
Abstract
Chronic medical conditions such as type 2 diabetes may alter the body's normal response to heat. Evidence suggests that the local heat loss response of skin blood flow (SkBF) is affected by diabetes-related impairments in both endothelium-dependent and non–endothelium-dependent mechanisms, resulting in lower elevations in SkBF in response to a heat or pharmacological stimulus. Thermoregulatory sweating may also be diminished by type 2 diabetes, impairing the body's ability to transfer heat from its core to the environment. Diabetes-associated co-morbidities and the medications (particularly those affecting fluid balance) required to treat these conditions may exacerbate the risk of heat-related illness by decreasing SkBF and sweating further. Unfortunately, the majority of studies measure local heat loss responses in the hands and feet and lack measures of core temperature. Therefore, the impact of these impairments on whole-body heat loss remains unknown. This review addresses heat-related vulnerability in individuals with type 2 diabetes by examining the literature related to heat loss responses in this population. Type 2 diabetes, its associated co-morbidities, and the medications required in their treatment may cause dehydration, lower SkBF, and reduced sweating, which could consequently impair thermoregulation. This effect is most evident in individuals with poor blood glucose control. Although type 2 diabetes can be associated with impairments in SkBF and sweating, more physically active individuals requiring fewer medications and having good blood glucose control may be able to tolerate heat as well as those of similar age and body composition.
Introduction
Epidemiological data from extreme heat events demonstrate that individuals with type 2 diabetes are more likely to die or be hospitalized during a period of severe heat compared with those without diabetes. 1 These findings indicate that heat tolerance may be reduced in individuals with type 2 diabetes, but the extent that this condition affects the body's ability to dissipate heat remains unclear. If increased heat-related morbidity and mortality are due to diabetes-related impairments in thermoregulatory function, then individuals with type 2 diabetes may also have a greater risk of heat-related injury or illness while performing physical activity under moderate conditions.
The World Health Organization estimates that of the 346 million people worldwide thought to have diabetes, 2 90% have type 2 diabetes. Where the environment is concerned, the frequency and severity of extreme heat events are likely to increase in coming years. 3 Thus, determining the magnitude of heat-related risk in potentially vulnerable individuals, such as those with type 2 diabetes, is essential.
In healthy individuals heat is dissipated from the body to the environment via the local heat loss mechanisms of skin blood flow (SkBF) and sweating (Fig. 1). For a comprehensive overview of these mechanisms, the reader is referred to the review by Kenny and Journeay. 4 Although only one study to date has examined whole-body heat loss in individuals with type 2 diabetes, 5 several studies have examined the local heat loss responses of SkBF 6 –15 and sweating. 16 –19 Many of these studies found impairments in local heat loss responses in individuals with type 2 diabetes compared with matched controls. Unfortunately, many studies measure responses of the hands and/or feet, in order to assess neuropathy, a complication associated with long-standing or poorly controlled diabetes, rather than heat loss capacity. Meaningful measures of change in core temperature are absent, and the impact of impairments in local heat loss responses on whole-body heat loss capacity in this population remains unclear. This review examines the current state of knowledge surrounding impairments in heat loss responses in individuals with type 2 diabetes and identifies existing knowledge gaps.
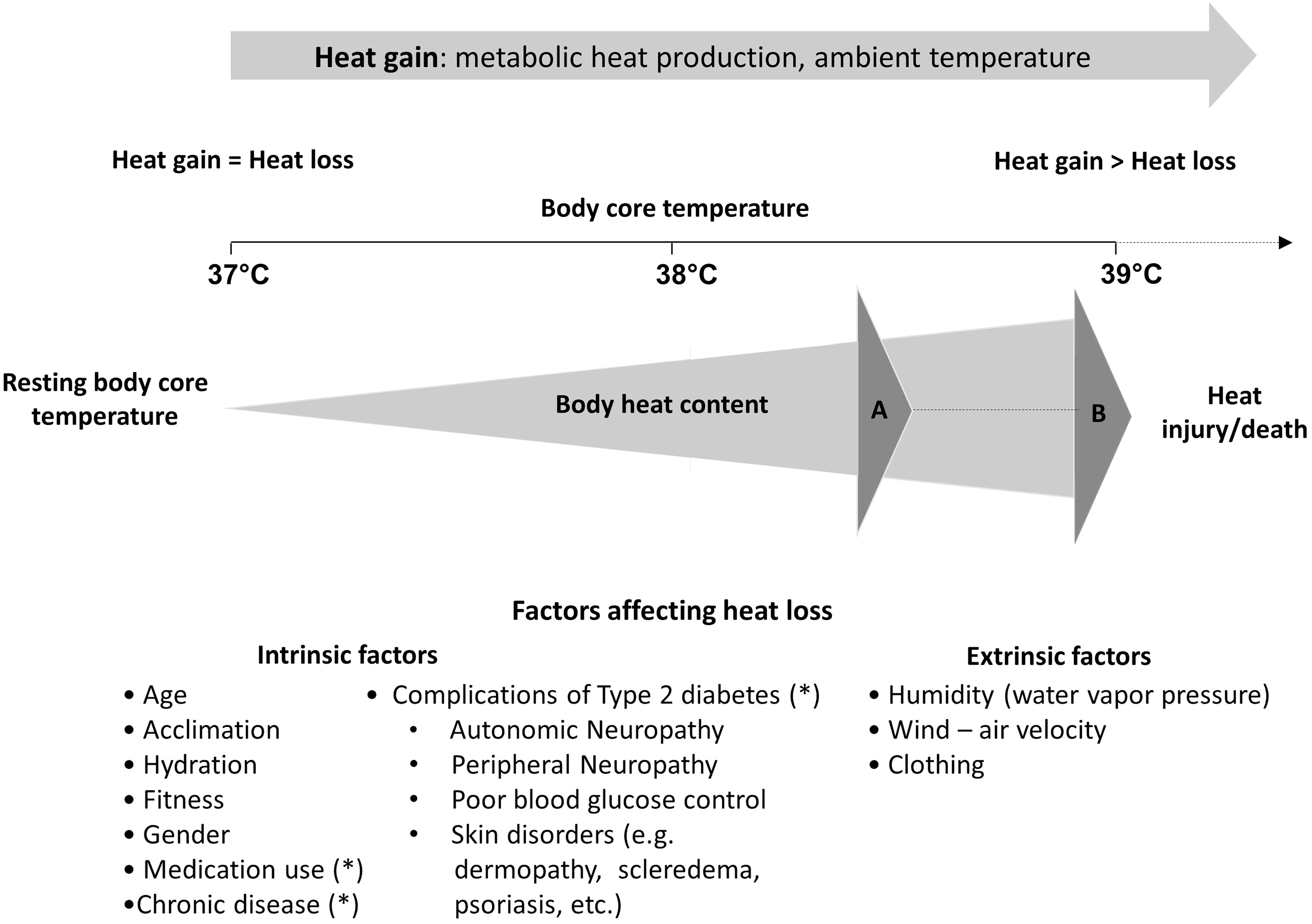
Schematic of the human heat stress response. Heat gain, from increases in metabolic heat production and/or ambient temperature, causes an elevation body core temperature, activating the heat loss responses of skin blood flow and sweating. The requirement for heat loss rises with increasing heat load. If the rate of heat gain exceeds that of heat loss, body heat content increases, resulting in a rise in body core temperature. Extrinsic factors (ambient humidity, clothing, etc.) can restrict heat loss, causing a greater increase in body heat content (depicted as a shift from point A to point B). Intrinsic factors such as age, gender, fitness, acclimation, etc., as well as those associated with complications of type 2 diabetes can affect the body's heat dissipation capacity and subsequently the amount of heat stored during a thermal challenge. The local heat loss responses of skin blood flow and sweating may be diminished by type 2 diabetes, its associated co-morbidities, and commonly prescribed medications. The impacts of these impairments on whole-body heat loss have not been fully elucidated (*).
Type 2 Diabetes and Thermoregulation
Skin blood flow
Type 2 diabetes is associated with serious vascular complications, including nephropathy, retinopathy, and cardiovascular disease. Within the skin microvasculature, diabetes-associated endothelial dysfunction decreases the bioavailability of nitric oxide (NO), a key player in vasodilation. As a result, individuals with type 2 diabetes may have lower SkBF responses to pharmacological stimuli, 7,10,13 the application of local heat, 6,11,15,16 or whole-body heating 9,14,16 compared with age-matched controls. The effect of these reductions on thermoregulation in this population is unclear, as most studies measure SkBF on the hands and/or feet. Measures of core temperature are lacking, thereby restricting their usefulness in predicting whole-body heat dissipation and the level of thermal strain.
Individuals with diabetes exhibit decreased vasodilator responsiveness to pharmacological stimuli. 7,13 Williams et al. 7 compared forearm blood flow responses to methacholine chloride and sodium nitroprusside (SNP) in individuals with diabetes versus age- and sex-matched controls to assess vasodilation in response to endothelial-independent NO. The researchers observed an attenuated response to both methacholine and SNP in the type 2 diabetes group compared with controls indicating impaired vasodilation to both endogenous and direct-acting exogenous NO donors. 7
Impairments in both endothelium-dependent and endothelium-independent vasodilation have also been examined in forearm cutaneous vasculature in resting individuals with type 2 diabetes. 10,13 Schmiedel et al. 13 found lower SkBF responses to local heating (44°C), acetylcholine (ACh) (assessing endothelium-dependent vasodilation), and SNP (assessing endothelium-independent vasodilation) in individuals with type 2 diabetes (n=29) compared with controls without diabetes (n=10). Similarly, Beer et al. 10 found impaired responses to local heat (41°C), SNP, and ACh in a group of type 2 diabetes patients (n=54) compared with age- and sex-matched controls without diabetes (n=38). In both studies, individuals with diabetes complications (who also tended to have a longer duration of diabetes) exhibited greater impairments in SkBF responses than those without.
Sokolnicki et al.
8
compared forearm SkBF responses of individuals with type 2 diabetes and age-matched controls using a microdialysis infusion of N
G-nitro-
Being physically active may help in maintaining vascular responses to heat exposure in individuals with type 2 diabetes. 20,21 Colberg et al. 20 found that resting SkBF on the dorsal foot was lower in sedentary type 2 diabetes participants than in regularly exercising diabetes participants. In fact, resting SkBF in the type 2 diabetes exercisers was similar to that of exercising controls without diabetes. 20 Maximal SkBF elicited by local heating (44°C), however, was still lower in exercisers with diabetes compared with exercisers without diabetes, although comparable to sedentary controls without diabetes. 20 When the same measurement was taken after a bout of cycle ergometer exercise to volitional fatigue, differences between exercisers without diabetes and those with diabetes were eliminated, 21 indicating that chronic physical activity positively affects cutaneous circulation in individuals with type 2 diabetes. Blood glucose control also had a significant effect, with hemoglobin A1c (HbA1c) and fasting glucose levels being inversely correlated with blood flow during heating. 20,21
Training duration and exercise intensity may also affect endothelial function. Colberg et al. 22 found that maximum skin perfusion on the foot dorsum (elicited by local heating to 44°C) was lower in individuals with type 2 diabetes prior to 10 weeks of moderate (50–65% heart rate reserve) aerobic training three times a week, compared with controls without diabetes. Post-training, differences between groups were no longer significant, in spite of neither group experiencing a significant perfusion increase. 22 The authors attributed the lack of significant change to the training period being too short and/or the exercise intensity being too low. These observations are consistent with studies examining different exercise modalities. Two months of moderate resistance exercise (three sets of eight to 12 repetitions, two to three times weekly) did not increase maximal skin perfusion elicited by local heating on the dorsum of the foot 23 or in response to infusion of SNP in the forearm. 24 Cohen et al., 24 however, found that vascular reactivity to SNP in the forearm was significantly improved after 14 months of resistance training in individuals with type 2 diabetes. Vascular responsiveness after 14 months of training also showed a strong inverse correlation with baseline HbA1c, indicating the importance of blood glucose control. Where exercise intensity is concerned, da Silva et al. 25 found that high-intensity training (80% of maximum heart rate, four times weekly for 6 weeks) improved endothelium-dependent vasodilation in patients with metabolic syndrome and type 2 diabetes, whereas a comparable period of low-intensity exercise (55% of maximum heart rate) did not.
Although poor blood glucose control is associated with impaired SkBF, the early damage caused by chronic hyperglycemia may be partially reversed with improvements in blood glucose control. 26 The maximum SkBF response to local heating (44°C) on the foot dorsum of type 2 diabetes patients was examined at the time of diagnosis (mean HbA1c, 9.4%) as well as 3 months (mean HbA1c, 6.8%) and a year (mean HbA1c, 6.1%) thereafter where blood glucose control had improved substantially. After a year of good control, the impaired SkBF responses (compared with controls without diabetes) measured at baseline and 3 months were significantly improved, with the percentage increase in maximal SkBF correlating with the percentage decrease in HbA1c. 26 How these changes affect whole-body heat loss, however, remains unclear.
Sweating
The limited sweating-related studies in type 2 diabetes primarily examined sudomotor function to assess autonomic neuropathy, rather than thermoregulatory function. Although one study examining forearm sweating in response to ACh iontophoresis found similar mean sweat volume and number of activated sweat glands in individuals with type 2 diabetes and controls without diabetes, 18 most studies found impaired sweat responses in this population. 16,17,19 For example, in response to an electrical stimulus on the quadriceps, the percentage increase in sweating was lower in resting participants with type 2 diabetes compared with individuals without diabetes. 19 In addition, responses to repeated stimulation were lower in those with diabetes compared with those without. 19 The effect of attenuated responses to repeated stimuli on whole-body heat loss and core temperature regulation requires assessment.
Studies examining whole-body heat exposure in individuals with type 2 diabetes have also found attenuated sweat responses. 16,17 Fealey et al. 17 found that 94% of type 1 and type 2 diabetes patients with signs and symptoms of neuropathy displayed some form of sweating abnormality when subjected to a passive heat exposure (ambient air temperature of 44°C, approximately 45% relative humidity). Abnormalities ranged from decreased sweating in the lower limbs to complete anhydrosis. Similarly, regarding sweating responses, type 2 diabetes participants resting in a supine position in a hot environment (39°C) had lower sweat rates on the head, chest, leg, and arm compared with controls without diabetes. 16 Lower sweat rates were also found on the arms and legs of type 2 diabetes participants compared with controls during and after a 40% maximum voluntary handgrip contraction to exhaustion performed under warm ambient conditions (32°C). Sweating on the forehead, however, was higher for diabetes subjects compared with controls, demonstrating that sweating decrements occur at a non-uniform rate over the entire body. How regional alterations in sudomotor function affect the body's ability to dissipate heat remains unclear. 16
Type 2 diabetes-related impairments in sudomotor function may be linked to changes in sweat gland peripheral properties, especially where diabetes has been long-standing and/or poorly controlled 17,27 or in the presence of autonomic neuropathy. 27 Skin biopsies of individuals with diabetic neuropathy revealed that type 2 diabetes patients had a lower sweat gland innervation index (area of nerve fibers normalized to the area of sweat glands) than age- and sex-matched controls. 27,28 Also, whereas sweat gland secretory coils were present in controls, the periglandular nerve terminals were reduced or absent in individuals with type 2 diabetes. 27,28 Lower sweat gland innervation correlated inversely with levels of HbA1c and fasting plasma glucose, indicating that sweating impairments in type 2 diabetes may be directly related to poor blood glucose control. 27 In one study, sweat gland innervation was also related to the level of autonomic neuropathy, evidenced by reduced heart rate variability. 27 It should also be noted that sweat gland output may be reduced as a result of decreased NO bioavailability in type 2 diabetes: nonselective NO synthase inhibition has been shown to decrease thermoregulatory sweating during exercise in a warm environment 29 and delay increases in pharmacologically induced maximal sweating 30 in individuals without diabetes.
Although impaired sweat production, especially in the presence of poor blood glucose control, seems common with type 2 diabetes, none of the above studies included core temperature measures. One study using whole-body calorimetry (a device accurately measuring the heat emitted by the human body) to assess how older adults with type 2 diabetes respond to increasing levels of heat stress during physical activity found that whole-body heat loss was significantly suppressed throughout a 60-min moderate intensity exercise bout in participants with diabetes. 5 This resulted in a greater amount of heat stored, and therefore a higher level of thermal strain, in the individuals with type 2 diabetes (360 kJ) relative to their matched (for age, body composition, and fitness) healthy controls (265 kJ). By the end of the 60-min recovery, the individuals with type 2 diabetes lost only 21% of the total heat gained during exercise, whereas their counterparts without diabetes lost in excess of 55%. 5 These findings demonstrate that older adults with type 2 diabetes may be at greater risk of developing a heat-related injury during exercise in the heat.
Complications and Co-Morbidities
Diabetic neuropathy
Long-standing diabetes, especially if it is poorly controlled, can cause widespread damage to peripheral and autonomic nerves and small vessels. Unmyelinated fibers are often prone to damage, resulting in a decreased ability to sense a heat stimulus, 31 –33 which could potentially delay appropriate adaptive behavior in a hot environment. Many people with type 2 diabetes have the metabolic syndrome, and sensory neuropathies have also been associated with the metabolic syndrome prior to the development of frank diabetes. 34 The severity of autonomic neuropathy in individuals without diabetes but with metabolic syndrome is inversely correlated with high-density lipoprotein-cholesterol rather than HbA1c. 34 Although damage to sensory nerves will impair the ability to sense thermal changes, it remains unclear whether the inability to sense warming of the skin affects efferent signals of cutaneous vasodilation and/or sweating during exposure to a warm environment.
Autonomic neuropathy could be of greater concern than peripheral neuropathy in this population, as it can occur relatively early after the development of type 2 diabetes, with clinical manifestations including macrovascular, microvascular, gastrointestinal, genitourinary, and sudomotor dysfunction. 35 As mentioned above, skin biopsies of individuals with diabetic neuropathy revealed that type 2 diabetes patients had a lower sweat gland innervation index than age- and sex-matched controls. 27,28 Neuropathy-related impairments in sudomotor function may result in partial (generally lower body) or complete anhydrosis in individuals with type 2 diabetes. 17 SkBF responses to local heat exposure are also decreased in individuals with diabetic neuropathy 36 with greater impact also being seen in the lower body. 37 Taken together with the increased cardiovascular risks, individuals with autonomic neuropathy may be at particularly high risk of heat-related morbidity and mortality.
Obesity
About 80% of people with diabetes in the United States are overweight or obese. 38 Even in the absence of diabetes, obesity alone is a risk for heat-related injury and illness. Fatal heat stroke occurs 3.5 times more often in overweight or obese adults compared with normal-weight individuals. 39 The body surface area to mass ratio is smaller in obese individuals, decreasing the ability to exchange heat with the environment per unit of body mass. 40 The specific heat capacity of adipose tissue is also about half of that of fat-free mass, producing greater increases in body temperature in obese individuals compared with lean individuals faced with a similar heat load. 41 The importance of both of these factors in temperature regulation was shown by Havenith and van Middendorp 42 : a multiple regression analysis of factors influencing heat storage and changes in body core temperature during exercise in the heat found that percentage body fat and body surface area to mass ratio had the largest influence on the variance in these measures.
Most studies examining heat tolerance in obese individuals involve performing mild to moderate exercise in environments of varying temperature and humidity. 40 –48 Although two studies showed similar heart rate and core temperature responses to cycling exercise in the heat between obese and lean individuals, 47,48 participants in these studies were performing non–weight-bearing activity at a relative intensity (percentage maximal oxygen uptake [%VO2max]) where obese individuals had a significantly lower fitness level, and therefore a lower work output. Conversely, when obese and lean participants performed weight-bearing exercise at a controlled rate (i.e., treadmill walking at a specific speed) in a hot and/or humid environment, obese individuals had elevated heart rates, 40,41,43,46 lower evaporative heat loss, 43,46 greater core temperature increases, 40,46 and more body heat storage 40,46 compared with age-matched, lean controls. This is mostly explained by the greater metabolic heat production required for a heavier individual to perform the same physical work. For example, Haymes et al. 46 found that obese participants expended 40% more energy than lean participants during standardized treadmill walking (4.8 km/h, 5% grade). With a lower surface area to mass ratio, the additional metabolic heat produced by obese individuals is less easily dissipated, thereby increasing the risk of heat-related injury.
Obesity may also impair an individual's ability to adapt to repeated heat exposures. Dougherty et al. 44,45 exposed both lean and obese boys (9–12 years old) to repeated bouts of treadmill walking at 30% VO2max on separate days at an ambient temperature of 38°C and 50% relative humidity. Although core temperatures were lower in both groups with successive exercise sessions, adaptation occurred more slowly in the obese boys. In addition, where exercise heart rates decreased with successive sessions in the lean participants, no changes were seen in obese participants. 44 In a study attempting to determine critical environmental limits for exercise in heat-acclimated boys, obese participants had a lower maximal evaporative capacity and failed to maintain heat balance at a lower temperature and/or relative humidity than their lean counterparts. 45
It is difficult to assess the additional impairment in local heat loss responses conferred by the presence of type 2 diabetes in obese individuals. Most studies reviewed in the present article matched their participants with diabetes with age- and sex-matched controls, but not for body mass index or body composition. 7,10 –12,16,18,19,28 Where studies matched for body mass index and percentage body fat, 6,8,9,13 –15,21 all but one found impairments in SkBF in the participants with type 2 diabetes compared with their controls. 6,8,9,13,14,21 As mentioned above, only one study has examined whole-body dry and evaporative heat loss in individuals with diabetes and well-matched controls, with impaired whole-body heat loss being found during moderate-intensity exercise in those with type 2 diabetes. 5 Future studies should carefully match subjects for body surface area and percentage body fat, as well as for age and sex (Table 1).
Dyslipidemia
Dyslipidemia, a common co-morbidity in type 2 diabetes, is associated with several vascular complications, including nephropathy, retinopathy, neuropathy, and coronary artery disease. 52 How this condition impacts sweating has not been examined. Meanwhile, SkBF is often measured to assess microvascular responsiveness in individuals with dyslipidemia. Although statins, commonly prescribed for dyslipidemia, are known to improve microvascular responses, 53 it is unclear whether it is the lipid lowering per se or the pleitropic effects of the statins (also influencing inflammation, oxidative stress, and endothelial-derived NO production) that have the greatest effect on microvascular function. A study by Settergren et al. 54 used laser Doppler flowmetry to examine the effects of lowering blood lipid levels, either by use of simvastatin or a combination of very low-dose simvastatin and ezetimide, on postocclusive and heat-induced hyperemic foot and forearm SkBF responses. Similar responses were found in both groups after 6 weeks of treatment, indicating that lipid lowering is the most important factor in improved microvascular response. Two other studies, however, failed to produce improvements in microvascular function with lipid-lowering therapy, 55,56 although this may be due to poor diabetes control in one study 55 and a lack of initial vascular complications in the other. 56 The effect of dyslipidemia on whole-body heat loss by means of impaired SkBF responses requires further scrutiny.
Hypertension
Hypertension is associated with structural abnormalities of the microvasculature including vessel wall thickening with concurrent reduction of the lumen diameter and a decrease in the number of parallel-connected capillaries and arterioles. 57 These changes could limit increases in SkBF during heat exposure, thereby decreasing a hypertensive individual's ability to maintain a safe core temperature. In addition, several medications used in the treatment of hypertension increase the risk of dehydration (discussed below) and subsequently impair thermoregulation.
Impaired local heat loss mechanisms in hypertensive individuals are most evident where greater heat loss is required. Two studies involving passive whole-body heating where core temperature increases did not exceed 0.5°C measured similar SkBF responses in hypertensive individuals and normotensive controls. 58,59 Meanwhile, Carberry et al. 60 found that resting maximal forearm SkBF response to local heating (44°C) was reduced in hypertensive individuals compared with age- and weight-matched normotensive controls. Similarly, during moderate-intensity exercise (40% VO2max) in the heat (38°C), Kenney et al. 61,62 found attenuated increases in forearm blood flow in hypertensive participants compared with normotensive controls. The authors surmised that structural alterations in the vasculature (thickened media and/or an increase in smooth muscle layers) would diminish vasodilation in response to increased thermal stimuli.
Changes in the vasculature associated with diabetes, however, may supersede those of hypertension where thermoregulation is concerned. Jaap et al. 63 compared the maximal SkBF response to local heating (44°C) on the foot dorsum in three different groups: hypertensive individuals with type 2 diabetes, normotensive individuals with type 2 diabetes, and a normotensive group without diabetes. Groups were matched for age and sex, and the diabetes groups were matched for disease duration. SkBF responses to local heating were comparable between the hypertensive and normotensive diabetes participants; however, both groups with diabetes had an attenuated response compared with individuals without diabetes. 63 The impact of these impairments on whole-body heat loss is currently unknown.
Cardiovascular disease
Adults with diabetes have heart disease death rates two to four times higher than those without diabetes. 64 Individuals with cardiac dysfunction have greater difficulty increasing cardiac output to maintain elevated SkBF when faced with prolonged heat exposure. Evidence of this can be found in the epidemiological data: during the heat event that struck Europe in 2003, mortality rates were 30% greater among individuals with heart disease than during a comparison period. 65
There is currently no evidence indicating that cardiovascular disease interferes with sweat production, but it may impair SkBF responses to a heat stimulus. Cui et al. 66 found that although sweat responses were preserved, skin vasodilator responses during both local (42°C) and whole-body heating were significantly lower in heart failure patients compared with healthy matched controls. Similarly, Green et al. 67 found lower SkBF responses to whole-body heating in patients with chronic heart failure compared with healthy matched controls. It is unknown whether the presence of diabetes will exacerbate impairments in SkBF found in cardiovascular disease patients, but a synergistic effect of the two conditions is possible. For example, a 6-h heat exposure (ambient air temperature of 41°C, 15–25% relative humidity) increased blood viscosity, elevated red blood cell counts, and increased platelet counts in healthy individuals. 68 These alterations to the blood will increase the risk of coagulation, and subsequently cerebral and coronary thromboses, 68 in relatively healthy individuals, let alone those having several cardiovascular risk factors. Where individuals with type 2 diabetes are at a higher risk of dehydration due to hyperglycemia and/or medication usage, the risk of a cardiovascular event may be compounded. Further research is warranted to determine how these conditions interact to affect whole-body heat loss and the resulting heat injury risks during prolonged heat exposure.
Skin disorders
Studies have found an association between skin disorders such as infections, psoriasis, eczema, scleredema, and dermopathy and type 2 diabetes, with greater prevalence being found in those with worse metabolic control. 69 Disorders can often result in areas of thickened skin, reduced skin elasticity, and reduced blood flow. 70 If large enough areas of skin are affected, such legions could theoretically impact the body's ability to cool itself through effective SkBF and sweating. There are, however, no studies to date examining the effect of diabetes-related skin disorders on thermoregulation.
Additional Considerations
Physical characteristics
Physical activity levels, 71 age, 72 and sex 73 also affect the ability to increase sweating and SkBF during heat stress. More frequently active people have greater SkBF 71 and sweat 74 responses compared with less active age- and sex-matched individuals. In addition to the declines in strength and aerobic capacity, 75 aging is associated with decrements in sweating and SkBF 72,76,77 during heat exposure. The thirst response (the body's primary mechanism of signaling the need for fluid) is also blunted with age, leading to progressive dehydration during heat exposure 78 or physical activity. 79 In addition, when requirements for heat loss reach their highest levels, females have less ability to sweat than males. 73 With the exception of the study by Colberg et al. 20 described above, studies to date have failed to assess the impact of physical characteristics such as age, sex, and physical fitness on local heat responses in individuals with type 2 diabetes. A great deal more research is necessary to understand the spectrum of heat-related vulnerability in this population.
Hydration
During prolonged heat exposure, sweating can lead to significant water loss, especially where physical activity has been performed in the heat, subsequently affecting the body's ability to sweat and increase SkBF during heat stress. Lower levels of hydration can increase the core temperature at which the onset threshold for skin vasodilation occurs and can decrease sweat rates for a given core temperature. 80,81 Decreased blood and plasma volume, and the concomitant increase in plasma osmolality accompanying dehydration, have been shown to independently attenuate SkBF and sweating responses during heat stress. 80,82 –84 Where cardiac output must substantially increase to meet SkBF demands (up to 8 L/min during heat stress), 85 dehydration adds considerable strain on the cardiovascular system and increases the risk of cardiovascular events.
Good blood glucose control is essential to ensuring hydration in individuals with diabetes. 86 If blood glucose levels exceed the renal threshold for glucose reabsorption, the resulting osmotic diuresis leads to substantial dehydration if adequate replacement fluids are not ingested, thereby impairing SkBF and sweating. It should also be noted that medications affecting renal function (i.e., diuretics and angiotensin-converting enzyme inhibitors) can adversely affect fluid balance.
Medication
Several medications that are commonly prescribed to individuals with type 2 diabetes may have an impact on thermoregulation. These include salicylates (for treatment of mild to moderate pain and for heart disease risk reduction), diuretics, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers (prescribed for hypertension or to reduce cardiovascular and renal risks). Other medications not specific to the treatment of diabetes-related ailments that also interfere with sweating and SkBF include anticholinergic agents (treatment of gastrointestinal, genitourinary, or respiratory disorders), antidepressants, antiglaucoma agents, bladder stimulants, antiepileptics, antihistamines, antipsychotics, and antiemetics. Side effects of the above agents involve increased heat production in the body, prevention of heat loss to the environment by inhibition of local heat loss mechanisms (usually sweating), or both. Where intensive treatment with multiple medications has been shown to decrease the risk of type 2 diabetes-related complications such as cardiovascular disease, nephropathy, and retinopathy, 87 it is uncertain what effect multifactorial pharmacological treatment will have on heat-dissipation capacity in these individuals. The combination of certain medications with high environmental temperatures and/or increased metabolic heat production from physical activity can increase heat injury risks substantially. For a more comprehensive review of the effects of medication on thermoregulation, the reader is referred to the report by Health Canada. 88
Knowledge Gaps
Key knowledge gaps related to heat loss responses in individuals with type 2 diabetes are summarized in Table 1.
Conclusions
Impairments in local heat loss responses are evident with type 2 diabetes, which may subsequently affect whole-body heat loss. Data to date are insufficient to determine the extent of the risk associated with heat exposure in this population. More studies examining these responses concurrently with changes in core temperature are necessary. In addition, there is a lack of research examining the effects of physical activity either in the heat or during uncompensable heat stress (due to high humidity or protective clothing restricting sweat evaporation). As the incidence and prevalence of type 2 diabetes increase, it is essential to ascertain the full level of risk associated with heat stress for this potentially vulnerable population.
Footnotes
Acknowledgments
J.E.Y. was supported by a University of Ottawa postdoctoral fellowship (funds held by G.P.K.). J.M.S. was supported by a MITACS Accelerate Doctoral Internship. G.P.K. was supported by a University of Ottawa Research Chair Award. R.J.S. was supported by a Health Senior Scholar award from the Alberta Heritage Foundation for Medical Research.
Author Disclosure Statement
No competing financial interests exist.