued group were lower than those in the 50% reduced metformin dose group (Table 2). The values for CPR, IRI, CPI, and HOMA-β in the glimepiride-discontinued group decreased more than for the 50% reduced metformin dose group. The change of BMI was less in the glimepiride-discontinued group than for the 50% reduced metformin dose group, and there was no difference in the change of FPG and HOMA-IR between the two groups (Table 2).
Discussion
This study determined that after 3 months in either treatment group, the HbA1c and GA levels were not significantly different. In addition, the increases in both HbA1c and GA levels from baseline to the 3-month time point in the glimepiride-discontinued group were much more than those in the 50% reduced metformin dose group. This suggests that inclusion of glimepiride has a greater effect on HbA1c levels than a higher dose of metformin in triple OAD therapy that includes sitagliptin, metformin, and glimepiride, although both glimepiride and a higher dose of metformin may be important factors for good glycemic control in this triple OAD therapy.
Metformin enhances incretin signaling by increasing both the plasma level of GLP-1 and expression of the glucagon-like peptide-1 receptor in the insulin-containing pancreatic β-cells. 19 In contrast, a recent study showed that metformin did not inhibit plasma dipeptidyl peptidase-4 activity either in vitro or in vivo. 20 These reports suggest that sitagliptin and metformin increase active glucagon-like peptide-1 levels through different mechanisms, which results in an additive glucose-lowering effect in combination therapy. Studies in mice showed that metformin increased plasma glucagon-like peptide-1 levels and inhibited gastric emptying at both low doses (75 and 150 mg/kg) and a high dose (300 mg/kg) but only significantly reduced hepatic glucose production at the high dose (300 mg/kg). 19 However, FPG did not differ between the two groups in the present study, so the effect of sulfonylurea on FPG needs to be considered. The mechanism underlying the dosage effect of metformin in this study was not elucidated, and defining the necessary dose of metformin for combination therapy could not be concluded from this study.
Japanese T2DM patients tend to be less obese and have lower insulin secretion compared with Western T2DM patients, 3 and sulfonylurea is commonly used for their treatment in Japan. 4 although the trend has been for the daily dose to decrease. It have been reported that glimepiride at 0.5 mg daily was safe and effective with Japanese patients with mild T2DM. 21 Also, the 2012 report of the Drug Event Monitoring of the Japan Pharmaceutical Association showed that the proportion of patients receiving ≤2 mg daily of glimepiride was 72.9%, even including 12.7% of patients with ≤0.5 mg daily in the entire description of glimepiride use in Japan. 22 Thus, a daily dose for glimepiride of 0.5 mg was not uncommon in Japan.
In pancreatic β-cells, glimepiride interacts directly with exchange protein directly activated by cyclic AMP 2, resulting in activation of Ras-proximate-1 protein in a cyclic AMP-dependent and a protein kinase A–independent manner. 23,24 Together with the closure of KATP channels via binding to the sulfonylurea receptor, 25 activation of the exchange protein directly activated by cyclic AMP 2/Ras-proximate-1 protein signaling pathway might be one of the mechanisms that underlie the glimepiride synergic stimulation of glucose-lowering effects with sitagliptin. Restoring pancreatic ATP levels by these mechanisms may recover the response to sulfonylurea. Combination therapy of sitaglitpin added to a low dose of sulfonylurea has been shown to be effective for glycemic control, 26 which is compatible with our observation that a small dose of glimepiride is necessary for improved triple OAD therapy.
In the present study, greater deterioration in fasting CPR, IRI, CPI, and HOMA-β were noted in the group who stopped sulfonylurea than in those who were treated with a reduced dose of metformin, whereas HOMA-IR and FPG did not differ between the two groups. These observations suggest that glimepiride acts to lower circulating glucose levels by stimulating insulin secretion but not by improving insulin sensitivity. This conclusion is compatible with the observed lower capacity for insulin secretion in Japanese T2DM patients. In the American Diabetes Association/European Association for the Study of Diabetes guidelines, a high dose of metformin is the first-line treatment, 1 but this in not always in the Japanese guideline. 2 We do not know whether our results may compatible with Western T2DM patients whose pathophysiology of T2DM is mainly insulin resistance. However, our results suggest that at least a small dose of glimepiride may be required for the glucose-lowering effect of sitagliptin in triple OAD therapy in Japanese T2DM patients.
There are some limitations in the present study, including the fact that it was not conducted as an add-on for existing OAD therapy. The time and order of selection of the three OADs were different for each patient in usual clinical practice. Therefore we had to choose a study design that subtracted glimepiride from triple OAD therapy after achieving satisfactory glycemic control. Another limitation was that the subjects who discontinued glimepiride were compared directly with the subjects who received a 50% reduced metformin dose. It would be preferable to divide subjects into four groups, such as those who (i) continued triple OADs, (ii) discontinued glimepiride, (iii) discontinued metformin, and (iv) reduced metformin by 50%. The existing design was chosen because of an insufficient number of patients available in a single center to use the four-group design.
In summary, glimepiride and a high dose of metformin are both necessary for improved glycemic control in T2DM patients. Sulfonylurea is required for glycemic control in triple OAD therapy with sitagliptin, metformin, and glimepiride for Japanese T2DM patients. This triple OAD regimen may be useful for patients who do not achieve satisfactory glycemic control in dual OAD therapy. Further precise analyses are necessary to identify the characteristics of patients who did not experience any deterioration in their glycemic control after discontinuing sulfonylurea or reducing metformin in this triple OAD therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.