
Abstract
Background:
Type 2 diabetes mellitus (T2DM) and obesity are often associated in the same metabolic pathology and represent a significant public health problem. Although laparoscopic sleeve gastrectomy (LSG) is a relatively recent technique of bariatric surgery, it has shown to be efficient and safe and has obtained much support from physicians and patients. Several studies have highlighted the effects in terms of resolution and improvement of diabetes.
Subjects and Methods:
From January 2009 to November 2012, 15 patients in Obesity Class II (body mass index [BMI], 37.9±1.5 kg/m2; baseline weight, 102.7±11.6 kg) with uncontrolled T2DM despite taking a glucose-lowering drug therapy (glycated hemoglobin [HbA1c], 8.1±0.6%) underwent LSG and advanced practice medical management in accordance with the American Diabetes Association guidelines. All patients were subjected to follow-up controls with anthropometric and metabolic indices at 5, 15, 30, and 60 days, and at 6 and 12 months after surgery, remission of diabetes was also evaluated.
Results:
At 1 year after surgery, the mean excess weight loss percentage (EWL%) was 58.4%, and the mean BMI had decreased from the preoperative value of 37.9 kg/m2 to 30.4 kg/m2. The average reduction in HbA1c was 2.5 (30.9%). The mean homeostatic model assessment of insulin resistance decreased from 13.3 to 4.9. Overall, during the period of observation, four patients (26.7%) had started drug therapy again, six patients had complete remission (40%), and five patients had partial remission (33.3%).
Conclusions:
LSG not only makes it possible to attain a significant EWL% in obese patients, but also a remission or improvement of diabetes. Further studies are required to determine the duration of the effect and the role of different factors involved.
Introduction
Literature gives evidence that bariatric surgery can determine the treatment of both obesity and T2DM. 5 Buchwald et al., 6 in their systematic review and meta-analysis, compared the different surgical techniques bringing the 95.1% resolution of T2DM in patients undergoing biliopancreatic diversion/duodenal switch, followed by gastric bypass (80.3%), gastroplasty (79.7%), and laparoscopic adjustable gastric banding (56.7%). In 2000, Ren et al. 7 published the first laparoscopic duodenal switch; however, they noted that patients with superobesity had a high rate of complications and thus decided to divide the two-step procedure starting with a laparoscopic sleeve gastrectomy (LSG) and then completing with a bypass. It was observed that, by itself, the LSG determined adequate weight loss, and so this procedure has spread rapidly around the world and was approved by three International Consensus Summits.
Currently, the LSG has gained consensus not only among physicians but also among patients because of its efficacy and no significant postoperative morbidity. Yet, there are few studies that show the results on T2DM, although the first data, relative to follow-up in the short and medium term, are interesting and show rapid resolution or improvement of T2DM in 65–85% of patients. 8 Moreover, rapid changes in glycemic indices and a significant reduction of insulin resistance (homeostatic model assessment of insulin resistance [HOMA-IR]) in the immediate postoperative period have led to the hypothesis the action of mechanisms independent from the weight loss. 9 The objective of this study is to evaluate the effectiveness of LSG in Obesity Class II diabetes patients (body mass index [BMI], 35.0–39.9 kg/m2) in terms of complete or partial resolution of T2DM in light of recent ADA guidelines and to report variations in parameters related to glucidic metabolism in relation with the reduction of weight.
Subjects and Methods
From January 2009 to November 2012, at the Department of Digestive Surgery and the Multidisciplinary Centre for Obesity of St. Maria Hospital, Terni, Italy, 15 (male:female, 5:10; mean age, 58.8±2.8 years) non-morbidly obese patients (mean BMI, 37.9±1.5 kg/m2) in Obesity Class II according to the NHLBI classification 4 and with uncontrolled T2DM despite taking oral hypoglycemic therapy (mean glycated hemoglobin [HbA1c], 8.1±0.6%) underwent LSG surgery and advanced practice medical management according to the ADA and NHLBI guidelines. 3,4
Following the indications of the ADA–European Association for the Study of Diabetes on the algorithm for the initiation and adjustment of therapy, 10 before the surgical option was proposed, patients were subjected to monotherapy with metformin in combination with lifestyle changes. Metformin is easy to use without causing hypoglycemia and in obese patients allows either weight stability or modest weight loss, in contrast with many other blood glucose-lowering drugs. The dosage scheme was as follows: the patients started taking low doses of metformin (500 mg) once or twice daily or 850 mg once a day. After 10 days, and if there were no adverse events, the dose was increased to 850 mg twice daily. The maximum effective dose administered was 1,000 mg twice daily.
In accordance with the guidelines of the ADA, patients enrolled in the study were referred for surgery after the failure of biochemical control of diabetes was confirmed, with a simultaneous increase in weight resulting from the failure of lifestyle interventions (duration of medical behavioral therapy, 2.3±1.1 years). At this stage, an integrated team of specialists, including the internist, nutritionist, endocrinologist, psychologist, and bariatric surgeon, evaluated all patients in the study.
As a preliminary, in one or more sessions, there was an interview during which the medical history of patients, including personal and weight history information, was collected, and a dietary and psychological assessment was performed (Eating Disorder Examination Questionnaire, Minnesota Multiphasic Personality Inventory, Communication and Insights Analysis Questionnaire, and stress balance). Then we proceeded to the physical examination and the study of anthropometric data and carried out blood tests for the study of the metabolic picture. Each clinical case was jointly discussed, and, before proceeding with the surgical option, all subjects underwent cardiologic, pulmonary, and anesthesia testing. The patients signed a written consent after being thoroughly informed of their medical condition and the treatment options proposed.
The inclusion criteria for this study were as follows: history of T2DM with a diagnosis of at least 1 year and that was poorly controlled (HbA1c >7%) with a BMI of <40 kg/m2 but ≥35 kg/m2. Blood samples for the analysis of blood glucose and insulin were performed in the patients after fasting of at least 8 h. HOMA-IR was used to assess insulin resistance, considering normal values to not be higher than 2.5. 11
Follow-up
Patients were subjected to periodic laboratory testing and anthropometric indices. The excess weight percentage and the excess weight loss percentage (EWL%) were calculated considering a BMI of 25 kg/m2 as the reference standard. Furthermore, a specific follow-up for evaluation of the early change of the diabetes state was conducted at 5, 15, 30, and 60 days and 6 and 12 months after surgery. The latter was based on clinical examination and analysis of blood chemistry parameters compared with their preoperative values (HbA1c, fasting glycemia and insulin, and HOMA-IR).
The remission of T2DM has been certified according to the ADA criteria 12 during the entire period of observation.
Surgical procedure
Pneumoperitoneum is created with a Veress needle in the left subcostal region. An optical trocar and three operative trocars of 12 mm were placed. Marking is performed on the large gastric curve at 6 cm from the pylorus. From this site, progressive skeletrization of the greater curvature is done with an ultrasonic scalpel. After placement of an orogastric probe (32 French), the stomach is vertically sectioned and sutured (sleeve resection). The suture is sealed with methylene blue.
Statistical analysis
Data were analyzed with a statistical computer software (MedCalc [Ostend, Belgium] software version 12.2.1).
Patient characteristics were expressed as mean±SD values and medians for continuous data and as frequencies for categorical data. Student's t tests were used to compare data before and after surgery. Spearman's correlation was applied to assess a correlation between two variables. Kaplan–Meier survival analysis was used to evaluate the different time at which patients have started complete remission after surgery. A value of P<0.05 was considered to define the results as statistically significant.
Results
The general and anthropometric characteristics of the patients are shown in Table 1 along with the type of therapy used and the presurgery metabolic indices. All surgical procedures were performed using the minimally invasive laparoscopic technique, and none of the interventions was converted to open surgery. The median operative time was 97.6 min (range, 80–125 min), no intraoperative complications occurred, the estimated intraoperative bleeding was negligible (mean, 105 mL; range, 90–135 mL), and transfusions were not required in the perioperative period.
BMI, body mass index; DM, diabetes mellitus; EW (%), excess weight percentage; F, female; HbA1c, glycated hemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; M, male.
In all patients, the hospital stay was very short and smooth and was structured according to the following scheme. During the first postoperative day, the Visual Analog Scale score was administered to score for pain (median, 3). 13 On Day 2, the oral intake of liquids was resumed. On Day 4, iopamidol (Gastromiro®; Bracco, Milan, Italy) was applied to assess the correct gastrointestinal transit, and the patients started a first light feeding. On Day 5, we proceeded to evaluate postoperative metabolic parameters according to the criteria considered in the study. The mean hospital stay was 5.8 days (range, 5–7 days), and physical examination at discharge showed a not painful, palpable abdomen and normal bowel functioning. There were no major postoperative complications (bleeding, fistula, or stenosis) or reoperations, and there was a rapid return to daily activities without any limitation in all patients, which was demonstrated through the Short Form-12 Assessment Scale. 14 This questionnaire was administered to patients in clinical monitoring performed one month after surgery.
Table 2 summarizes the results of the main outcomes analyzed. The mean EWL% was 2.7±1%, 13.4±4.9%, 27.5±8.8%, 39.6±9.6%, 45.2±10.7%, and 58.4±9.9%, respectively, at 5, 15, 30, and 60 days and 6 and 12 months. The mean BMI in the corresponding observation intervals was, respectively, 37.6±1.6 kg/m2, 36.2±1.8 kg/m2, 34.4±1.9 kg/m2, 32.8±1.9 kg/m2, 32.2±2 kg/m2, and 30.4±1.8 kg/m2. The mean HbA1c was 7.9±0.7%, 7.6±0.7%, 7.1±0.7%, 6.1±0.6%, 5.9±0.6%, and 5.6±0.6%, respectively.
P<0.05 compared with preoperative value.
BMI, body mass index; HbA1c, glycated hemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance.
Figure 1 shows the variations of the anthropometric and metabolic indices, which highlight the significant difference between the preoperative values and those obtained at the end of the observation period.
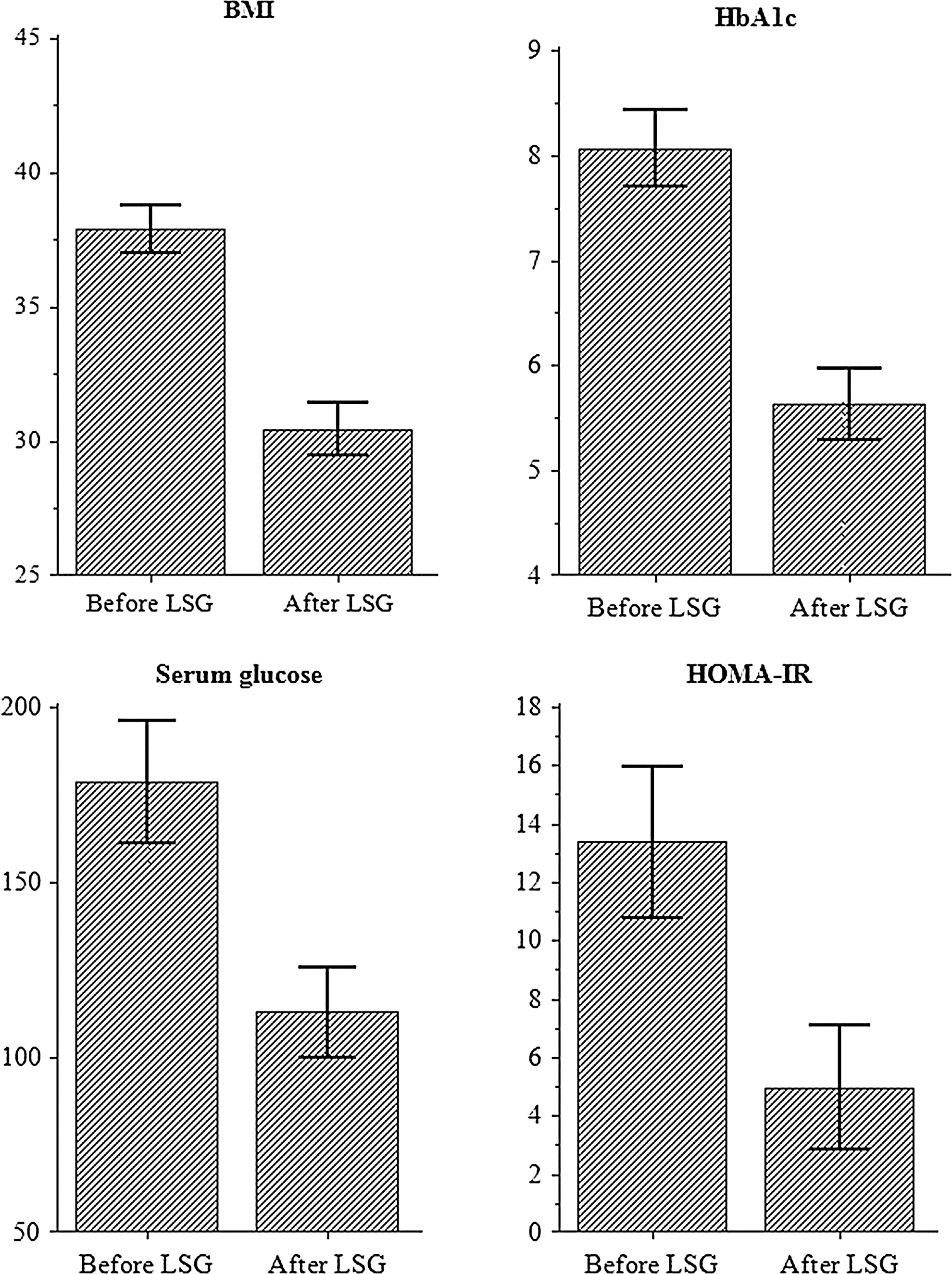
Comparison between preoperative values and results 1 year after laparoscopic sleeve gastrectomy (LSG) of the main anthropometric and metabolic indices: body mass index (BMI), glycated hemoglobin (HbA1c), serum glucose level, and homeostatic model assessment of insulin resistance (HOMA-IR). Data are mean±SD values. P<0.001.
One year after LSG, the average reduction in HbA1c was 2.5 (30.9%). Figure 2 shows the trend of the average reduction of BMI in relation to the decrease in HbA1c at different time periods.
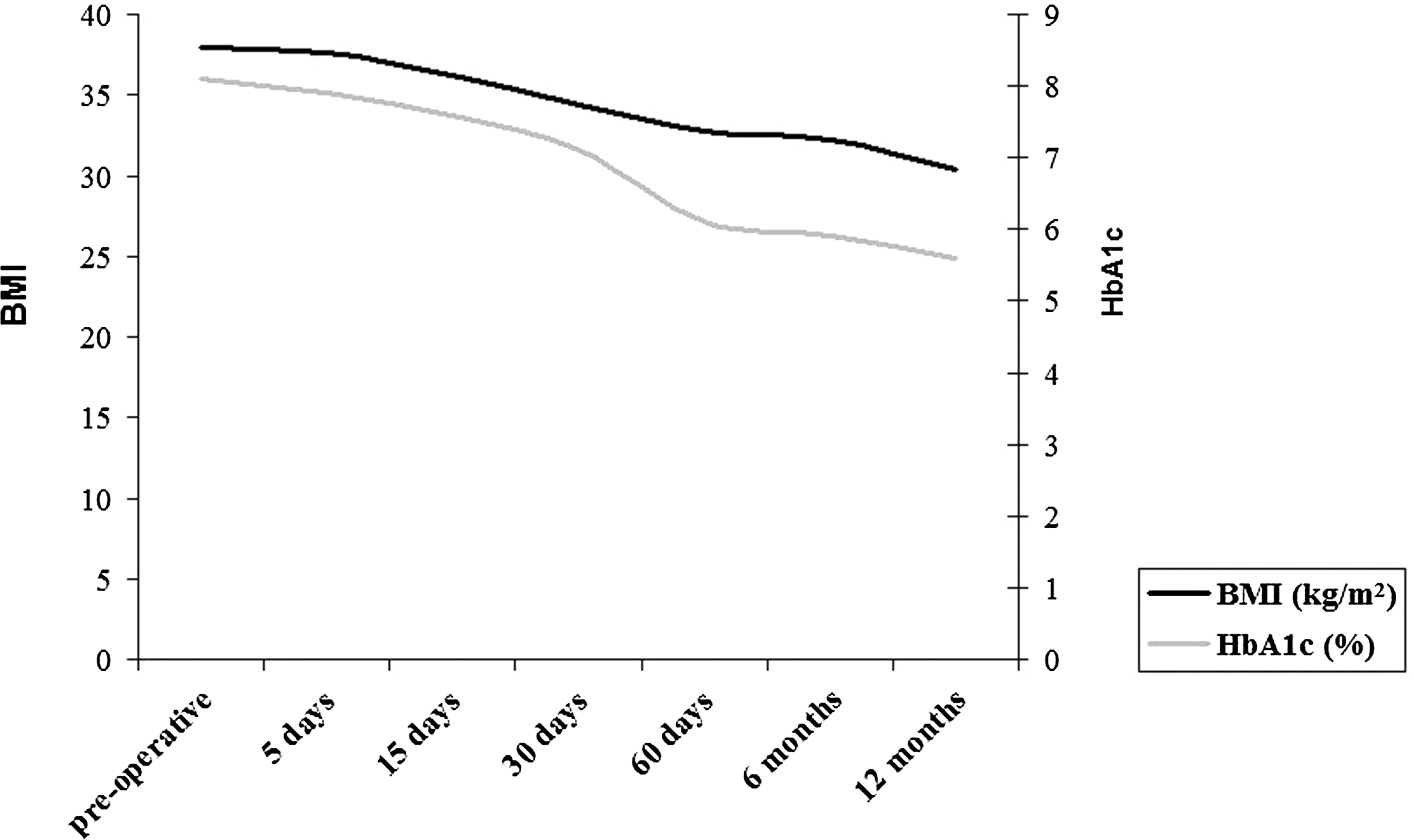
Change in body mass index (BMI) and glycated hemoglobin (HbA1c) at different time periods during follow-up.
Blood glucose, insulin, and HOMA-IR compared with preoperative values significantly improved starting on postoperative Day 5 (P<0.01) and were kept at lower levels during subsequent controls, whereas differences were not significant, in the short observation period, regarding the anthropometric index variations (P=0.5). At 30 and 60 days after surgery, blood glucose, insulin, and HOMA-IR remained substantially stable compared with a significant weight loss (EWL%, 27.5±8.8% and 39.6±9.6%, respectively) and lower BMI (P<0.01).
Figure 3 shows a poor correlation between BMI and HOMA-IR and a relative variability in terms of remission (represented by the shading of the circles). This observation, in spite of the small sample involved, shows that regardless of the metabolic and anthropometric baselines, several additional factors, which should be explored in future studies, influence and participate in the remission of diabetes.

Correlation between homeostatic model assessment of insulin resistance (HOMA IR) and body mass index (BMI) (r=−0.1; P=0.7): black circles, patients with complete remission; gray circles, patients with partial remission; and open circles, patients without remission.
During the period of observation, four patients (26.7%) resumed drug therapy with oral hypoglycemic agents (three after 30 days and one after 60 days), whereas the other 11 patients maintained the normalization of metabolic indices without the use of drugs: six (40%) had a complete remission (Fig. 4), and five (33.3%) showed partial remission.
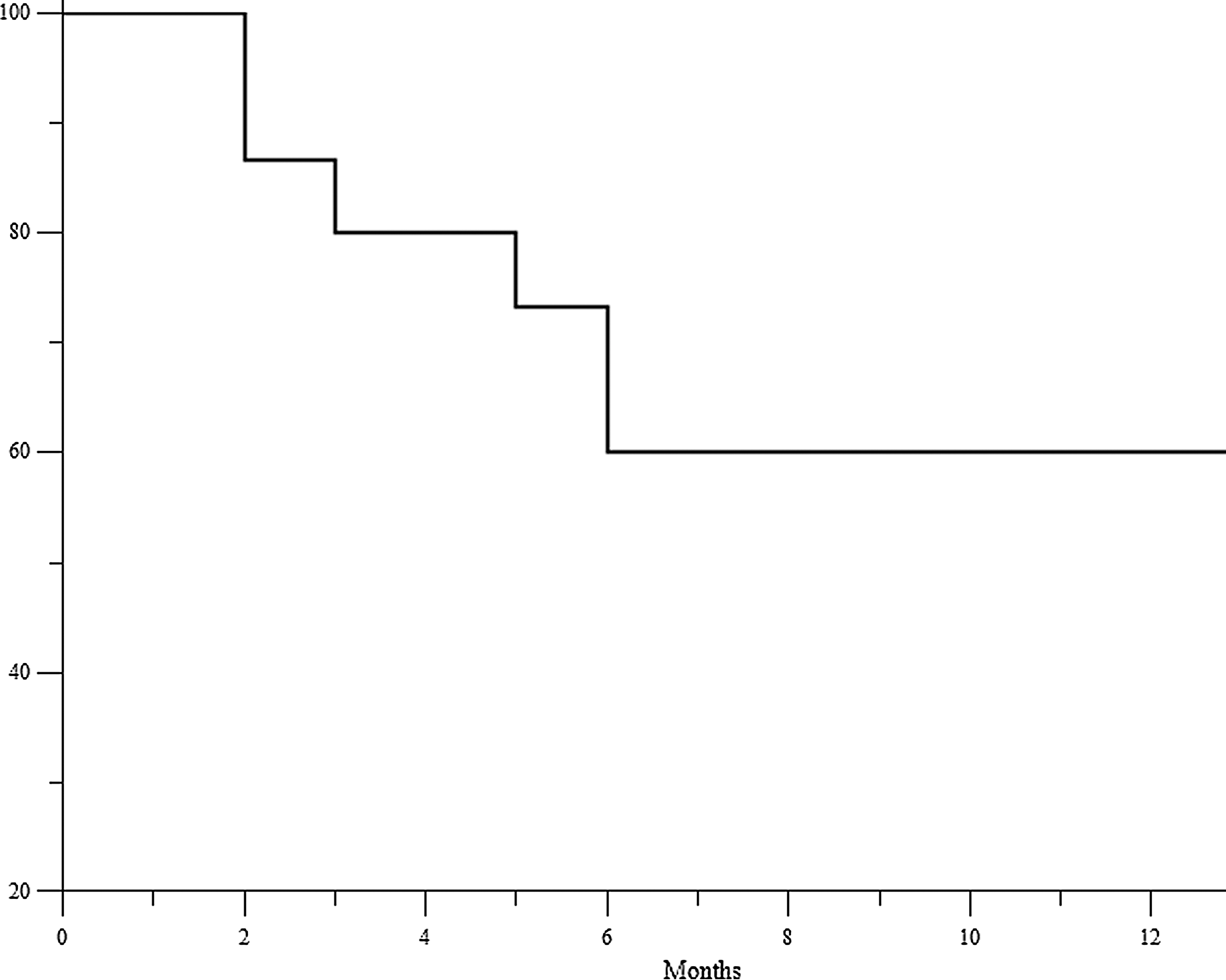
Kaplan–Meier curve estimates of different times at which patients started complete remission after surgery (glycated hemoglobin <6% and fasting glucose <100 mg/dL).
In the subgroup of patients who went into complete or partial remission, there was a significant reduction in BMI (mean reduction, 7.4 kg/m2; 95% confidence interval 6–8.8; P<0.001), and at the same time there was a lower insulin resistance (mean HOMA-IR reduction, 9.2; 95% confidence interval 6.6–11.8; P<0.001) and better control of glucose metabolism (mean HbA1c reduction, 2.6; 95% confidence interval 2.2–3; P<0.001). Analyzing the subgroup of patients who resumed drug therapy, even if they have not gone into remission, there was a significant improvement of diabetes that brought all patients into the HbA1c range recommended by the ADA 3 for an adequate control of diabetes, compared with largely higher values noted preoperatively (mean HbA1c reduction, 2.1; 95% confidence interval 1.4–2.8; P<0.001).
Discussion
The prevalence of T2DM in association with varying degrees of obesity has increased dramatically in the last decade and tends to involve lower age groups. 15 This condition is the result of a complex interaction of genetic, environmental, and lifestyle factors. There are three characteristic physiologic abnormalities: impaired insulin secretion, peripheral insulin resistance, and excessive hepatic glucose production. There are various stages of the disease, from compensatory hyperinsulinemia to glucose intolerance, with an elevation of postprandial blood glucose levels to the reduction of basal insulin levels with fasting hyperglycemia.
Currently, according to the indications of the ADA, 3 bariatric surgery for the treatment of T2DM can be considered in patients with a BMI of >35 kg/m2 if diabetes is associated with comorbidities or is difficult to control with medication. LSG, which was designed as the first phase of biliopancreatic diversion, has been established in the last few years. Currently, in our Institute, this is the most common procedure performed because of its effectiveness and safety and the consensus found among patients.
Several studies are reported in the literature that highlight the characteristics and advantages of LSG over other more challenging surgeries. Vidal et al. 16 have reported that the LSG is associated with a high rate of resolution of T2DM at 4 months after surgery and with values comparable to gastric bypass (51.4% and 62%, respectively; P=0.3). At 12 months, patients with resolution of T2DM were 33 of 39 (84.6%) in the LSG and 44 of 52 (84.6%) in the gastric bypass group (P=0.6). In the recent randomized controlled trial of Schauer et al., 17 the primary outcome in the control and remission of diabetes did not reach a significant difference between the two procedures (P=0.6). Moreover, Cutolo et al. 18 noted the significant difference in comorbidity with a higher incidence of peri- and postoperative complications of gastric bypass compared with LSG (31.2% vs. 6.6%).
The study conducted in our Multidisciplinary Centre for Obesity shows the results obtained in the first 15 diabetes patients with moderate obesity who underwent LSG. The data obtained during follow-up seem to confirm the evidence available in the literature regarding the effectiveness of bariatric surgery in the treatment of obese patients with T2DM. In fact, we noted a significant and early reduction (5 days after surgery) of HOMA-IR, indicating a rapid and significant improvement in insulin sensitivity (ΔHOMA-IR, 9.6±3.9; 95% confidence interval 7.4–11.8; P<0.01), obviously not correlated to weight loss in this early stage. From Day 15 to Day 90 after LSG, the HOMA-IR values were significantly and consistently lower than the preoperative data (P<0.01). On the other hand, weight loss began to be relevant beginning from 60 days after surgery. These observations suggest the influence of a non–weight loss-related mechanism on the normalization of glycemic indexes.
Many researchers have analyzed changes in insulin resistance and β-cell function after the execution of different types of bariatric procedures. The HOMA-IR allows us to express insulin resistance by simply determining blood glucose and fasting insulin, so this measure is frequently used.
A recent meta-analysis 19 on the subject showed the percentage decrease in HOMA-IR within 2 weeks from bariatric surgery was equal to 33.48±5.78 and that at 1 year was 44.91±7.98. From the analysis of subgroups it emerges that Roux-en-Y gastric bypass results in a net improvement of insulin resistance (54.96±21.27% at 1 year) that is statistically significant compared with predominantly restrictive surgery (laparoscopic adjustable gastric banding). This observation is in line with the study by Ferrannini and Mingrone, 20 which suggests that surgical procedures that greatly restrain food intake (Roux-en-Y gastric bypass) or absorption (biliopancreatic diversion) induce some recovery of insulin sensitivity before any large weight loss has occurred, compared with mainly restrictive procedures.
However, LSG requires special attention, and further studies should clarify the actual impact of this technique on insulin resistance. In fact, in some studies 21 as well as in our series, LSG has been shown to improve insulin resistance in the early days and weeks after surgery, when no weight change had taken place, but substantial stability was observed after a few months, by which time a significant reduction in BMI was detected. This result, coupled with the fact that LSG produces an increase in postprandial insulin and glucagon-like peptide-1 levels similar to Roux-en-Y gastric bypass, determines an effect that you would not expect from restrictive procedures alone.
The relative importance of the different factors that contribute to the improvement of insulin resistance, the timing of their action, and their interdependence is still open to debate. Caloric restriction, weight loss, and functional changes in the enteroinsular axis are all possible mechanisms. Gumbs et al. 22 suggested that the improvement in insulin resistance after bariatric surgery is due to the reduction of the stimulation of the enteroinsular axis induced by caloric restriction in the short term and by weight loss in the long term. Rubino and Gagner 23 showed that insulin action and the function of pancreatic β-cells are both influenced by hormonal signals originating in the gastrointestinal tract that change after bariatric surgery.
The role of LSG in the improvement and resolution of T2DM has been the subject of many studies and theories, which are still being analyzed. The positive effect of this technique seems to be linked to the extended resection of the gastric fundus, which could in itself result in metabolic changes. Ghrelin, produced mainly in this region of the stomach, inhibits the release of insulin-induced glucose, and it has been shown that the plasma concentrations of this hormone are closely related to the amount of ghrelin-secreting cells that are removed surgically. 24 In experimental studies, 25,26 it was observed that, after LSG, the reduction of ghrelin levels is associated with a simultaneous increase, both during fasting and postprandial, of levels of peptide YY and glucagon-like peptide-1, both secreted by the L intestinal cells in response to food intake. Glucagon-like peptide-1 exerts a trophic mechanism on the β-pancreatic cells by stimulating the biosynthesis of insulin. In addition to the insulinotropic effect, glucagon-like peptide-1 exerts a glucose-lowering effect through inhibition of gastric emptying, the restoration of sensitivity to insulin, and the inhibition of glucagon secretion with consequent reduction of hepatic glucose production. Thus, LSG seems to have metabolic action, but all the mechanisms hypothesized require further tests and trials.
The results of the cases already reported in the literature, as well as that of our center, are encouraging. In light of these clinical and experimental data, researchers have described their results by considering diabetes remission as the primary outcome without, however, adopting the evaluation criteria shared and thus creating confusion. In 2009, the ADA found it necessary to clarify the definition of remission. 12 Despite this, there are few studies that consider and report the ADA guidelines in the literature. Remission is defined by the constant permanence of blood glucose levels below the diabetes range and in the absence of antidiabetes treatment in place. It may be considered partial or complete. Partial remission is characterized by the presence of subdiabetes hyperglycemia (HbA1c not diagnostic of diabetes, <6.5%; fasting glucose, 100–125 mg/dL) for at least 1 year in the absence of drug therapy. Complete remission is the return to the normal range of glucose metabolism (HbA1c, <6%; fasting glucose, <100 mg/dL) for at least 1 year in the absence of therapy. Prolonged remission is the complete remission lasting more than 5 years.
In our study, we have taken into account these criteria. During the period of observation, 73.3% of the patients completely suspended taking oral hypoglycemic therapy started prior to surgery with a complete remission of 40%. Partial remission was observed in 33.3%, whereas there was a failure of remission in 26.7% of cases. In the latter group, patients, despite having taken the previous therapy with metformin, gained control of the glycemic index (HbA1c, <7% according to ADA recommendations) with a reduction of drug dosing.
Several observational studies 27 reported extremely variable remission rates (from 55% to 95%), and these are often determined without biochemical evidence (levels of HbA1c or fasting plasma glucose) or through the use of much less restrictive definitions (e.g., fasting plasma glucose of ≤125 mg/dL).
The factors that led a quarter of the patients in our study to resume drug therapy are not fully understood, and further trials are needed to determine these with larger patient samples. However, several current studies have emphasized the importance of β-cell functionality at the time of surgery as a major predictor of a favorable remission of diabetes. 28
The limitations of our study are those inherent to a retrospective analysis with data that were collected in a clinical setting and conducted on the basis of the documentation coming from the database of our Institute and the interview given to patients. The study is based on a small number of subjects and on a follow-up in the short to medium term. However, the volume of our series does not seem to differ significantly from the population of patients enrolled in other reports available in the literature, probably because of its recent consideration of the role of metabolic LSG. However, this is a limitation of single-center trials, and we hope the organization of multicenter studies can bring together the experience of more specialized institutions within the guidelines of a shared protocol.
Given the importance of the subject, which could potentially revolutionize, in the foreseeable future, the treatment algorithm of obese patients with T2DM, we find that it is important to plan randomized clinical trials and the stratification of patients according to the different classes of BMI and duration of diabetes in order to investigate the precise role each variable plays.
Conclusions
Bariatric surgery has opened the door to the exciting field of metabolic surgery. There are still many clinical, physiological, and hormonal aspects to be investigated, but the data of the studies in literature and the results of our experience provide insights and hypotheses that should be developed in future randomized clinical trials.
Footnotes
Author Disclosure Statement
None of the authors involved in the manuscript preparation has any conflicts of interest, either financial or moral, toward the manuscript itself. None of the authors received support in the form of grants, equipment, and/or pharmaceutical items. All authors contributed equally to this work and read and approved the final manuscript.