
Abstract
Background:
Several countries restrict individuals with type 1 diabetes mellitus (T1DM) from skydiving because of concerns over possible alterations in consciousness. To our knowledge, glucose levels and working memory in individuals with T1DM during skydiving have not been assessed earlier. The objective of this study was to investigate changes in glucose levels and working memory in selected subjects with T1DM compared with control subjects without diabetes mellitus (DM) during ambient air pressure changes as those anticipated during standard skydiving.
Subjects and Methods:
Six subjects with T1DM and six controls were included. Using a hypobaric chamber, the ambient air pressure was changed to simulate a standard skydive from 4,000 m (13,000 feet) above mean sea level. The procedure was repeated six times to mimic a day of skydiving activity with a median of 8.7 h/day (5th, 95th percentile: 8.1, 9.8 h). All subjects carried a continuous glucose monitor (CGM). Capillary glucose tests were taken in order to calibrate the CGM. Hemoglobin oxygen saturation, heart rate, and working memory, evaluated through digit span, were monitored regularly.
Results:
No subject experienced documented symptomatic hypoglycemia with impaired working memory during the simulations. One asymptomatic hypoglycemia episode with a plasma glucose level of <3.9 mmol/L was recorded in a subject with T1DM, with a corresponding CGM trend indicating declining glucose levels. Interstitial glucose levels of <3.9 mmol/L were recorded by CGM in three of the controls during the simulations. There were no significant differences in hemoglobin oxygen saturation, heart rate, or working memory between the T1DM patients and the controls.
Conclusions:
This study of interstitial glucose levels and working memory could not show the activity-specific risk factor (i.e., repetitive rapid-onset hypobaric hypoxia exposures) to be a greater safety concern for selected subjects with T1DM compared with subjects without DM during a simulated day of skydiving. Further studies are needed to clarify the suitability of subjects with T1DM to participate in this air sport.
Introduction
W
With improved treatments and the development of new pharmacological agents, individuals with type 1 DM (T1DM) can achieve better metabolic control. 2,3
Hypoglycemia is generally defined as a plasma glucose (PG) level of <3.9 mmol/L. A working group of the American Diabetes Association and the Endocrine Society has further subdivided hypoglycemia into severe hypoglycemia, documented symptomatic hypoglycemia, asymptomatic hypoglycemia, probable symptomatic hypoglycemia, and pseudohypoglycemia. 4 These definitions were used in this study.
Stehno-Bittel 5 described the positive physical effects of sports participation in individuals with T1DM and summarized the results of various studies. However, restrictions are present in the lives of individuals with DM regarding participation in many sports because of concerns over possible alterations in consciousness.
One of the objectives of the International Diabetes Federation is to remove any social stigma and discrimination associated with DM, as stated in the St. Vincent Declaration. 6 During the annual meeting of The Swedish Society of Medicine in Gothenburg in 2010, the issue of possible persistent discrimination was voiced by DM patient groups at a symposium about DM and so-called risk sports. Sports discussed included SCUBA diving, mountain climbing, and air sports. One sport mentioned in particular was skydiving (i.e., sport parachuting from aircraft). The patient groups expressed a strong desire for participation in this air sport, from which they are prohibited in Sweden as well as in several other countries, without clear medical evidence. Similar issues have been raised in skydiving community Web sites such as Dropzone.com, where DM has been widely discussed for many years, debating international regulatory inconsistencies, lack of guidelines, and advice for skydiving with diabetes in countries where this is allowed. The heterogeneity between the regulations of different countries concerning skydiving participation of those with T1DM was discussed during the Fédération Aéronautique Internationale/International Parachuting Commission meeting in Buenos Aires, Argentina, in February 2012. However, studies on glucose levels in individuals with T1DM during skydiving have not been published.
Several studies compared the glucose changes between individuals with DM and controls in sports, such as mountain climbing and SCUBA diving. 7 –10 However, these studies did not systematically investigate the effects of the concurrent stress experienced by the subjects. Because glucose levels may rise with higher stress, it is difficult to analyze any results based solely on glucose responses without accounting for factors such as physiological responses and alertness.
The functionality and accuracy of continuous glucose monitor (CGM) sensors in hypo- and hyperbaric environments ranging from 0.5 atm to 4 atm have been published, showing reliability of the sensors under these conditions in both subjects with T1DM and controls. 11
Working memory as a measure of cognitive ability during skydiving was studied earlier in healthy subjects. 12 –14 The Wechsler Adult Intelligence Scale (WAIS) is a valid psychological test and has been used worldwide to measure intelligence in adults and older adolescents since 1955. 15 The third edition (WAIS-III) was published in 1997, and it provided scores for Verbal IQ, Performance IQ, and Full Scale IQ, along with four secondary indices, including working memory. 16 The fourth edition was published in 2008 and is the version currently used. 17 The digit span forward subtest is used to measure the number storage capacity of the working memory. Participants are presented with a series of digits and must immediately repeat them back. If the task is completed successfully, they are given a longer list. The length of the longest list a person can remember is that person's digit span.
Because the cerebral functions are known to be highly sensitive to hypoxia, one might expect that environmental factors that can affect human physiological and psychological responses during skydiving more than height per se are the rapid changes in ambient air pressure, with related hypobaric hypoxia. Typical skydiving aircraft exit altitude is 4,000 m (13,000 feet) above ground level (AGL), and a standard “jump cycle” (pending drop zone logistics for aircraft loading and taxiing, aircraft type, and air traffic control considerations) may typically involve a few minutes on the ground on board the aircraft, 15–40 min of climb from ground level to exit altitude, and 1 min of free fall from 4,000 m AGL to 1,000 m (3,500 feet) AGL, where the main parachute is deployed, followed by 2–5 min of wing parachute flight down to landing. Regulations in Europe and the United States allow skydivers to ride up to 30 min without extra oxygen supply in a nonpressurized aircraft cabin between 3,000 m (10,000 feet) and 4,000 m above mean sea level (AMSL). 18,19 Aircraft type and air traffic control considerations are among variables that may prolong hypobaric hypoxia exposure toward this limit. At 4,000 m AMSL, the partial pressure of oxygen is approximately 60% of that at mean sea level.
The objective of this study was to investigate changes in glucose levels and working memory in selected subjects with T1DM compared with subjects without DM during ambient air pressure changes as those anticipated during standard skydiving.
Subjects and Methods
To be included in this study, subjects without DM had to be between 18 and 40 years of age and fulfill the medical examination and requirements for a skydiving license in Sweden. Subjects with T1DM had to fulfill the same requirements mentioned above including the medical examination, although regulations in Sweden prohibit individuals with T1DM from obtaining a skydiving license. Exclusion criteria for subjects with T1DM were any known long-term diabetes complications and/or documented severe hypoglycemia during the last year. The aim for the group with T1DM was to have glucose levels between 7 and 11 mmol/L prior to the first jump cycle.
The definitions of hypoglycemia or low glucose levels when measuring PG or interstitial glucose (IG) by CGM, respectively, and of severe hypoglycemia met the criteria established by the American Diabetes Association and the Endocrine Society. 4 Hyperglycemia was defined as having PG or IG>10.1 mmol/L.
Eight subjects with T1DM and eight controls were included in the study. Two subjects with T1DM were excluded prior to onset of the simulations because of poor metabolic control, and two of the controls were excluded because of CGM sensor failure prior to the start of the simulations.
All subjects with T1DM and one of the controls who did not have a skydiving license were medically examined. The subjects with T1DM were required to measure self-monitored blood glucose during a 14-day period before the simulations to record any recent metabolic instability that would not have been captured by measuring glycated hemoglobin. Hyperglycemic and hypoglycemic excursions were assessed based on 14-day self-monitored blood glucose values. These data were not recorded for the controls. PG measurements for calibration purposes were being assessed during the simulation.
There was no carbohydrate prefeeding protocol. The included subjects with T1DM dosed insulin in accordance to their own judgment based on the planned carbohydrate intake. The subjects could not see their glucose levels in real time, and hydration was not controlled.
An ambient air pressure profile was created to simulate a regular skydive involving the maximum exit altitude stand-by time allowed by international flight regulations without on-board oxygen. The simulations took a median of 8.7 h/day (5th, 95th percentile: 8.1, 9.8 h). A complete “jump cycle” took a median of 42 min (5th, 95th percentile: 25, 50 min), and the median ground-time between jump cycles was 35 min (5th, 95th percentile: 25, 65 min), with the lunch break excluded. The lunch break was during ground time between the third and the fourth cycle and took a median of 55 min (5th, 95th percentile: 55, 80 min). Using a hypobaric chamber (Kockums, Malmö, Sweden), the ambient air pressure was lowered, simulating aircraft ascent, from sea level pressure (open chamber door; Karolinska Hospital, Stockholm, Sweden) to 0.72 bar (approximately 3,000 m AMSL) in a median of 5 min (5th, 95th percentile: 4, 8 min). The median time from 3,000 m to maximum altitude (approximately 4,000 m AMSL, 0.63 bar) was 3 min (5th, 95th percentile: 2, 7 min), and the median time above 3,000 m AMSL was 29 min (5th, 95th percentile: 27, 31 min). The simulated free fall time from maximum altitude to approximately 1,000 m AMSL (0.90 bar) was 1 min, and the median simulated parachute flight time from 1,000 m to the ground was 4 min (5th, 95th percentile: 3, 6 min) (Fig. 1). The ambient air pressure in the chamber was controlled manually, monitored by a digital thermometer/barometer (TrackSense® Pro Logger, for temperature and pressure; Ellab A/S, Hillerød, Denmark), and the simulated altitude was measured by a standard skydiving altimeter (Neptune III, version 6.0.2; Alti-2, Inc., Deland, FL). The procedure was repeated six times to mimic a day of skydiving activity. All test subjects carried CGM sensors (iPro™2; Medtronic, Northridge, CA) during the simulations.
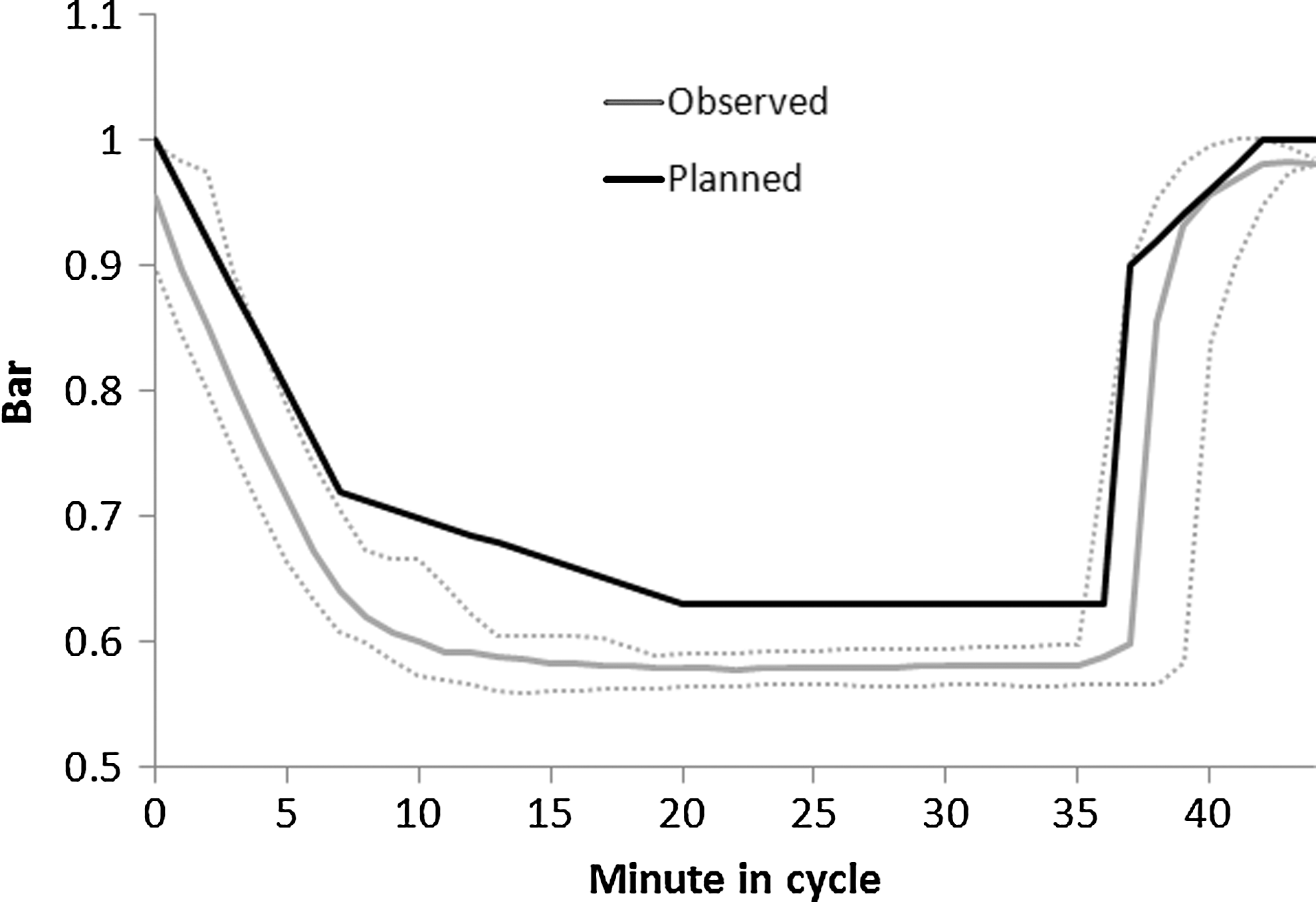
The planned ambient pressure curve (black line) and the median observed pressure curve (gray line) during the study investigating glucose excursions when changing ambient air pressure simulating skydiving. The striped lines show the 5th and 95th percentiles of the pressure distribution.
Capillary glucose (device from HemoCue®, Ängelholm, Sweden) was measured before and after each cycle and was taken in all subjects in order to calibrate the CGM. The aim for the group with T1DM was to have glucose levels between 7 and 11 mmol/L prior to the first jump cycle.
During the simulations, all subjects were served the same lunch with the exception of one individual with T1DM who, by bringing his own food, claimed that he could count his carbohydrate intake more accurately.
Heart rate and hemoglobin oxygen saturation were monitored in all subjects and were recorded before, during (every third minute), and after each cycle (Propaq® Encore 206-EL; Welch Allyn, Skaneateles Falls, NY).
Working memory was monitored by using the digit span forward. Digit span raw scores of 7 are average, <7 are low, and >7 are good scores. The digit span was administered by a licensed psychologist before, at the end of the stand-by at maximum altitude, and after each cycle to measure the working memory. Because of the special conditions during this study (group assessment instead of one subject at a time), the digit span was modified, after consulting licensed psychologists, by making the subjects repeat the digit span in writing instead of orally.
A medical staff member was present outside and inside the hypobaric chamber at all times during the simulations.
Descriptive statistical analysis, including estimation of 95% confidence interval (95% CI) for the time series of hemoglobin oxygen saturation and heart rate, was performed using Stata® version 11 (StataCorp, College Station, TX). Statistical significance was assessed based on nonoverlapping 95% CI values.
The local ethics committee approved this study (protocol number DNR 2011/1349-31/3).
Results
Baseline data for the subjects in each group are shown in Table 1. The actual ambient air pressure measured in the hypobaric chamber during the simulations compared with the planned pressure changes are shown in Figure 1. The altimeter used reacted as in authentic skydives.
Data are median (5th, 95th percentile) unless indicated otherwise.
The method of analysis was that of the International Federation of Clinical Chemists.
Glycated hemoglobin (HbA1c) and capillary hemoglobin (Hb) was measured for only one of the controls because the rest were licensed skydivers and did not need a new medical examination. The individual tested had values within the normal range.
Capillary Hb was measured with the HemoCue Hb 201+model.
BMI, body mass index; bpm, beats per minute; CSII, continuous subcutaneous insulin infusion; HR, heart rate; MAP, mean arterial pressure; MDI, multiple daily injections; NA, not applicable; SpO2, hemoglobin O2 saturation; T1DM, type 1 diabetes mellitus.
The glucometers from all subjects with T1DM were downloaded with seven-point profiles for the last 14 days prior to the simulations. Four subjects with T1DM had documented hypoglycemia on self-monitored blood glucose (nadir values of 2.2, 2.2, 3.1, and 3.4 mmol/L respectively), but no severe hypoglycemia episodes were documented.
Just prior to start of the first cycle, one documented asymptomatic hypoglycemia episode was recorded in a subject with T1DM with a capillary glucose of 3.3 mmol/L as well as a falling CGM trend indicating declining IG levels 60, 30, and 10 min prior to start of the simulations (13.5, 9.2, and 5.7 mmol/L, respectively).
The CGM sensors on the subjects were fully functional during the entire length of the simulation. The group with T1DM had mean IG levels between 7 and 10 mmol/L during the simulations (Fig. 2). Median IG levels in the group with T1DM 60, 30, and 10 min before starting the first cycle were 7.9 (5th, 95th percentile: 6.1, 13.5), 8.6 (5th, 95th percentile: 6.4, 9.2), and 7.8 (5th, 95th percentile: 5.6, 10.2) mmol/L, respectively. Mean IG levels in the group with T1DM varied from 6.0 (95% CI: 4.8–8.3) to 9.5 (95% CI: 7.6–10.9) mmol/L at the start of any cycle and from 6.6 (95% CI: 6.0–8.0) to 8.3 (95% CI: 6.0–11.1) mmol/L at the end of any cycle (Fig. 2). During CGM recordings, the median percentage of hyperglycemia and documented low glucose levels in the group with T1DM were 11.4% (5th, 95th percentile: 0%, 31.6%) and 0% (5th, 95th percentile: 0%, 31.3%) respectively during the simulations. One subject with T1DM experienced asymptomatic low glucose levels with an IG nadir of 2.2 mmol/L, and five subjects in the same group experienced hyperglycemia with an IG zenith of 13.0 mmol/L measured by CGM during the simulations. None of the controls experienced hyperglycemia; however, five episodes of asymptomatic low glucose levels were recorded in three of the controls, as measured by CGM (ranging between 2.2 and 3.7 mmol/L). IG levels were slightly but significantly higher in the group with T1DM after lunch (Fig. 2).
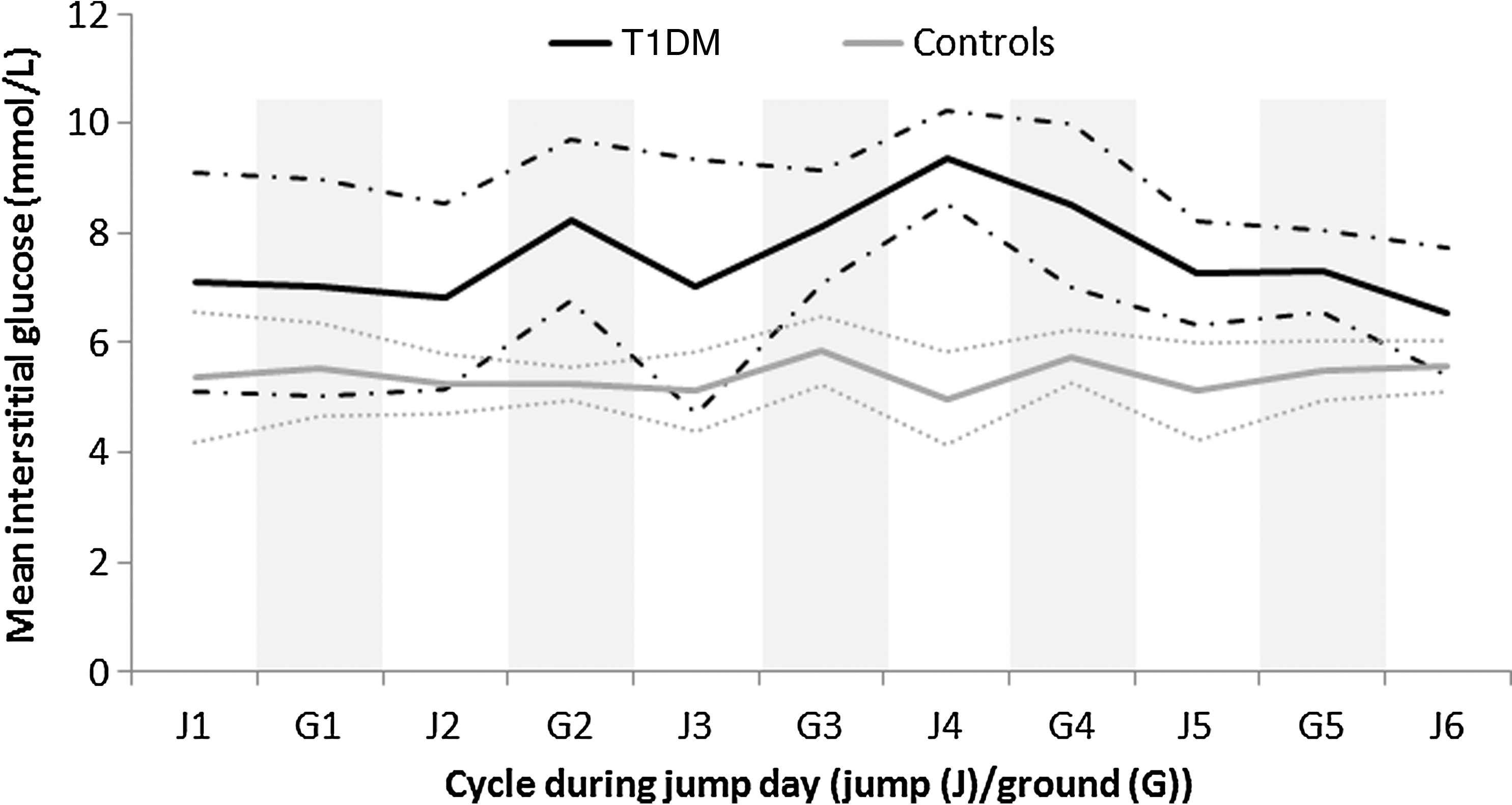
Mean interstitial glucose levels measured by continuous glucose monitoring in the group with type 1 diabetes mellitus (T1DM) (black line; n=6) and the controls (gray line; n=6) during the study investigating glucose excursions when changing ambient air pressure simulating skydiving. The striped lines show the 95% confidence interval. Gray bands indicate “ground” (G). White bands indicate “jump cycle” (J). A lunch break was taken between the third and the fourth jump cycles.
There were no significant differences in the hemoglobin oxygen saturation or the heart rate between the group with T1DM and the controls (Figs. 3 and 4). The hemoglobin oxygen saturation dropped, and the heart rate rose, showing a seemingly reverse proportionality in both groups with lowered ambient air pressure (Figs. 3 and 4). There were no significant differences in the results of the digit span forward between the two groups, and the results were not significantly affected before, during, or after the jump cycles compared with baseline (Fig. 5).
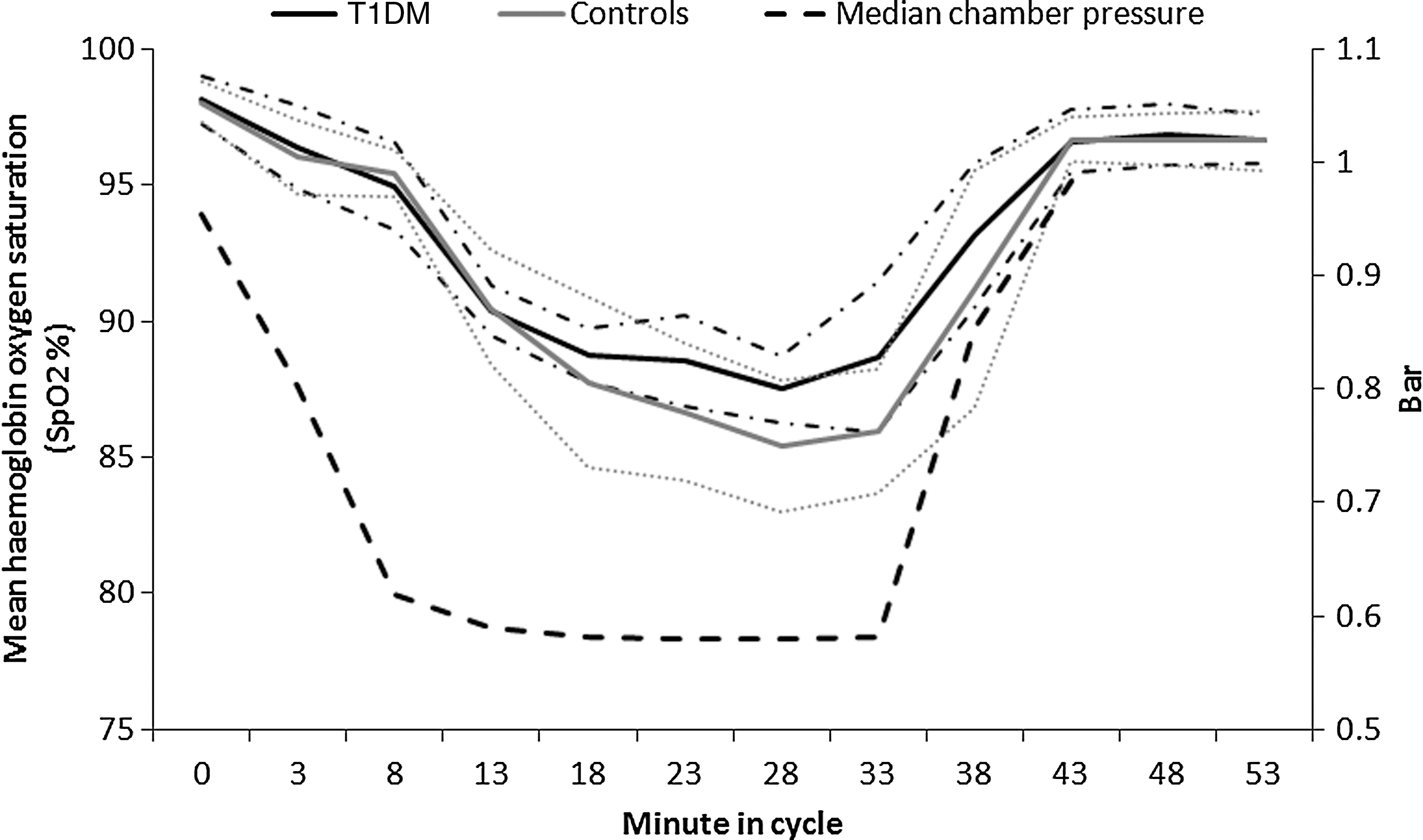
Mean hemoglobin oxygen saturation (SpO2%) in the group with type 1 diabetes mellitus (T1DM) (black lines; n=6) and the controls (gray lines; n=6) during the study investigating glucose excursions when changing ambient air pressure simulating skydiving. The striped lines show the 95% confidence interval. The dashed black line shows the median ambient air pressure in the chamber.
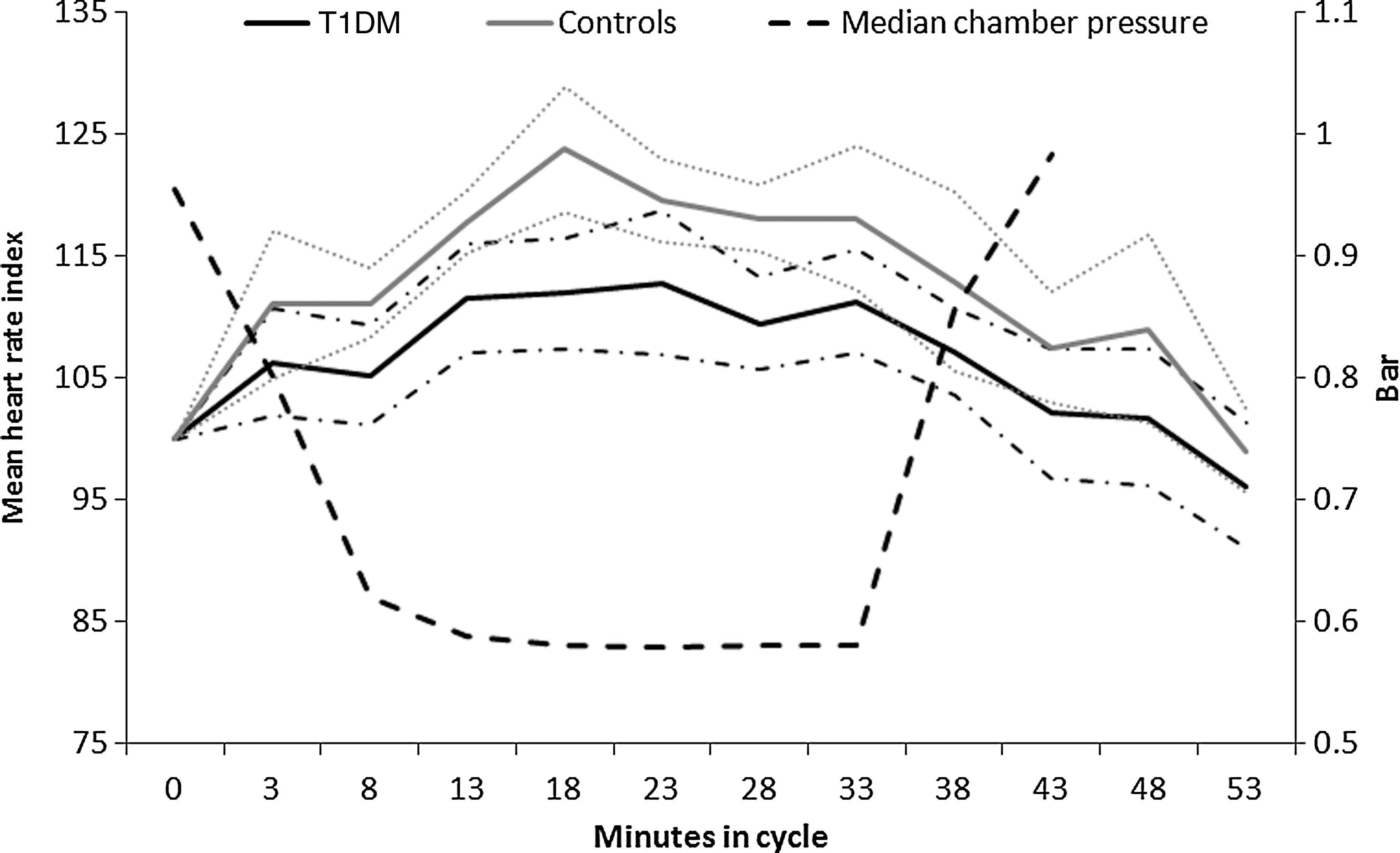
Mean heart rate index in the group with type 1 diabetes mellitus (T1DM) (black line; n=6) and the controls (gray line; n=6) during the study investigating glucose excursions when changing ambient air pressure simulating skydiving. A heart rate index of 100 indicated no difference in heart rate compared with baseline values. The striped lines show the 95% confidence interval. The dashed black line shows the median ambient air pressure in the chamber.

Results of the digit span forward test relative to baseline (span – baseline) before, at the end of the stand-by at the simulated 4,000 m altitude, and after the simulations in the hypobaric chamber during the study investigating glucose excursions when changing ambient air pressure simulating skydiving in the group with type 1 diabetes mellitus (T1DM) and the controls (n=6 in both groups). The boxplots show the median and the 25% and 75% interquartile range. The “whiskers” show the 5th and 95th percentiles. The dots show the most extreme observations outside this range.
Discussion
This study investigated glucose changes and working memory in selected subjects with T1DM compared with subjects without DM during ambient air pressure changes in a hypobaric chamber simulating a day of standard skydiving with repetitive skydives.
Published studies relating to individuals with T1DM and sports with dynamic ambient pressures, such as SCUBA diving and mountain climbing, have concluded that there are no contraindications for well-controlled individuals with T1DM to practice these sports, provided they fulfill a set of criteria. 8 –10,20
The psychophysiological arousal and anxiety of novice and experienced healthy sport parachutists were studied in several trials previously, and they showed that the differences between the two groups were either insignificant or minor. 13,14,21 –27
This is the first study, to our knowledge, that has investigated the activity-specific risk factor of hypobaric hypoxia during skydiving in a controlled environment. By the completion of this investigation, confounding factors such as psychological stress due to acrophobia could be excluded.
The sample size in this study was limited, which means that the absence of statistically significant differences could be due to a lack in power. However, the absolute differences seen between the two groups in hemoglobin oxygen saturation, heart rate, and working memory were of limited biological relevance and not of any medical concern. In fact, there was a tendency for the group with T1DM to perform better, something that could have been explored in a multivariable analysis taking factors such as age, sex, and other factors into account. However, this would have to be explored in a larger study.
The pressure changes captured by the altimeter during the simulations indicated similar changes as during actual skydives. It was easier to isolate the effects of dynamic hypobaric hypoxia on the subjects in a medically safe way in a hypobaric chamber compared with an authentic skydive.
Repetitive real-world skydives may induce greater stress than repetitive hypobaric chamber confinements, leading to more unpredictable glucose responses. Other factors such as poor caloric intake, thermal stress, and unforeseen delays could also have an impact on glucose levels and need to be studied further.
Because a skydiver receives multiple, simultaneous stimuli (vision, balance, awareness of the surrounding airspace) during a real-world skydive, working memory might be more affected compared with that while being maintained in a hypobaric chamber. However, because this has not been studied in this context earlier, it was necessary to investigate working memory as baseline prior to future field studies.
Six skydives per day constitutes a medium level of activity for an experienced skydiver, but a high level for a novice. Consequently, by repeating the procedure six times, a normal to intense day of skydiving has been mimicked.
After lunch, the IG levels in the group with T1DM were significantly higher than in the controls. The subjects with T1DM administered the insulin dose they judged to be the most appropriate. It is common to decrease the insulin dose before exercise and in new environments. The subjects might therefore have underestimated the prandial insulin dose required to achieve normoglycemia during the simulations.
Because only subjects with well-regulated T1DM were included in the study, the results do not reflect the effects of hypobaric hypoxia when skydiving for individuals with poor metabolic control and many high/low glucose excursions.
CGM recordings of both subjects with T1DM and controls have in hyperbaric and hypobaric environments shown acceptable mean absolute relative difference values: hypobaric (14.9%) and hyperbaric (6.7%). 11 Many of the marketed CGM systems have a tendency of less accuracy in the lower glucose level range and during rapid changes of glucose levels with a risk of overestimating hypoglycemia. Although the accuracy of CGM devices has improved, a CGM cannot fully replace PG measurement. 10,28,29 This might have overestimated the risk of low IG levels in both the group with T1DM and the controls.
Digit span is a valid instrument used in psychology to measure working memory. 30 The effects of the modification made were not tested prior to the study, but a licensed psychologist and leading expert in this field was consulted and approved the modification design. Both groups in this study had average baseline digit spans; however, the group with T1DM had digit spans in the lower range (Table 1). Because different randomly selected digit spans were used for each jump cycle, there was no risk that the results were confounded by learning.
The rise of heart rate during the simulations could be a physiological compensation for the hemoglobin oxygen saturation drop due to lower ambient air pressure. Figures 3 and 4 support this phenomenon, showing a reverse and synchronous relationship.
Conclusions
This study of IG levels and working memory could not show the activity-specific risk factor (i.e., repetitive rapid-onset hypobaric hypoxia exposures) to be a greater safety concern for selected subjects with T1DM compared with subjects without DM during a simulated day of skydiving. No significant differences in working memory between the group with T1DM and the controls were found. The hemoglobin oxygen saturation dropped, and the heart rate rose, showing a reverse and synchronous relationship to the drop in ambient pressure. Further studies are needed to clarify the suitability of subjects with T1DM to participate in this air sport.
Footnotes
Acknowledgments
We thank Bengt M. Eriksson, Claes Frostell, Peter Kronlund, Peter Lindholm, Cecilia Engblom, Ola Jameson, and Håkan Nyman for moral support and assistance. We thank the manufacturers Medtronic, for kindly providing glucose sensors, and HemoCue, for kindly providing cuvettes and lancets. We thank the Research Council of the County of Värmland, Sweden for economic support.
Author Disclosure Statement
No competing financial interests exist.