
Abstract
Background:
Children with type 1 diabetes (T1D) spend 4–7 h/day in school with very little supervision of their diabetes management. Therefore, families have become more dependent on technology, such as use of real-time continuous glucose monitoring (RT-CGM), to provide increased supervision of their diabetes management. We sought to assess the impact of RT-CGM use in the classroom/school environment.
Subjects and Methods:
Children with T1D using RT-CGM, their parents, and teachers completed a questionnaire about RT-CGM in the classroom/school environment.
Results:
The RT-CGM was tolerated well in the classroom/school environment. Seventy percent of parents, 75% of students, and 51% of teachers found RT-CGM useful in the classroom/school environment. The students found the device to be more disruptive than did their parents and teachers. However, all three groups agreed that RT-CGM increased their comfort with diabetes management at school.
Conclusions:
Our study suggests that RT-CGM is useful and not disruptive in the classroom/school environment. The development of education materials for teachers could further increase its acceptance in the classroom/school environment.
Introduction
With these challenges in mind, the introduction of new insulin delivery systems as well as real-time continuous glucose monitoring (RT-CGM) systems may have facilitated optimal management of T1D. 4 However, the complexity of care has increased in both the family and school environment because of the burden of managing additional equipment, which is worn on the body at all times, and from the resultant issues that result from improper use or management. In these situations, the benefits of RT-CGM come from the more extensive BG information it provides, useful in diabetes management decisions. Also, the ability for RT-CGM to alarm when a child's BG level has reached a predetermined threshold can ease some of the common fears shared among teachers. A survey found that a major worry of teachers “was the possibility that children [with diabetes] could go into a coma at school or that they [the teachers] would not be able to recognize a hypoglycemic episode.” 3 Although severe hypoglycemia is feared by teachers, mild or moderate hypoglycemia occurs more often. RT-CGM could help reduce anxiety about unexpected hypoglycemia; however, the alarms on the device have the potential to disrupt classrooms or distract the child with diabetes from learning. The goal of this pilot study was to assess the relative benefits and disadvantages of RT-CGM in the classroom setting.
Subjects and Methods
All school-age children between 5 and 17 years with T1D using a continuous glucose monitoring system (Minimed Paradigm® continuous glucose monitor [Medtronic, Inc., Northridge, CA], Dexcom® Seven Plus [Dexcom, Inc., San Diego, CA], or Freestyle® Navigator continuous glucose monitoring system [Abbott Diabetes Care, Abbott Park, IL]) were asked to participate. The child and parent each completed an ad hoc family questionnaire. Three children who could not read were asked to listen to the questions and answer them orally. The questions were asked using age-appropriate language, and the answers were recorded by research staff. The parents and the rest of the children separately completed his or her own written questionnaire (see Supplementary Fig. S1; Supplementary Data are available online at
All data were collected and managed using REDCap (Research Electronic Data Capture) (CTSA# UL1 RR025744) electronic data capture tools hosted at Stanford University. REDCap is a secure, Web-based application (
Results
Twenty of the 21 families agreed to participate in the study (Table 1). All students were enrolled in grades kindergarten–12 (four elementary, seven middle school, and nine high school). Six students attended private school. Eleven of the students had more than one teacher (up to seven teachers). Forty of the 65 (62%) of the teachers agreed to participate and completed the surveys. Thirteen of the teachers taught the student for 4 h a day or longer. Almost 80% of the teachers had been teaching for more than 5 years (20% had been teaching for more than 20 years), and six of the classrooms had greater than 28 students. Ten (50%) of the students had a registered school nurse or health aide available at school outside of the classroom. However, the nurse or health aide was present at the school for less than 1 h/day and provided care to all students requiring medication administration in the school. Half of the elementary school-age children (n=2) verified insulin doses with the nurse or health aide, but the rest of the students did not seek assistance from a nurse or health aide.
Data are number or mean±SD as indicated.
HbA1c, glycosylated hemoglobin; MDI, multiple daily insulin injections; RT-CGM, real-time continuous glucose monitoring.
Seventy percent of parents, 88% of students, and 78% of teachers reported that they were moderately to very comfortable with technology (computers, smartphones, digital cameras, text messaging, etc.) in general, whereas 100% of parents, 65% of students, and 38% of teachers were at the same comfort levels with diabetes management. Either a parent (n=6) or a student (n=9) provided training on the RT-CGM device to their teachers (n=23). This training session lasted up to an hour.
The RT-CGM was well tolerated in the classroom/school environment. Seventy percent of parents, 75% of students, and 51% of teachers found RT-CGM useful in the classroom/school environment.
Further analysis revealed that students ranked their devices as significantly more disruptive than did teachers (H 1=14.04, P=0.000).
Although the student users found the RT-CGM to be the more disruptive than did parents or teachers (Fig. 1A), all three groups reported that the RT-CGM increased their comfort of managing diabetes in the classroom (Fig. 1B). Those teachers who found the RT-CGM disruptive in the classroom had the student with diabetes for more than 4 h/day. There were significant differences in subjective ratings of comfort change in the classroom among all three groups (H 2=7.50, P=0.024). Additional analyses showed there were no statistical differences in reported comfort between students and teachers (P=0.318) and between students and parents (P=0.102). However, parents rated the classroom comfort change as significantly higher than teachers (H 1=7.47, P=0.006). It is interesting that the total number of reported BG checks during school (seven or eight times a day) did not change with the use of the RT-CGM device. The average number of the actual of BG checks a day, downloaded from the meters, was 7.4±3.6 (range, three to 15) times per day.
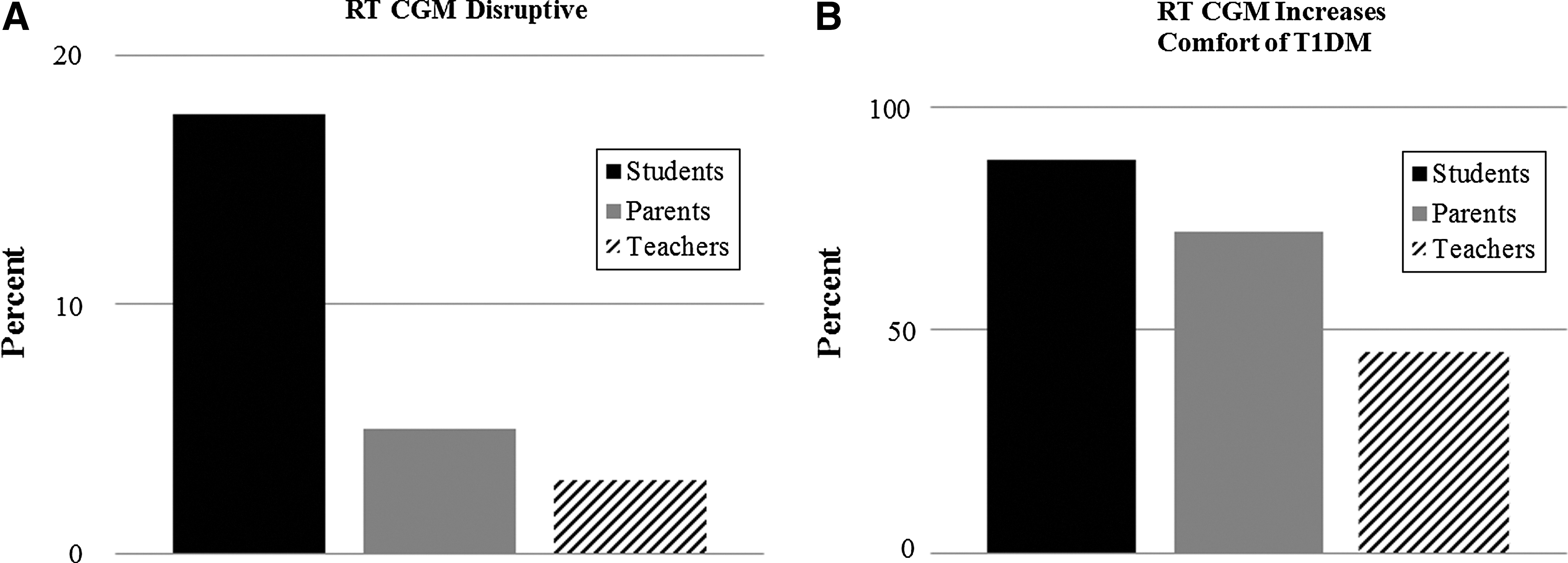
Students with type 1 diabetes (T1DM), parents, and teachers were surveyed regarding usage of real-time continuous glucose monitoring (RT CGM) devices in the classroom/school environment.
Discussion
Because children with diabetes may spend up to 8 h/day at school, they need to rely on the school personnel, particularly the teachers, to manage their diabetes. Because of recent advances in technology, more students are using continuous subcutaneous insulin infusion (or pump) therapy and RT-CGM in the classroom/school environment. In this study, we report that teachers did not find RT-CGM to be disruptive but rather useful to have in the classroom/school environment and that the presence of RT-CGM increased the comfort level of diabetes management in the classroom by the students, parents, and teachers.
U.S. federal law protects the rights of children with diabetes, 6 and diabetes is considered a disability. 7,8 Therefore, the needs of a student with diabetes should be provided during school with little disruption to the school's and the child's routine. 9,10 However, despite this, current budgets do not allow for nurses to be available in many of the schools where there are children with diabetes, and, instead, teachers and other school personnel such as school administrators, teacher's aides, health aides, secretaries, coaches, bus drivers, etc., 11,12 often provide supervision of the diabetes management. 2 Families and schools have adapted by having children learn to give their own insulin injections, use an insulin pump, and, more recently, use RT-CGM. Often goals of RT-CGM use are (1) to reduce glycemic variability, (2) to avoid or decrease the number of moderate or severe hypoglycemic episodes, and (3) to increase awareness of BG values during the time spent in school without direct supervision.
As in any study, this pilot study had limitations, which included the small sample size and potential selection bias as the families who participated in the study were very motivated in their children's diabetes management as seen by 6 out of 7 days a week of RT-CGM use. The results of the study may also not be generalizable because, although continuous subcutaneous insulin infusion and RT-CGM are available for diabetes management, only a small percentage of our patients use both devices consistently. Also, we did not ask what percentage of time the students used the vibrate feature rather than the alarm feature on the RT-CGM, and a greater percentage of time on alarm mode would potentially result in more classroom disruption. In addition, because the amount of time the RT-CGM device was placed on vibrate mode is unknown, it is possible the teachers did not find RT-CGM to be disruptive because they could not hear the vibrations but were felt only by the students.
In our study, diabetes healthcare professionals instructed the families on the use of the RT-CGM device, and the families trained the teachers for less than 1 h. The teachers who received training were receptive to the use of RT-CGM in their classrooms and appreciated the training. In fact, the teachers commented in the teachers' questionnaire that they were willing to learn how to use the devices and wanted a quick reference guide. However, as some teachers did not receive any training, they possibly would not be able to identify the source of the alarm(s) in the classroom. Our limited resources prevented us from uniformly training each teacher on RT-CGM use before they completed the questionnaires. Also, we were unable to survey the classmates of our participants if the use of RT-CGM was disruptive in the school/classroom environment as the participants' privacy needed to be respected and protected in the school.
Conclusions
One of the frontiers of diabetes research is in the development of closed-loop algorithms for diabetes management. Thus the use of RT-CGM in the classroom/school environment will increase. As the management of diabetes becomes more dependent on technology, the support and knowledge of school personnel need to broaden. Therefore, we propose that device companies, healthcare professionals, children and adults with diabetes, and teachers form committees to work towards the goal of developing diabetes education materials for school personnel. This should include a user-friendly or quick reference guide for RT-CGM use in school. Knowledgeable, trained personnel are essential if children are to avoid the immediate risks of low BG levels and to achieve the metabolic control required to decrease risks for later development of diabetes complications. 2
In summary, this small pilot study suggests that use of RT-CGM in the school environment is not disruptive. The development of educational materials for teachers could further increase its acceptance in the classroom/school environment.
Footnotes
Acknowledgments
We would like to thank all the families for their participation and time.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.