
Abstract
Type 1 diabetes (T1D) results from the autoimmune destruction of pancreatic β-cells, and as such it should respond to immunotherapy. George Eisenbarth gave many significant contributions to this field. He has been involved at some level in most immunotherapy trials during the past three decades. He was among the pioneers who attempted immunotherapy approaches in patients with recent-onset T1D. In the early 1980s he began studying relatives of those with the disease, leading to the concept that T1D was a chronic autoimmune disease, in which islet autoimmune responses would silently destroy β-cells and cause progressive impairment of insulin secretion, years to months before a diagnosis was made. Consequently, he was one of the first to attempt immune intervention in people at high risk of T1D. Throughout his career he developed autoantibody assays and predictive models (which included metabolic testing and later genetics) to identify individuals at risk of T1D. He provided seminal intellectual contributions and critical tools for prevention trials. His focus on insulin as a critical autoantigen led to multiple prevention trials, including the Diabetes Prevention Trial-Type 1 (DPT-1), which studied both parenteral and oral insulin. In the DPT-1 Oral Insulin Trial, a cohort with higher levels of insulin autoantibodies was identified that appeared to have delayed disease progression. Type 1 Diabetes TrialNet is conducting a new trial to verify or refute this observation. Moreover, George identified and tested in the mouse small molecules that block or modulate presentation of a key insulin peptide and in turn prevent the activation of insulin-specific T-lymphocytes. Thus, we believe his greatest contribution is yet to come, as in the near future we should see this most recent work translate into clinical trials.
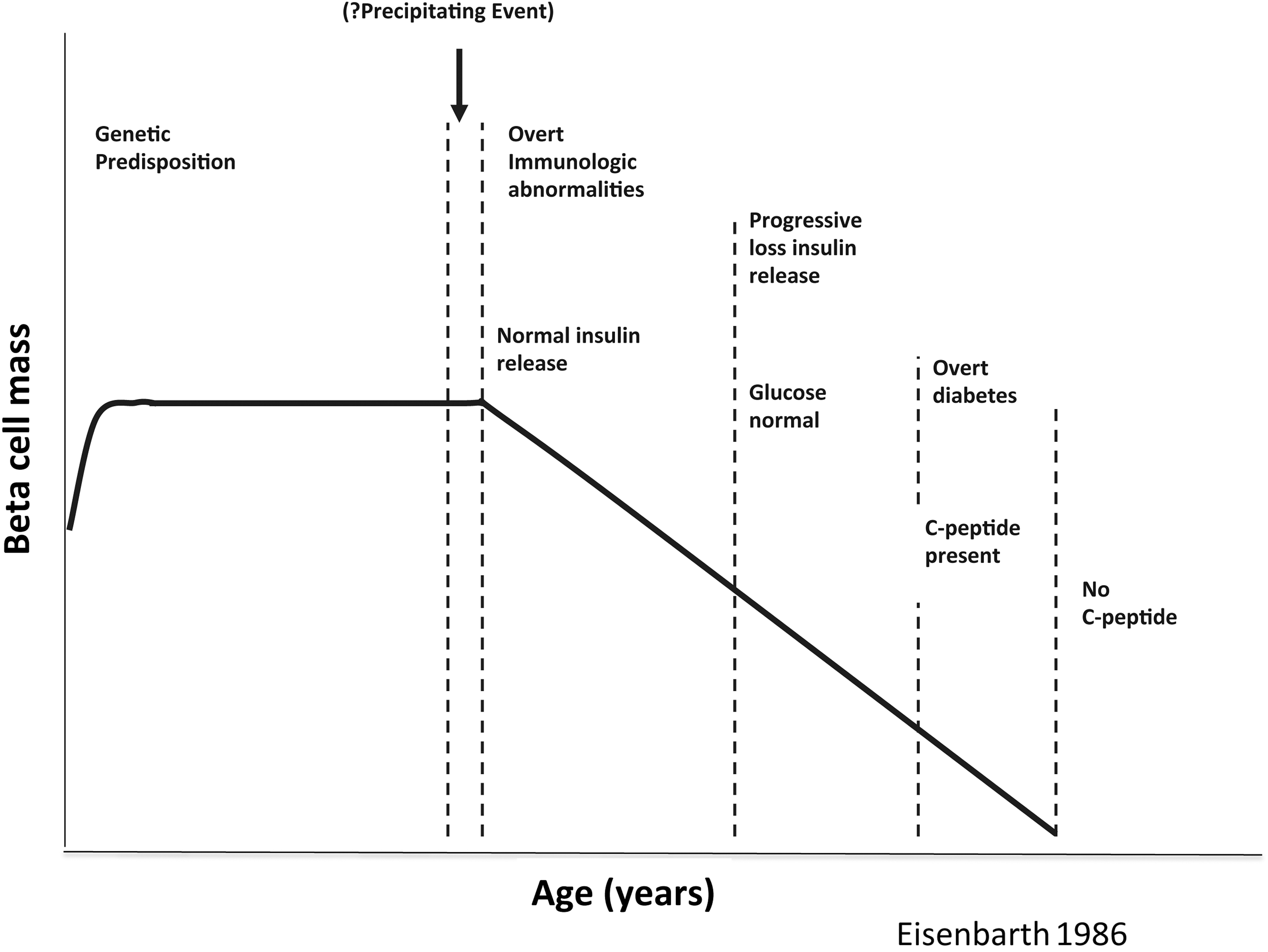
Scheme depicting a model of the stages of type 1 diabetes as a chronic progressive autoimmune disease, eventuating in “total” diabetes with absent β-cell function (i.e., no C-peptide production). The x-axis is without a specific time scale as the rate of progress of the disease may be quite variable. Modified from Eisenbarth. 3 (Source: Eisenbarth GS: Autoimmune beta cell insufficiency - diabetes mellitus Type 1. Triangle 1984;23:111–124.)

Updated scheme depicting a model of the stages of type 1 diabetes as a chronic progressive autoimmune disease, with variation in the rate of β-cell destruction during progression to hyperglycemia. Again, the x-axis is without a specific time scale as the rate of progress of the disease may be quite variable. Modified from Eisenbarth. 5 Reprinted from Endocrine Practice, Vol 18, Eisenbarth GS: Prevention of type 1A diabetes mellitus, pp 745–749, 2012, with permission from the American Association of Clinical Endocrinologists.
An immune-mediated disease should be beneficially impacted by immune modulation therapy. Thus, beginning in the 1970s, there were attempts to treat T1D with various immune interventions. 7,8 Moreover, if the immune process indeed begins a long time prior to clinical disease onset, immune intervention should be able to interdict the disease process and prevent or delay clinical disease. 9,10 George Eisenbarth was involved in several early studies, designed to alter the course of the disease, in both recent-onset T1D and for prevention of T1D.
One early study, in recent-onset T1D, evaluated short courses of immunotherapy and included nine patients treated with prednisone, six treated with the anti-thymocyte globulin ATGAM plus prednisone, and three treated with placebo. 11 Both therapies altered T cells, and ATGAM patients had lower hemoglobin A1c (HbA1c) levels on lower insulin doses with two subjects able to discontinue insulin therapy for 8 months. Unfortunately, thrombocytopenia precluded further study of ATGAM.
In recent-onset diabetes, George was also involved in a study with an anti-CD5 immunotoxin in which an anti-CD5 monoclonal antibody was linked to the ricin A-chain. 12 This seemed to preserve β-cell function, as evidenced by C-peptide, but was never advanced to a full-scale trial. This was the first study in T1D using a monoclonal antibody, and it would foretell many studies that would subsequently evaluate several different monoclonal antibodies in T1D.
Prevention trials were really the thing that motivated George the most, however. He was involved in several early pilot trials. One demonstrated that in two individuals prednisone could increase first-phase insulin secretion rate (FPIR) during an intravenous glucose tolerance test (IVGTT). 13 In another small pilot study of only three subjects, oral nicotinamide failed to slow progression of disease, 14 an observation that would presage the results of the large-scale multicenter European Nicotinamide Diabetes Intervention Trial (ENDIT) that involved 549 subjects at risk of developing T1D, which also did not show a benefit from nicotinamide. 15
Building on the success in two large randomized controlled clinical trials of cyclosporine in improving outcomes in recent-onset T1D, 16,17 it was logical to attempt using cyclosporine to prevent T1D. Therefore, in an early study in relatives at risk of T1D, six subjects treated with cyclosporine were compared with nine historical controls. 18 The controls had developed T1D within 12 months (5.9±1.1 months), whereas four of the six cyclosporine-treated subjects developed T1D after 5, 24, 24, and 47 months, respectively, and at the time of the report two cyclosporine-treated subjects had not yet developed T1D 47 and 57 months after entry into the study. Two of the subjects showed correction of their low FPIR levels.
Another early attempt at interrupting the T1D disease process in relatives at risk of the disease was to use insulin therapy itself. 19 In a pilot study at the Joslin Diabetes Center, Boston, MA, George and his colleagues offered a program of insulin prophylaxis to 12 individuals at risk of T1D. Seven declined, and five accepted the treatment, which consisted of low-dose subcutaneous insulin therapy together with a 5-day course of intravenous insulin every 9 months. The subjects who declined were followed as a contemporary comparison group, and historical controls were analyzed as well. A life table analysis suggested a dramatic benefit, as after 3 years, only one of the five treated subjects had developed T1D, in comparison with all seven of those who had declined the therapy. 19
Around the same time, Anette-G. Ziegler (a former Fellow of George's) and her colleagues in Munich, Germany, initiated a similar study of prophylactic insulin use. 20 In their randomized trial, ultimately seven subjects at risk of T1D received prophylactic insulin, and seven were randomized to the control group. Life table analysis showed that clinical onset of T1D was delayed in the insulin-treated group compared with the control subjects (means±SEM diabetes-free survival, 5.0±0.9 years vs. 2.3±0.7 years; P<0.03). 21
The hypothesis that insulin therapy for relatives at risk of T1D was fully tested in the Diabetes Prevention Trial-Type 1 (DPT-1), a multicenter randomized clinical trial conducted through the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). 22 George was a member of the DPT-1 Steering Committee and was a member of the small group that designed the study. That design, in large part, was based on the Joslin pilot study 19 and on concepts that George had articulated 23 and required that subjects be positive for ICA and have either reduced FPIR during an IVGTT (as standardized 24 ) or an abnormal glucose level but not one indicating diabetes during an oral glucose tolerance test (OGTT) and not have the protective HLA DQB1*0602. 25 Based on these criteria, subjects enrolled in the DPT-1 parenteral insulin trial had a projected 5-year risk of T1D of at least 50%. The study screened 84,228 relatives of people with T1D, with 3.7% being positive for ICA on initial screening. The study randomized 339 subjects—the experimental group to receive twice-daily injections of human ultralente insulin (total daily dose of 0.25 units/kg), plus annual 4-day infusions of intravenous insulin, whereas the control group had “close observation.” 22 Both groups underwent an OGTT every 6 months. After a median follow-up of 3.7 years, the cumulative incidence of T1D was similar in the two groups (relative risk in the intervention group compared with the observation group, 0.96), a disappointing result. It should be noted that the observed 5-year risk of T1D was 65%, thus validating the prediction criteria, which, as noted, were based in large part on George's concepts.
A subsequent Belgian study, which used prandial insulin rather than basal insulin, in relatives at risk of T1D also failed to show a beneficial effect on delaying progression to T1D. 26
Meanwhile, it was recognized that while screening for the DPT-1 parenteral insulin trial, which required enrollees have a projected 5-year risk of T1D of at least 50%, there would be identified a cohort of individuals still at modestly high risk of T1D, but not a 50% projected risk. An important study that George had conducted together with Howard Weiner and colleagues had demonstrated in non-obese diabetic (NOD) mice (an animal model of T1D) that oral insulin could prevent the development of T1D. 27 Even more powerful was the finding that splenocytes from NOD mice that had received oral insulin prevented the adoptive transfer of T1D in mice that concomitantly received splenocytes from mice with diabetes. 27
These observations led to the DPT-1 Steering Committee electing to conduct a second concomitant study evaluating the use of oral insulin in relatives with a projected 5-year risk of T1D of 25–50%. 28 That risk was based on subjects screening positive for ICA, also having insulin autoantibodies (IAA) and having “intact” FPIR on IVGTT and normal OGTT. The study screened a total of 103,391 relatives of people with T1D. Ultimately, 372 met the inclusion criteria and were randomized to receive oral insulin (7.5 mg/day) or matched placebo. Both groups underwent an OGTT every 6 months. After a median follow-up of 4.3 years, the cumulative incidence of T1D was similar in the two groups (hazard ratio in the oral insulin group compared with the placebo group, 0.76; P=0.189), another disappointing result. 28 Yet, a post hoc hypothesis-generating analysis showed that there was a suggestion of a beneficial effect in enrollees who had on two occasions at baseline IAA levels of at least 80 nU/mL. In such individuals (n=263 of the 372 subjects randomized), the annualized diabetes rate was 6.2% with oral insulin and 10.4% with placebo (hazard ratio in the oral insulin group compared with the placebo group, 0.566; P=0.015). That subgroup was analyzed because it represented the initial IAA level required for enrollment. Unfortunately, enrollment rate was slower than projected, so the unfortunate decision (in hindsight) was made to reduce the level of IAA required for enrollment to 39 nU/mL (3 SD above the mean of controls without diabetes, whereas 80 nU/mL was 5 SD above the mean of controls without diabetes).
Treatment was stopped in the DPT-1 oral insulin trial in 2003. In an effort to determine long-term outcome of the study, a telephone survey was conducted in 2009 to ascertain whether T1D had been diagnosed, and, if not, an OGTT, HbA1c, and autoantibody levels were obtained on subjects who agreed to participate. 29 Overall, the oral insulin treatment effect in individuals with confirmed IAA of at least 80 nU/mL seemed to be sustained; yet, once treatment was stopped, the rate of developing T1D in the previous oral insulin group increased to that in the placebo group.
Given the results seen in the post hoc analysis of the DPT-1 oral insulin trial, Type 1 Diabetes TrialNet, 30 an NIDDK-sponsored clinical trials consortium that basically succeeded DPT-1, has elected to conduct another oral insulin prevention trial, with the expectation of replicating the outcome seen in the post hoc analysis of the DPT-1 oral insulin trial. 30,31
Meanwhile, George continued to promote the concept that antigen-based therapies would be the safest and most specific way of dealing with immune modulation in T1D. 32 Based on studies in NOD mice, 33 he championed the concept that an altered peptide ligand, specifically a modification of the amino acid sequence of the peptides spanning positions 9–23 on the B-chain of insulin (B9–23), might modify the course of the disease. A study with a B9–23 altered peptide ligand was undertaken in recent-onset T1D but failed to show an effect on residual β-cell function. 34
Another antigen-based approach is the use of a plasmid DNA vaccine encoding mouse pro-insulin. 35 George participated in a mouse study suggesting the potential utility of this approach in T1D. 36 Yet, the 1-year results of a clinical trial with a plasmid DNA vaccine encoding human pro-insulin in patients with T1D gave mixed results. 37 The authors of the abstract asserted that there might be some associated preservation of β-cell function, but the data were not completely convincing. 37 However, the plasmid DNA vaccine was well tolerated.
Unfortunately, several other antigen-based therapies also have not met with success. Nasal insulin was studied in the Type 1 Diabetes Prediction and Prevention Study (DIPP), which was conducted in Finland. 38 The DIPP group screened 116,720 newborns from the general population for high-risk HLA-DQB1 susceptibility alleles, followed up 10,577 prospectively, and, after at least two diabetes autoantibodies were confirmed, eventually enrolled 224 who were randomized to receive either intranasal insulin (1 unit/kg of body weight daily) or placebo. The rate of progression to T1D was the same in the nasal insulin group and the placebo group. 38
Intranasal insulin has also been studied in Australia. The first trial established safety of the approach. 39 A subsequent trial showed potential immunologic effect by demonstrating that the interferon-γ response of blood T-cells to proinsulin was suppressed after nasal insulin. 40 A full-scale trial is now being recruited. 41
Also, currently underway is another study motivated by George—the PrePoint study. 42 This is a primary prevention pilot study evaluating oral or nasal insulin in very high-risk children with genetic markers, to determine whether this might prevent the emergence of islet autoantibodies.
Another insulin-based approach is the use of pro-insulin peptides as immunotherapeutic vaccines. 43 To date, only a Phase 1 safety study has been reported, but further studies are underway.
Another antigen that has been evaluated in several trials is glutamic acid decarboxylase (GAD). In recent-onset T1D, several trials using a GAD-alum vaccine have been conducted. A pilot study looked promising, 44 but three larger trials failed to show a benefit on preserving residual β-cell function. 45 –47 A randomized controlled prevention study is currently taking place in Sweden, in which 50 children with at least two diabetes autoantibodies, including anti-GAD, have been enrolled. 48 Also underway is a study in recent-onset T1D combining GAD vaccine, vitamin D, and ibuprofen. 49
In his 2009 Banting Lecture to the American Diabetes Association, George described the importance of the “trimolecular complex” of insulin peptide being presented by major histocompatibility complex (MHC) class II to a specific T-cell receptor (TCR) V-alpha. 50 He focused on work on this complex from then until the time of his death, asserting that the primary trimolecular complex was a clearer therapeutic target for interdicting T1D. 51 Thus, he and his colleagues have explored several ways of impacting the T1D disease process in NOD mice via interference with the trimolecular complex. One approach is vaccination with a mutated recombinant insulin peptide–MHC complex, which delayed development of autoantibodies and of diabetes in NOD mice. 52 A second approach has involved a structure-based approach to identify small molecules that can either enhance or inhibit specific TCR signaling in the presence of target peptides. 53 The latter approach identified glyphosine as a molecule that alters insulin peptide presentation to TCR and prevents diabetes in NOD mice. 53 Further studies are in progress to identify small molecules that might be tested in human clinical trials.
Although mostly interested in antigen-based therapies, George also served as a member of the Steering Committee of Type 1 Diabetes TrialNet 30 and of the Network Steering Committee of the Immune Tolerance Network, 54,55 both of which have been conducting trials in T1D with various immunomodulatory approaches. Studies have also been conducted outside of these networks.
In recent-onset T1D, to date there have been three approaches that have shown promise.
Anti-CD3 monoclonal antibodies selectively deplete pathogenic T-lymphocytes while preserving regulatory T-lymphocytes. 56 In studies with two different anti-CD3 monoclonal antibodies, short treatment courses of 14 or 6 days in recent-onset T1D have shown preservation of residual β-cell function for several years, 57 –60 and another study has shown beneficial effect even when treatment has commenced beyond the initial period after diagnosis. 61 Unfortunately, the anti-CD3 landscape has become confused because of failure of large Phase 3 clinical trials to meet their primary efficacy outcome measure. 62,63 It has been highly debated whether the Phase 3 trials were appropriately designed. 64 Thus, it is likely premature to abandon anti-CD3 approaches. Indeed, anti-CD3 is being pursued by TrialNet as a therapy to prevent progression from altered glucose tolerance to clinical T1D. 65
The anti-CD20 monoclonal antibody rituximab depletes B-lymphocytes, which may have a role in facilitating activation of T-lymphocytes. 66 Rituximab, given in recent-onset T1D as weekly infusions for 1 month, compared with placebo preserved residual β-cell function for 2 years. 67,68
Abatacept (CTLA4-Ig) is a “second signal” co-stimulation blocker that prevents activation of T-lymphocytes. 69 Given monthly over 2 years, it also preserved residual β-cell function in recent-onset T1D. 70 That effect was sustained for 1 year following cessation of therapy. 71
All three of these approaches that showed beneficial effects on residual β-cell function—anti-CD3, anti-CD20, and co-stimulation blockade—resulted in only transient benefit, as subsequent to initial improvement there was a progressive decline in β-cell function parallel to that seen in the respective placebo groups. 57,58,67,70
Several other interventions—mycophenolate mofetil with or without concomitant dacluzimab, 72 anti-interleukin-1β blockade with either the monoclonal antibody canikinumab or the interleukin-1β receptor anatagonist anakinra, 73 or the T-cell-depleting drug thymoglobulin 74 —failed to show beneficial effect on preservation of residual β-cell function.
In a small uncontrolled pilot study in recent-onset T1D, the combination of cyclophosphamide, high-dose thymoglobulin, and granulocyte colony-stimulating factor, together with rescue therapy of autologous human bone marrow transplantation, had an apparently beneficial effect as evidenced by cessation of insulin therapy in the majority of patients treated. 75 –77 A pilot study is currently underway to study this type of approach further, but with a milder combination: low-dose thymoglobulin plus granulocyte colony-stimulating factor. 78
Several other studies are currently underway or being planned. It is our bias that combination therapy, involving several pathways, will be required to effectively intervene and sustain residual β-cell function for a protracted period of time. 79 It was George's hope that others would carry on to achieve what he did not live to see—namely, the prevention and reversal of T1D. Fortunately, George's legacy includes a large number of former Fellows and trainees that he inspired to work in the field of immunopathogenesis and immunotherapy of T1D. They are likely to achieve this goal for him. To do so would be quite fitting, as George was an extraordinary mentor who demonstrated an incredible willingness to collaborate, to share data, to offer help to anyone in the field. He always had an air of excitement, like a young boy, thrilled to see the field advance. He will be missed, but we who continue to work in the field will fulfill his goal. Of that, we are certain.
Footnotes
Author Disclosure Statement
No competing financial interests exist.