
Abstract
Background:
This article describes our experience with inpatient hybrid closed-loop control (HCLC) initiated shortly after the diagnosis of type 1 diabetes in a randomized trial designed to assess the effectiveness of inpatient HCLC followed by outpatient sensor-augmented pump (SAP) therapy on the preservation of β-cell function.
Subjects and Methods:
Forty-eight individuals with newly diagnosed type 1 diabetes and positive pancreatic autoantibodies (7.8–37.7 years old) received inpatient HCLC therapy for up to 93 h, initiated within 7 days of diagnosis.
Results:
On initiation of HCLC, mean glucose concentration was 240±100 mg/dL. During the first day of HCLC, median of the participant's mean glucose concentrations fell rapidly to 146 mg/dL, a level of control that was sustained on Days 2 and 3 (138 mg/dL and 139 mg/dL, respectively). By Day 3, the median percentage of glucose values >250 and <60 mg/dL was <1%. During the first 2 weeks of SAP treatment at home, the median participant mean glucose level was 126 mg/dL (interquartile range, 117, 137 mg/dL), and the median percentage of values between 71 and 180 mg/dL was 85% (interquartile range, 80%, 90%).
Conclusions:
Inpatient HCLC followed by outpatient SAP therapy can provide a safe and effective means to rapidly reverse glucose toxicity and establish near-normal glycemic control in patients with newly diagnosed type 1 diabetes.
Introduction
New technologies offer additional tools to improve glycemic control. In the inpatient research setting there are experimental closed-loop systems. In the outpatient setting there are commercially available insulin pumps and continuous glucose monitors (CGMs), which, when used together, have proven to be effective in lowering hemoglobin A1c levels in several randomized clinical trials. 5,6 However, pumps and CGM devices generally are not prescribed at the time of diagnosis of type 1 diabetes, and there is little information on the effect of optimizing glycemic control as soon as possible after diagnosis.
To test the hypothesis that intensive glycemic control from the onset of type 1 diabetes will preserve endogenous insulin production, we conducted a randomized trial to evaluate inpatient hybrid closed-loop control (HCLC) followed by outpatient use of SAP therapy versus usual care in individuals enrolled within 7 days of diagnosis. The primary outcome is C-peptide levels measured with a mixed meal tolerance test (MMTT) at 12 months (these results will be reported in a separate article). Herein we describe our experience with the study participants in the intensive therapy group who were managed with inpatient HCLC and the subsequent first 2 weeks of outpatient SAP therapy.
Research Design and Methods
The study was conducted at five clinical centers. Participants were enrolled between May 2009 and October 2011. The protocol was approved by each local institutional review board. Written informed consent was obtained from participants ≥18 years of age and from parents/guardians of younger participants from whom written assent was obtained. Major eligibility criteria included ages from 6 to <46 years and diagnosis of type 1 diabetes with initiation of insulin therapy within the prior 7 days (with Day 0 considered the day that insulin was started). This report includes the results from the 48 participants who had at least one positive anti–islet cell autoantibody to insulin, glutamic acid decarboxylase, insulinoma antigen, zinc transporter-8, or an islet-cell antibody and were randomly assigned to the intervention group that received inpatient HCLC followed by outpatient SAP therapy. Two participants assigned to the intensive group did not have positive autoantibodies and as prespecified were not included in the analyses.
When possible, a blinded Guardian® CGM device (Medtronic MiniMed, Inc., Northridge, CA) was worn between enrollment and the hospital admission for initiation of HCLC. Prior to initiation of HCLC therapy, a 90-min MMTT was performed. At the start of the admission for HCLC therapy, an intravenous line was placed in the arm for blood draws to monitor glucose levels and for administration of glucose or insulin if needed for treatment of hypoglycemic or hyperglycemic events, respectively.
Inpatient HCLC used the Medtronic MiniMed external physiological insulin delivery (ePID) system, 7,8 consisting of a Medtronic MiniMed subcutaneous glucose sensor and insulin infusion pump communicating wirelessly every minute with a bedside computer running Control Tool software (developed by Medtronic MiniMed) using the ePID algorithm. The goal was to complete a minimum of 72 h to a maximum of 96 h of HCLC. The ePID algorithm used every 1-min sensor readings to determine insulin administration. The protocol required that a physician or nurse practitioner trained in the care of persons with diabetes be available at all times during HCLC therapy. Study personnel calculated premeal boluses of insulin to assist in controlling postprandial hyperglycemia in association with the automated closed-loop control, thus the nomenclature “hybrid” closed-loop control. Sensor calibration was performed using the Control Tool software. Study personnel recalibrated the sensor whenever repeated sensor values deviated from the reference glucose concentrations by at least 15%.
The proportional-integral-derivative algorithm used in these studies has been previously described 7 –9 but was modified to incorporate insulin feedback (IFB). 10 –12 IFB uses a three-state subcutaneous insulin absorption model that captures the subcutaneous, plasma, and effective insulin concentrations and modifies the insulin dose to adjust for active insulin. The proportional-integral-derivative algorithm with IFB was initialized by entering the participant's weight and total daily insulin dose. The glucose set point was 110–120 mg/dL. Up to 20 min prior to each meal and snack, carbohydrates were counted, and a premeal bolus was given to provide insulin coverage for 75–80% of the meal based on the participant's current carbohydrate-to-insulin ratio, which was initially determined by dividing the total daily insulin dose into 450 13 and then adjusted as needed based on postprandial glucose levels. There were no dietary restrictions, with participants choosing both the timing and the content of all meals and snacks. Participants were permitted short walks of up to 25 min between blood draws, during which time the closed-loop system and insulin delivery were suspended and then resumed upon return to the hospital room. During HCLC, blood glucose measurements were obtained every 30 min using a reference glucose analyzer (YSI [YSI Inc. Life Sciences, Yellow Springs, OH], GlucoScout [International Biomedical, Austin, TX], HemoCue® [HemoCue, Inc., Cypress, CA], or i-STAT® [Abbott Point of Care Inc., Princeton, NJ]) and every 15 min when glucose values were <70 mg/dL. Standard hypoglycemia treatment of approximately 15 g of carbohydrates was given for glucose values <70 mg/dL. For two consecutive glucose values >300 mg/dL, a serum ketone level was checked. Unless otherwise specified, reported glucose results refer to blood glucose measurements and not CGM measurements.
During the hospital admission, extensive teaching was provided for use of the insulin pump and CGM for diabetes management upon discharge. At discharge, participants were provided with all necessary supplies for the insulin pump and the CGM (including glucometers and testing strips) and were instructed to use the CGM daily.
Descriptive statistics are reported as mean±SD values or median with interquartile range (IQR) depending on the distribution of a variable.
Results
The 48 participants in the intensive treatment group had a mean (±SD) age of 12.7±4.7 years (range, 7.8–37.7 years; 46 of the 48 total patients were <18 years old), 35% were female, and 91% were non-Hispanic white, 2% were African-American, 4% were Hispanic, and 2% were more than one race. Three centers began recruitment from the onset of the study, enrolling 12, 14, and 11 subjects, respectively; two additional centers were added 2 years later, and they enrolled six and five subjects, respectively. At the time of diagnosis, mean initial glucose level was 501±193 mg/dL, mean hemoglobin A1c was 11.7±2.3% (105±25 mmol/mol), and mean body mass index percentile (excluding two participants >20 years of age) was 43±31%. Fourteen (29%) presented in diabetic ketoacidosis based on Diabetes Control and Complications Trial criteria. Intravenous insulin was received by 11 (79%) of the 14 with diabetic ketoacidosis and by none of the 34 without diabetic ketoacidosis; the mean initial glucose levels were 542±169 mg/dL and 483±202 mg/dL, respectively. Subcutaneous insulin was given on an outpatient basis prior to initiation of HCLC therapy.
Enrollment occurred 0–6 days after the initiation of insulin therapy (median, 3 days; IQR, 2, 4 days). For the 39 participants using a blinded CGM prior to the hospital admission, median participant mean glucose level by CGM was 179 mg/dL (IQR, 147, 231 mg/dL) during the day prior to initiating HCLC.
HCLC was initiated a mean of 5.7±1.2 days after diagnosis and was used for a median of 71.3 h (IQR, 70.3, 72.1 h; range, 29.9–93.2 h) by the 48 participants, with 45 of the 48 (94%) participants completing at least 68 h of HCLC. Three subjects stopped HCLC early (after 30, 42, and 56 h, respectively) because of problems with the intravenous line, which was required for use of HCLC.
On initiation of HCLC, mean glucose concentration was 240±100 mg/dL, which in some cases was measured shortly after the MMTT. Two participants had measurable blood ketones (0.3 and 0.5 mmol/L, respectively) within the first 12 h. During the first 6 h of HCLC, median participant mean glucose concentration was 170 mg/dL (IQR, 135, 208), with a median of 57% of values between 71 and 180 mg/dL (IQR, 35%, 81%). There was a progressive improvement in glycemic control over the rest of the first day, plateauing with a median among participants of about 80% of glucose values between 71 and 180 mg/dL (IQR, 75%, 90%) (Table 1 and Figs. 1 and 2). The median mean glucose level was lower, and the median percentage of values between 71 and 180 mg/dL was higher overnight (12 midnight to 7 a.m.) than during the daytime on all 3 days of HCLC (Table 2). The frequency of glucose levels ≤70 mg/dL was low (1.0% of glucose values) during HCLC with 13%, 17%, and 9% of participants having at least one value below 60 mg/dL on Days 1, 2, and 3, respectively. The percentage of readings ≤50 mg/dL was 0.1% on Day 1, 0% on Day 2, and 0% on Day 3, and for all days the Low Blood Glucose Index was 0.5. The percentages of glucose values 71–180 mg/dL according to clinical site are shown in Supplementary Table S1 (Supplementary Data are available online at
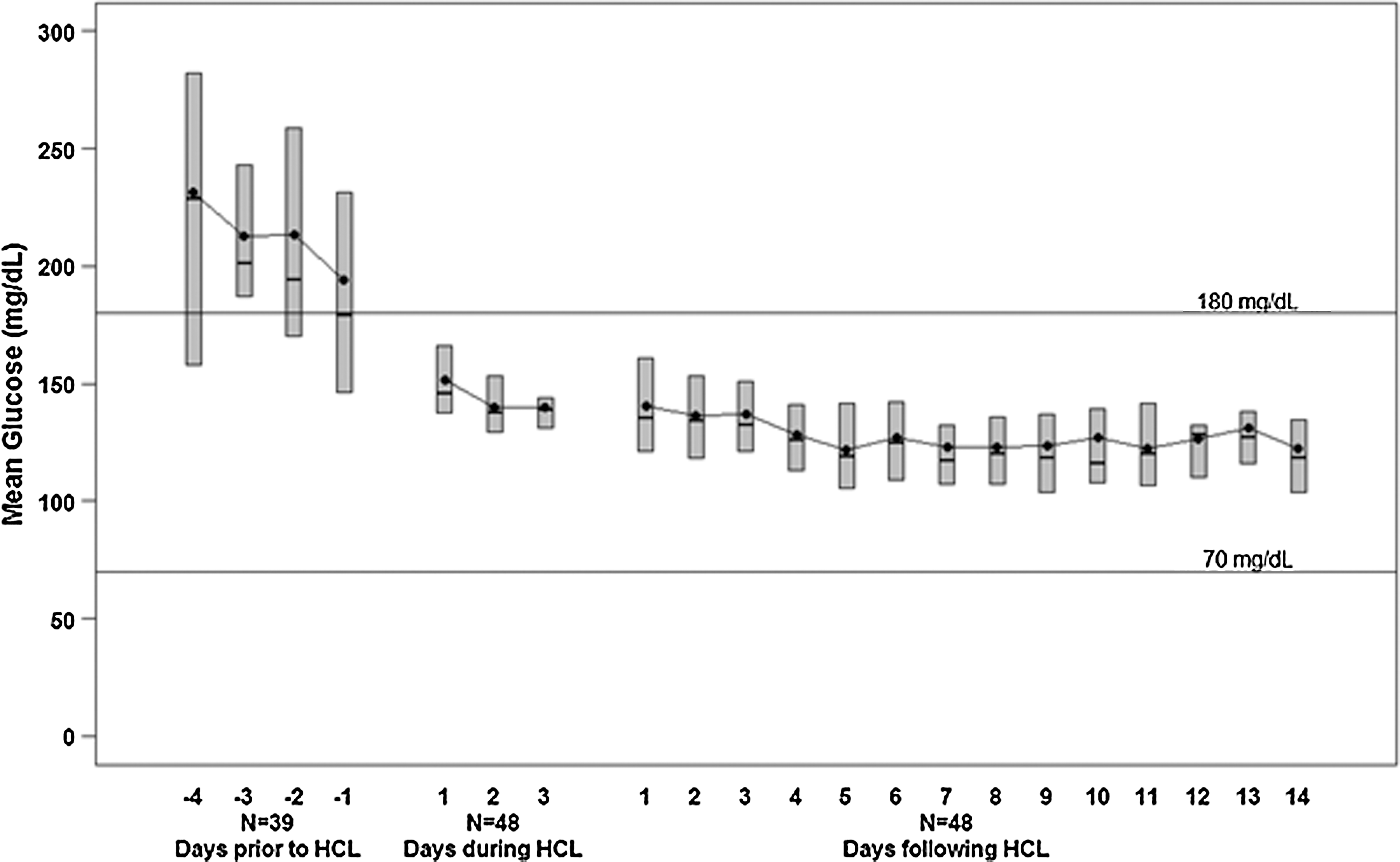
Participant mean glucose values from a continuous glucose monitor worn prior to admission, during hybrid closed-loop (HCL) control, and 2 weeks following discharge (n=48). The bottom and top of each box denote the 25th and 75th percentiles, respectively, the line inside the box denotes the median, and the dot is the mean.
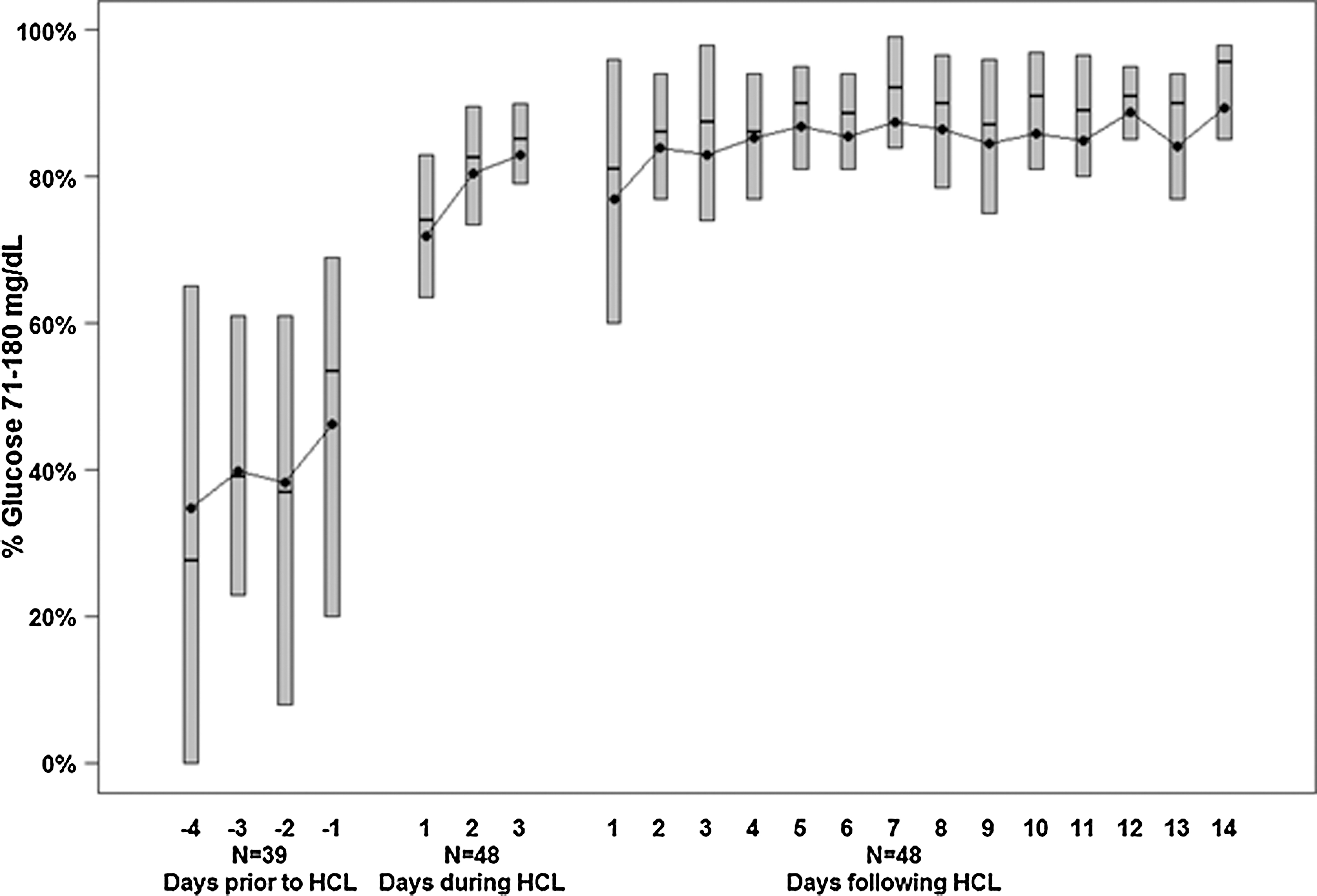
Distribution of percentage of continuous glucose monitor glucose values 71–180 mg/dL from a continuous glucose monitor worn prior to admission, during hybrid closed-loop (HCL) control, and 2 weeks following discharge (n=48). The bottom and top of each box denote the 25th and 75th percentiles, respectively, the line inside the box denotes the median, and the dot is the mean.
Data are median (25th, 75th percentiles) unless stated otherwise.
Pooled across participants.
Data are medians (25th, 75th percentiles) unless stated otherwise.
Pooled across participants.
Median (IQR) carbohydrate intake during the 3 days of HCLC was 72 (53, 88), 72 (59, 87), and 73 (59, 90) g for breakfast, lunch, and dinner, respectively, representing 1.7 (1.1, 2.3), 1.8 (1.3, 2.3), and 1.7 (1.3, 2.3) g/kg, respectively. There was an additional 51 (30, 88), 56 (33, 87), and 47 (27, 101) g for snacks on the 3 days. The median (IQR) total daily insulin dose was 1.2 (0.8, 1.5), 1.2 (0.8, 1.5), and 1.2 (0.9, 1.5) units/kg/day, and the percentage given by the ePID-IFB controller was 61%, 63%, and 58% on Days 1, 2, and 3, respectively, with the remainder given as manual premeal priming doses.
There were no episodes of diabetic ketoacidosis or severe hypoglycemia. One subject had an anaphylactic reaction (presumed peanut allergy) following his first dinner and received intravenous steroids, which resulted in increased insulin doses (1.8 units/kg/day) during the first 24 h.
In the 2 weeks following discharge from the hospital, during which time the participants were using SAP therapy at home, glycemic control improved further with a median participant mean sensor glucose level of 126 mg/dL (IQR, 117, 137) and a median percentage of values between 71 and 180 mg/dL of 85% (IQR, 80%, 90%) (Fig. 2). Median total daily insulin dose was 0.7 (IQR, 0.6, 1.0) units/kg/day.
Discussion
This study found that inpatient HCLC safely initiated soon after the diagnosis of type 1 diabetes resulted in a rapid decrease in blood glucose levels within 24 h of initiation. This was sustained during the subsequent 2 weeks of outpatient use of SAP therapy. While using HCLC, about 80% of glucose levels were in the target range of 71–180 mg/dL, with minimal hypoglycemia. The ePID controller in this setting was able to maintain excellent nocturnal glycemic control and good but not perfect daytime control, as has been demonstrated in prior inpatient studies of individuals with long-standing type 1 diabetes. 7,8
In order to simulate normal food intake at home during inpatient HCLC, the participants freely selected the content of meals from the standard hospital menus. Because the majority of participants were adolescent boys, it is not surprising that total carbohydrate intake approached a mean of 2 g/kg/day. To reduce the anticipated postmeal hyperglycemia with HCLC, a physician-determined premeal bolus was given, which has been previously shown by Weinzimer et al. 8 to significantly improve postprandial hyperglycemia during closed-loop control. It is of interest that despite the ePID-IFB controller not accounting for these premeal boluses, there was minimal postprandial hypoglycemia. All overnight insulin delivery was determined by the ePID controller.
It has previously been demonstrated that the metabolic decompensation at the time of diagnosis of type 1 diabetes is accompanied by a significant reduction in insulin sensitivity. 14 Such insulin resistance was reflected in the median total daily insulin doses that exceed 1 unit/kg/day during initial inpatient HCLC. Conversely, the benefits of early intensive management using HCLC to acutely reverse glucotoxicity and improve insulin sensitivity are reflected in the rapid fall in daily insulin requirements to 0.7 unit/kg/day during the first 2 weeks of outpatient SAP therapy.
The use of closed-loop control in this study differs from the closed-loop control previously used by Shah et al. 1 in that they began closed-loop control within 24–48 h from the onset of diabetes and continued inpatient closed-loop control for 14 days. They used the BioStator, which delivered intravenous insulin, whereas we delivered subcutaneous insulin, and their controller used blood glucose levels, whereas our controller was driven by subcutaneous glucose levels. Their target glucose levels were 63–80 mg/dL, and following meals glucose levels peaked between 110 to 150 mg/dL but returned within 1 h to the target glucose range.
In this study, we have shown that inpatient HCLC initiated shortly after the diagnosis of type 1 diabetes can be safe and effective in rapidly restoring near-normal glycemic control. It remains to be determined whether an “all-in” approach to diabetes technology that combines HCLC at the time of diagnosis with subsequent SAP therapy will result in a greater preservation of insulin production than the level that can be achieved with the current standards of care of newly diagnosed patients with type 1 diabetes.
Footnotes
Acknowledgments
We greatly appreciate the families who made a decision to participate in this study, a decision that was made within days of diagnosis, at a time of significant stress. This research was supported by National Institutes of Health/Eunice Kennedy Shriver National Institute of Child Health and Human Development grants HD41890-10, HD41906-10, and HD41908-10 for the Diabetes Research in Children Network (DirecNet) Study Group and grants U01DK085509, U01DK06104211, 5U01DK085466-05, U01DK085505-02, and 5U01DK085465-04 for the Type 1 Diabetes TrialNet Study Group. Type 1 Diabetes TrialNet is a clinical trials network funded by the National Institutes of Health through the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institute of Allergy and Infectious Diseases, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Center for Research Resources, the Juvenile Diabetes Research Foundation International, and the American Diabetes Association. This research was supported in part by the following: for the Barbara Davis Center for Childhood Diabetes, University of Colorado School of Medicine, CTRC grant 1UL1 RR025780; for the Division of Pediatric Endocrinology and Diabetes, Stanford University, Clinical and Translational Science Award SUL1 RR025744 for the Stanford Center for Clinical and Translational Education and Research (Spectrum) from the National Center for Research Resources, National Institutes of Health; for the Department of Pediatrics, Yale University School of Medicine, grant UL1 RR024139 from the National Center of Research Resources, a component of the National Institutes of Health, and the National Institutes of Health Roadmap for Medical Research (information on Re-engineering the Clinical Research Enterprise can be obtained from
Author Disclosure Statement
Among the members of the Writing Committee, B.A.B. received payment from Sanofi-Aventis, Glysense, and Roche for serving on Medical Advisory Boards, consulted for BD, received payment for a lecture (symposium at the European Association for the Study of Diabetes meeting) from DexCom, received payment from Medtronic for serving on the DSMB for STAR3 trial, and received institutional payment from Medtronic for other Principal Investigator–initiated studies and sponsored research. C.K. has consulted with Diabetes Technology Management (DTM). S.A.W. consulted for Johnson & Johnson and BD and received payment for lectures including service on speaker bureaus from Eli Lilly, stock/stock options from Insuline Medical, and in-kind support for research from Medtronic. L.D. reports payment to her institution from Medtronic for an investigator-initiated grant. A.A.B. consults for the American Humane Society on projects regarding animal-assisted therapy for pediatric patients and has received payment for lectures from Pfizer. M.C. is employed by Medtronic and has received payment for stock/stock options from Medtronic. R.S. serves on medical advisory board for Medtronic. No competing financial interests exist for R.W.B., K.J.R. and P.C.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.