
Abstract
Daily management challenges and declines in glycemic control are evident among youth with type 1 diabetes (T1D) as responsibility for care transitions from parent to youth. Many behavioral interventions developed for youth and their caregivers have demonstrated a small yet significant impact, and one method to potentially augment or increase their potency may be the use of mobile health strategies such as text messages. The primary aim of this systematic review was to evaluate the current literature regarding interventions incorporating text message–based interventions for youth with T1D. Feasibility was demonstrated across all text message programs, but participant satisfaction and glycated hemoglobin results were mixed. Retention rates varied, and technical difficulties were reported in several studies. Current evidence suggests that text message–based interventions that include text messages are feasible and enjoyable, but yet their clinical significance for long-term daily T1D management behaviors and glycemic control is unclear. Researchers are recommended to carefully consider the format, frequency, and timing of text message interventions and to fully test software before implementation. Future research needs include utilization of experimental designs such as randomized controlled trials, SMART design trials, and stepped wedge design trials to clarify specific medical and psychosocial outcomes, the role of caregivers/peers and incentives, and utility in clinical settings.
Introduction
A primary factor that may affect youths' glycemic control is that T1D responsibility begins to shift during adolescence. 6 Youth collaborate with their caregivers less over time, which makes it difficult for parents to monitor their child's T1D behavior and assist them with T1D problem solving when needed. 7,8 Additionally, caregiver–child conflict is common during adolescence, which may change the ways in which caregivers are involved in daily T1D care. 9 –11 Behavioral interventions are commonly used to prevent declines in adherence and glycemic control among youth with T1D, and many are at least somewhat effective, but there may be novel ways to augment the effectiveness or increase the potency of these behavioral trials. 12 –14 Interventions that endorse caregiver involvement in a way that reduces parent–child conflict and support youth in their development of T1D skills will likely result in the most robust and long-term improvements in glycemic control; the literature suggests that family cohesion is an integral part of successful T1D disease management. 15
Interventions that are grounded in behavioral theory are also likely to demonstrate long-term desired outcomes. Elements of social cognitive theory have been shown to predict health behaviors in adults and youth, 16 –18 are frequently used to guide the development of behavioral health interventions, 19 –21 and are directly applicable to youth with T1D as well. The theory purports that there are several key elements that may affect health behavior, including knowledge about the risks and benefits of specific health behaviors, perceived self-efficacy for personal control over health behavior, expectations about the costs and benefits of health behaviors, the ability to set achievable goals, social and environmental factors that may increase or decrease the probability of health behavior, and adaptability to change. 22,23 Youth develop these skills throughout adolescence and young adulthood; thus, interventions that address them during the transition of T1D care from parents to youth may be primed to impact long-term health behaviors as well.
Mobile health (mHealth) strategies may be one method to improve youths' glycemic control and psychosocial well-being within a social cognitive theoretical framework while also maintaining caregiver involvement in T1D care. The use and availability of mobile phones have rapidly increased over the past decade. A recent report by the Pew Research Center from September 2012 reported that 88% of Americans own a mobile phone, of which 55% use their phones to browse the Internet. 24 Many mobile phones users are youth, who are particularly willing and adept at using text messaging and mobile phone applications. Overall, 75% of youth send and receive text messages, with a median of 60 texts a day in 2011, a number that is steadily climbing as mobile technologies become more pervasive in youths' lives. 25 Racial differences in text messaging rates are decreasing, making this a technology that may be able to reach previously underserved populations. 25 In comparison, the frequency at which youth communicate by talking on a phone or socializing in person outside of school has decreased. 25 These estimates suggest that mobile phones may provide unique access to many health consumers and could serve as an important adjunct to other forms of intervention, such as clinic-based therapy sessions. Researchers may be able to reach youth and their caregivers during their daily activities on a platform that is already familiar to them in order to assess daily T1D behaviors, such as blood glucose levels, carbohydrate amounts, and insulin doses, and provide intervention that quickly addresses social and environmental factors that impact health behavior. Furthermore, interventions that include an mHealth component may maintain participant engagement and improve retention rates and outcomes.
Preliminary research regarding the use of mHealth technology for health management indicates it is feasible and acceptable among children and adolescents for improving adherence to immunosuppresant use among pediatric liver transplant patients, 26 promotion of sexual health, 27,28 and assessment of substance use. 29 A recent review about mHealth interventions for adults with T1D and type 2 diabetes demonstrated promising results concerning the use of text messages and mobile applications to manage daily diabetes care as well. 30 Furthermore, behavioral health interventions guided by social cognitive theory have begun to include text message components. 17,31,32 However, less information is available regarding the effectiveness of interventions that include text messages with youth with T1D. Discussion of unique childhood considerations, such as access to mHealth technology and inclusion of caregivers in interventions, is warranted.
The objective of this systematic review is to provide a comprehensive overview of the current literature regarding interventions that include text messages to promote glycemic control and well-being among youth with T1D in order to inform the development of future mHealth interventions with this population and direct their inclusion in future interventions. Specific areas to be considered in the review include description of the existing text message intervention studies for youth with T1D, synthesis of the findings from such studies, and discussion of the need for future research directions in this population.
Subjects and Methods
This systematic review was guided by the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 33 The articles selected for the current review were identified by a behavioral diabetes research fellow, two trained research assistants, and one trained medical student using the PsycINFO, PubMed, and Medline electronic databases. Combinations of the following key words were used for the initial article search: “diabetes,” “type 1 diabetes,” “SMS,” “short message service,” “mobile text,” “text message,” “telehealth,” “telemedicine,” “pediatric,” “children,” and “adolescents.” Reference sections of originally targeted articles were examined as well for additional articles to be considered for inclusion. 34 –40
Inclusion criteria for the current review were as follows: (1) a pediatric sample (age range, 0–20 years), (2) participants diagnosed with T1D, (3) an experimental or quasi-experimental study design published in a peer-reviewed journal, and (4) an intervention that included the use of text messages (Fig. 1). Abstracts that met these criteria were further reviewed, and the authors discussed any inconsistencies.
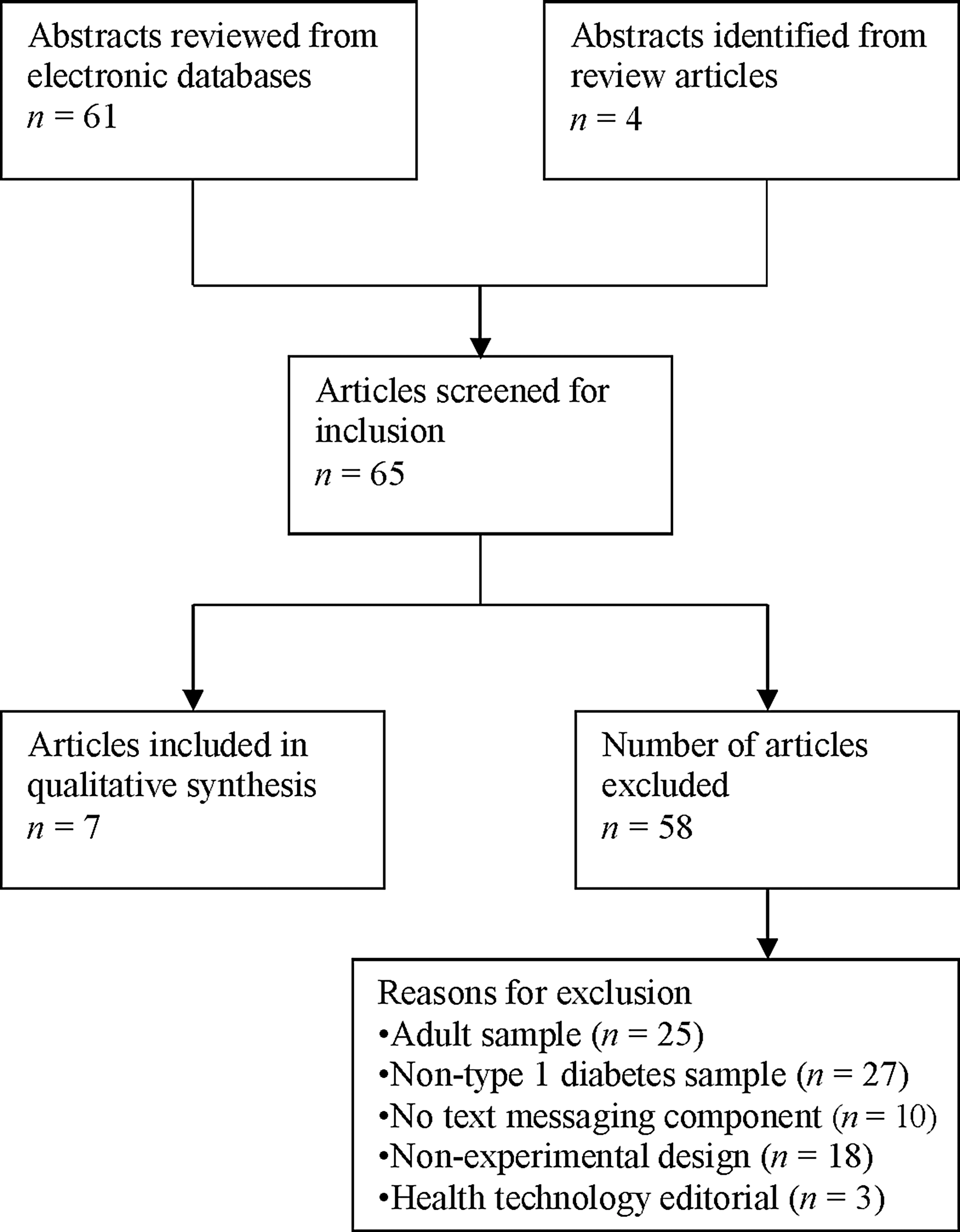
Article selection process.
Results
The initial article search yielded 61 abstracts from electronic databases and four additional abstracts from reference sections, for a total of 65 articles that were considered for inclusion. Fifty-eight articles were excluded from the final qualitative synthesis because of the following reasons: adult sample (n=25), non-T1D sample (n=27), lack of text message component (n=10), non-experimental design (n=18), or health technology editorial (n=3). Seven articles met inclusion criteria for this current review, all of which were published between 2006 and 2012. 34 –40 Table 1 gives detailed descriptions of each study.
BG, blood glucose; BMI, body mass index; HbA1c, glycated hemoglobin; RCT, randomized controlled trial; SMS, short message service; ST, Sweet Talk; SUS, System Usability Scale; T1D, type 1 diabetes; TM, telemedicine.
Sample demographics
Across reviewed studies, the average number of participants was 46 (median, 40; range, 11–92). The age range of participants was 8–25 years; only one study included participants older than 19 years of age. 40 Four studies required participants to have a T1D diagnosis for at least 1 year to participate, 35,37 –39 and two had glycated hemoglobin (HbA1c) requirements (i.e., either above or below a specific HbA1c level). 35,38 Only one study included direct caregiver involvement. 34
Study goals/design
The seven studies varied with respect to specific goals and design, but the majority were conducted in order to evaluate the feasibility and effectiveness of a text message intervention to improve glycemic control 35,37 –39 ; other studies were designed to increase blood glucose monitoring frequency 40 or physical activity 36 or to evaluate the use of text messages to provide T1D information. 34 One study noted the use of social cognitive theory as a guide for text message and study development 39 ; other studies did not reference behavioral theory.
Text message intervention duration ranged widely from 11 weeks to 12 months, with the majority involving a baseline (n=5) 35 –37,39,40 and either follow-up questionnaires (n=4) 35,36,39,40 or a follow-up interview (n=3) 34,37,38 as well. Three studies were randomized controlled trials, 36,39,40 and one was a randomized crossover trial in which intervention/conventional support group membership changed after 3 months of participation. 35 The remaining three studies were quasi-experimental studies that included all participants in each phase of the study (n=2) 34,38 or matched control participants (n=1). 37 Five of the seven articles provided information regarding mobile phone requirements. 35 –40 Three studies provided participants with a mobile phone 35,38,39 ; two also provided a prepaid phone card to cover the expense of study-related text messages. 35,39 Two studies included ownership of a text message–capable cell phone and home Internet access as a requirement for participation. 37,40
The majority of the text message interventions primarily targeted blood glucose monitoring reminders or assessment (n=4) 34,35,39,40 ; other diabetes-related text message topics included use of insulin (n=2), 34,38 nutrition and healthy eating (n=2), 34,39 physical activity (n=3), 34,36,39 barriers to adherence (n=1), 37 sick day management (n=1), 34 legal rights at school (n=1), 34 and general diabetes education (n=1). 38 Five articles included information about participants' orientation to the text message program. 35,37 –40 Specifically, participants received a verbal/automated introduction to the program (n=3), 37,38,40 were provided an instruction manual/card (n=2), 35,39 and/or attended a meeting to set T1D goals during a clinic visit (n=1). 39
Four studies only used text messages as a method of delivering educational information and behavioral reminders to participants, 34,36,37,39 but three studies included text messages as a method of T1D-related data collection as well. 35,38,40 Text message programs had varying structures and used a combination of the following: text messages created by the research team sent at predetermined times (n=4), 34,36,38,40 text messages based on personal T1D-related goals sent at predetermined times (n=3), 34,37,39 and participant-generated T1D-related daily care texts sent to the program followed by feedback sent from the medical team (n=3). 35,38,40 In five studies, text messages were not the only intervention component: changes to insulin regimen (n=1), 39 photo diaries (n=1), 38 Internet sites (n=2), 37,40 and pedometers (n=1) 36 were included as well.
Summary of findings
Each study used a unique set of outcome measures to evaluate program effectiveness and feasibility. The majority of studies measured HbA1c (n=5) 35 –39 and participant satisfaction (n=4). 34,35,37,38 Four studies assessed additional variables, including the frequency and response rate to program texts and participation in Web site diaries, 40 daily step count, body mass index, blood pressure, and quality of life, 36 social support, 39 and usability of the text message program. 38
Glycemic control outcomes varied across studies. In one study HbA1c levels decreased for the intensive insulin regimen and text message program group (10.0% at baseline, 9.2% at 12-month follow-up) but did not change for the conventional insulin regimen alone (10.1% at baseline, 10.3% at 12-month follow-up) or conventional insulin regimen and text message program groups (9.8% at baseline, 10.1% at 12-month follow-up). 39 In another study, at 3-month follow-up, HbA1c levels were maintained in the intervention group but increased in the control group (8.9% at baseline, 8.8% at 3-month follow-up in the intervention group, and 9.9% at 3-month follow-up in the control group). 37 Finally, in a third study, HbA1c levels were lower during the text message phase than at baseline or the paper diary phase (9.05% at baseline, 8.9% after the 3-month text message phase, and 9.2% after the 3-month paper diary phase). 35 The other two studies that measured HbA1c levels did not find any statistical differences. 36,38 With respect to psychosocial variables, higher self-efficacy, self-reported adherence, and social support from the diabetes team was reported by one study, 39 yet quality of life and daily step count were not affected by the text message program in another study. 36
Feasibility was demonstrated across all text message programs, but participant satisfaction was mixed. The majority of participants reported they enjoyed receiving the text messages and expressed a desire to continue receiving them, but some participants believed the texts were an intrusion in their daily routine. In the study that compared text messages with e-mail reminders, participants preferred the text messages. 40
Retention rates varied across studies (72–100%); three studies reported greater than 90% at follow-up, 35,36,38 and one study reported 100% participant retention. 35 Attrition occurred during both the intervention (n=5) 37 and at follow-up (n=2). 34,39 The greatest attrition was reported by one study in which 27.5% never used the e-mail/cell phone system and 73% stopped using the e-mail/cell phone system by the third month. 40 In another study, 37% of participants discontinued pedometer use, which meant they also no longer received the text message intervention. 36 Other studies did not provide details regarding reasons for attrition. Over half of the articles (n=4) reported technical problems that led to data loss and/or affected participant motivation. 34,35,37,38
Discussion
The objective of this review was to identify published studies that used a text message–based intervention designed for youth with T1D. Although the number of youth who engage in daily text message activity is high, which suggests that youth may use and benefit from such programs, there were only seven studies that met inclusion criteria; other studies were excluded primarily because they were not conducted with children and/or did not include a T1D population. The studies in this review indicate that interventions that include a text message component are, indeed, feasible and that youth enjoy participating in them, but it remains unclear whether or not these programs have an overall long-term influence on daily T1D management behaviors and/or glycemic control (e.g., HbA1c). Of the five studies that measured HbA1c levels, one reported statistically significant decreases in an intensive insulin plus text message intervention group only, 39 one reported statistically significant changes that were not clinically significant, 35 another reported stable HbA1c levels for the intervention group, 37 and the other two did not find any differences between groups or pre-/post-intervention. 36,38 That varying HbA1c outcomes were reported is not surprising. HbA1c measures glycemic control over a period of several months; thus, the length of these interventions may not have been sufficient to impact youth's T1D behaviors and, consequently, would not detect clinically significant change in HbA1c levels or identify patterns of changes in glycemic control over time. The methodological rigor of these studies varied as well, as not all were randomized trials, many included multiple intervention components, and only one was based on behavioral theory, which complicates the interpretation of aggregated findings. Additional assessment regarding the clinical utility of text message–based interventions is needed before it is possible to conclude that text message interventions are or are not effective at maintaining or decreasing HbA1c levels among youth with T1D.
Strengths of text message programs
This review suggests there may be many benefits to developing and including text message interventions for youth with T1D. Many authors cited cost-effectiveness and ease of use as considerable strengths because the majority of youth already have cell phones with text capabilities, are knowledgeable about text message functioning, and require little instruction on how to use a diabetes-related text message program. Additionally, texting is already a part of most youths' daily activities and requires minimal time to read and respond; thus, these programs may be less intrusive and easier to introduce into routine behavior than interventions that interrupt daily life (e.g., intervention sessions at clinic appointments, answering questionnaires with a research assistant by telephone). Collectively, by reducing barriers to participation (e.g., traditional in-person interventions), youths' participation is promoted, and higher retention rates are likely. Furthermore, text message programs can serve as both assessment and intervention tools, as demonstrated by these studies, and give researchers and clinicians access to data about T1D behavior in the moment it occurs, rather than requiring youth to recall information at a later time, and the automated structure can be easily incorporated into clinical practice.
Limitations to text message programs
Despite the aforementioned strengths, limitations remain to the incorporation of text messages into intervention programs. Foremost are technological limitations. Even with daily technology advances, hardware and software problems occur, which may affect participation and data collection. Consistent program malfunctions may result in high attrition if participants are frustrated or confused, and data may be lost if participants' phones, the cell phone network, and/or the text message software do not work. It is notable that both participant attrition and data loss due to software malfunctions were reported in several studies. Another technological limitation is that not all text message programs enable researchers to track whether or not texts are both received and read by participants. Without this information, it is impossible to measure treatment dose and comprehensively evaluate the feasibility, satisfaction, and effectiveness of the intervention.
Another limitation is the rapid pace at which technology develops; technological adaptations and advances are made every day. Therefore, although text messages are the most popular form of communication among youth currently, future technology will affect the relevance and success of a text message intervention program. The development of modern technological interventions is always a moving target, and text message programs will need to adapt and upgrade in order to remain applicable and interesting to this population. That being said, technological advances may also offer opportunities to develop text message intervention programs that provide greater personalization, social networking features, and/or advanced researcher tracking features, which may elicit greater user satisfaction and promote more robust health outcome changes.
Limitations to the text message literature
There are also limitations to the design of these studies that affect the generalizability of the findings. Some text message programs were only compatible with specific cell phone brands (e.g., one study implemented an application that was strictly compatible with the HTC 2 mobile phone 38 ), which limited sample size and diversity, and there were general inclusion criteria constraints (i.e., requiring an unlimited text message cell phone plan or consistent access to e-mail, phone memory limits) that likely resulted in a biased, affluent sample. Furthermore, most studies had brief intervention periods, ranging from 3 to 12 months, only two studies included control groups, 36,37 and only two studies included text messages as the only intervention mode. 34,35 Brief interventions, interventions without a control group, and interventions that include more than one component (especially changes in insulin regimen) are difficult to assess for overall and long-term impact on glycemic control, and it is difficult to determine if youth would continue to use diabetes-related text message programs beyond the intervention period. Without this information, it remains unclear if these programs are feasible and beneficial for this population. Larger studies, grounded in behavioral theory, that use an experimental design, such as the randomized controlled trial, SMART trial, or stepped wedge trial designs, to assess the use of text messages are needed in order to assess the potency and long-term impact of text message interventions. Furthermore, trials that incorporate text message interventions into T1D interventions for youth that are already proven to be effective could determine whether or not their inclusion increases the impact of the overall intervention.
Additional considerations for future research
There are many additional research questions regarding the use of text message interventions with the pediatric T1D population that need to be addressed. For instance, as this is a young target population, it is likely that the majority of health care is still monitored by a parent or other primary caregiver. Therefore, including a caregiver in future text message programs may be beneficial, particularly because youth transition from parental care to self-care during adolescence. Only one study in this review involved caregivers in the text message program, 34 and few details were provided about their role. Similarly, as peers play a dominant role in youth behavior, it may be informative to involve peers and friends as well. However, the recommended role of a caregiver/peer in a diabetes-related text message program is unclear and warrants discussion. For example, caregivers/peers could receive the same texts as youth with T1D, or it may be beneficial to send texts that address different aspects of daily T1D care. Alternatively, text message interventions could be developed for caregivers of young children who do not have cell phones.
Furthermore, because of the participants' age range (8–20 years), the timing of text messages with respect to school becomes a principal issue. Many U.S. schools prohibit cell phone use during the school day, including during free periods and at lunch. If such rules exist, the timing of text messages must be personalized to accommodate these schedules. Youth are also likely to have varying patterns of text message use depending on the time of year (i.e., during the academic school year versus summer). In fact, for this review, the study with the highest attrition rate was conducted during the summer, which the authors noted could have affected participation. Alternatively, caregivers may use cell phones as a form of reward or punishment, and the effectiveness of a diabetes-related text message program will be compromised if youths' phone privileges are revoked. Another consideration is the incentive process: should participants be compensated for their participation in a diabetes-related text message program, and if so, in what way? The majority of these studies included temporary cell phone access, a phone card, or compensation for text message costs as incentives, which makes it difficult to ascertain participants' motivation for completing the study. If participants only agreed to participate to gain access to a phone, findings regarding feasibility may be inflated. In general, incentives that encourage participant recruitment, but are not the primary reason for participation, are recommended.
The content of diabetes-related text message programs is likely to include queries about participants' medical and mental health information (e.g., blood glucose monitoring, carbohydrate counting, physical activity, mood, etc.). As youth are likely to experience stress and complications during adolescence, researchers need to establish guidelines about how to handle information received by text that requires clinical action. For instance, if participants report consistently high or low blood glucose levels that raise concerns about their current health and long-term care, is the research team ethically bound to intervene, and if so, in what way? Other studies have mentioned the need to investigate the best way to handle information requiring clinical action as well, 41 and, of those studies that include two-way text messaging, most programs provide tailored, computer-automated responses. For example, in a study conducted with women diagnosed with bulimia, a complex computer algorithm evaluated symptom patterns and suggested several appropriate texts for the research assistant to send to the participant, whereas in a study with hazardous drinkers, participants were automatically sent specific goals and strategies to reduce their drinking based on a threshold high number of drinks they reported consuming. 42,43 Regardless of the research team's decisions regarding these situations, guidelines need to be established prior to recruitment and fully explained to participants.
There are also questions about the actual functionality of such programs in clinical practice and daily life. The studies in this review introduced diabetes-related topics, including blood glucose monitoring, insulin use, physical activity, nutrition, and sick day management. When such topics are presented it may be necessary to extend involvement to a larger multidisciplinary team, including registered dieticians, nurse educators, physicians, and psychologists and, thus, expert opinions on all subject matter. However, the involvement of so many healthcare professionals may become costly, time consuming, and, depending on available resources, simply unattainable. Decisions regarding the continued role of these experts in the text message programs need to be addressed as well. Healthcare professionals will need to decide if they want to be “on call” to address participants' immediate concerns.
Recommendations
Researchers who plan to develop text message studies for youth with T1D are encouraged to fully evaluate the specific behavior change goals of the intervention program and select a guiding behavioral theory prior to implementation in order to build on prior successful interventions and increase participant engagement and retention. The timing and frequency of the targeted behaviors will affect the structure and content of text messages and may affect their effectiveness. For example, blood glucose checks are likely to occur before/after meals and physical activity, so a program intended to increase blood glucose checking may be most effective if text messages are sent around these times, especially if the program can be tailored for individual families' schedules.
Careful consideration should be given to the frequency of text messages as well. If texts are too frequent, participants may be less inclined to respond; on the other hand, texts that are too infrequent may not encourage engagement with the system or the research project. It is notable that one of the reviewed studies recommended avoiding excessive intrusion in daily activities; 34 another study stated that more frequent text messages may have sustained interest in the program. 36 The need for individual tailoring has been noted in other studies as well and was highlighted by a study for human immunodeficiency virus medication adherence in which participants expressed varying preferences with respect to receiving two versus four texts a day and whether or not texts were delivered 15 min before medication was scheduled versus the exact time medication was scheduled. 44
The structure of the text message program may impact engagement and retention as well. Programs that include two-way text message capabilities and/or access to a medical professional may encourage participation and increase effectiveness because participants receive immediate benefit from their interaction with the program. Finally, it is recommended that text message programs be fully tested prior to implementation because such testing will allow for identification of software problems before they impact participant engagement with the program.
Conclusions
Given the small number and wide variability of text message intervention studies with the pediatric T1D population, there is a great need for additional research to more thoroughly evaluate the potential of mHealth technologies as an intervention modality. Steadily increasing numbers of youth use text messages as their predominant means of communication, so it is important for future research to include larger sample sizes that promote generalizability. In much the same way, it is important to incorporate participants who are not tech-savvy in order to obtain realistic results regarding use and sustainability. As text messages are a communication tool used across all races, ethnicities, and socioeconomic statuses, there should be ample opportunity to explore generalizability in future studies.
The overwhelming presence of mobile phones in today's society suggests that text messages may be a valuable health behavior change tool. Although the reviewed articles provide mixed results regarding the effectiveness of text message interventions with respect to daily T1D management behaviors and glycemic control and include generally small, middle-class and above samples, they did demonstrate their feasibility and high levels of participant satisfaction, suggesting that additional research regarding text message interventions is both feasible and warranted. Further research needs include the implementation of studies that utilize experimental designs and are grounded in behavioral theory to clarify specific medical and psychosocial outcomes, examination of the role of caregivers/peers and incentives, and ultimately implementation among clinical settings.
Footnotes
Acknowledgments
The authors would like to thank Lindsey O'Brecht for literature review assistance and Maureen Monaghan, PhD, and Marisa Hilliard, PhD, for manuscript review.
Author Disclosure Statement
No competing financial interests exist.