
Abstract
George Eisenbarth devoted his life to understanding the basic immunology of the autoimmune polyglandular syndromes and type 1 diabetes, while providing exceptional clinical care to individuals afflicted with these disorders. Over the last 5 years, I was privileged to know George Eisenbarth as a mentor, colleague, and friend. His enthusiasm for science and specifically understanding the basic immunology of type 1 diabetes was infectious. George was the first to initially hypothesize that type 1 diabetes is a chronic autoimmune disorder. He made diabetes a predictable disease by developing biochemical assays to measure islet autoantibodies and provided this technology worldwide to researchers and the medical community. His work identifying and detecting islet autoantibodies allowed for clinical intervention trials aimed at preventing type 1 diabetes. George worked fervently to prevent the disease. During my time as a fellow in George's laboratory and faculty member at the Barbara Davis Center for Diabetes, we focused our efforts for diabetes prevention at the trimolecular complex (human leukocyte antigen molecule, self-peptide, and T cell receptor), which plays a pivotal role in diabetes pathogenesis. It is our belief that targeting this complex with safe and specific therapies will lead to the prevention of type 1 diabetes and an improved understanding as to why diabetes develops.
Introduction
The Trimolecular Complex
The trimolecular complex is composed of three components: an HLA molecule, self-peptide such as insulin, and a TCR on a CD4 T cell. HLA genes predispose risk for developing T1D and encode proteins, major histocompatibility complex (MHC) molecules, which present processed peptides to T cells. 7 The basic structural components of the trimolecular complex are depicted in the center of Figure 1. In his 2009 Banting Lecture at the American Diabetes Association Annual Meeting, George compared the elements of the trimolecular complex to a hotdog in a bun 8 : the bun is the MHC molecule, the hotdog is a peptide, and the TCR would be the individual eating the hot dog. In a typical bite, a person (TCR) consumes bun and peptide, analogous to a T cell interacting with a peptide bound to a MHC molecule. Understanding complex immunology and communicating those concepts to others in a comprehensible manner was a strength George possessed.
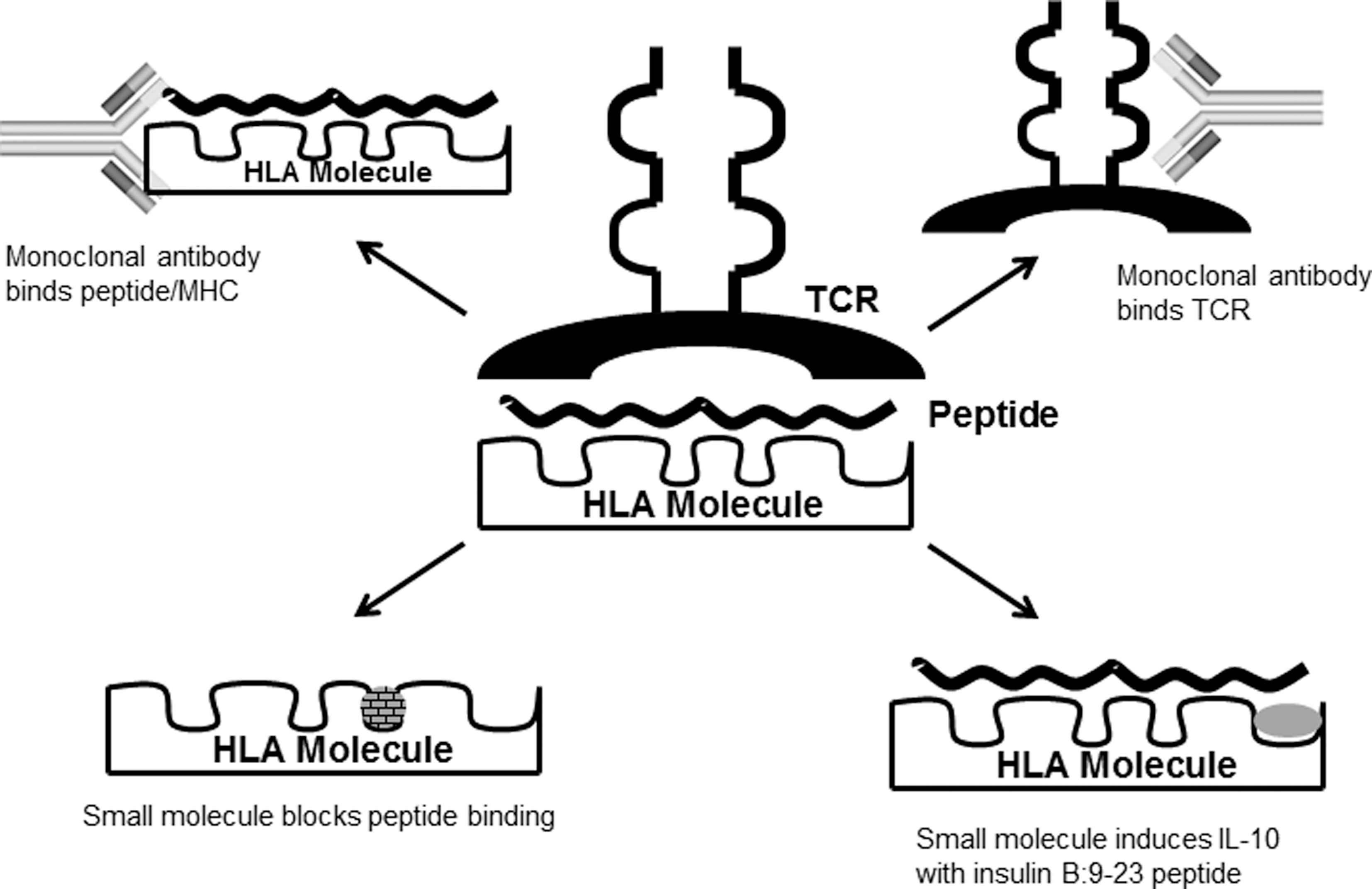
The components of the trimolecular complex and therapeutic approaches for targeting. The trimolecular complex consisting of a T cell receptor (TCR)–peptide–human leukocyte antigen (HLA) molecule. In order to block interactions, (1) a small molecule can occupy a pocket in a specific major histocompatibility complex (MHC) peptide binding groove, blocking peptide presentation to T cells, (2) a small molecule, such as glyphosine, can bind the MHC molecule and with an appropriate peptide induce a protective interleukin (IL)-10 response, (3) a monoclonal antibody can bind a specific peptide/MHC complex, thereby blocking T cell activation, or (4) a monoclonal antibody targets a specific TCR.
George initially reported that HLA genes were associated with autoimmune polyglandular failure in a New England Journal of Medicine article in 1978. 9 It was later discovered that certain HLA molecules, termed DQ8 and DQ2, predispose risk for developing T1D. 10 In fact, genome-wide association studies showed that the odds ratio for developing diabetes ranged from 6.5 to 11 when either of these genes is present. 11,12 Approximately 90% of all individuals with T1D have either a DQ8 and/or a DQ2 gene, with 50–60% of all T1D patients having DQ8. Furthermore, a certain HLA molecule, DQ6 (DQB*0602), protects from diabetes development with an odds ratio of only 0.03, indicating that T1D develops extremely infrequently when this gene is present. 11
With the understanding and knowledge that HLA genes contribute to T1D risk, proteins and peptides presented by these MHC molecules needed to be identified. George worked to identify islet antigens and then measure antibodies to these proteins in T1D patients and those at risk for developing diabetes (those with high risk HLA genotypes and a family history of T1D). 13 –18 Currently there are four islet autoantibodies that can be measured directed against insulin, GAD, a tyrosine phosphatase-like protein (IA-2), and the zinc transporter 19,20 ; all islet autoantibody assays are now available commercially throughout the world. Recent work from George's laboratory has resulted in the development of nonradioactive islet autoantibody assays that are more sensitive and specific than the previously used radioimmunoassays. 21 George had a particular interest in the insulin molecule, as evidenced by immunotherapy trials using both subcutaneous and oral insulin to prevent diabetes onset. 22 –24 In a spontaneous mouse model of autoimmune diabetes, the non-obese (NOD) mouse, he and his lab discovered that insulin is a primary autoantigen in the disease process. Specifically, insulin B chain amino acids 9–23 (B:9–23) contained an epitope necessary to drive T cell destruction of islet β-cells, as mutating a single amino acid in the insulin B:9–23 peptide sequence resulted in all mice remaining euglycemic and free of insulitis. 25,26 Of note is that the insulin B:9–23 amino acid sequence is identical in the mouse and the human. The NOD mouse model parallels human T1D in having homologous genes encoding MHC molecules predisposing disease risk, development of insulin autoantibodies, and spontaneous development of T cell infiltration in islets. 27 Recent analysis of the Diabetes Autoimmunity Study in the Young (DAISY) and Type 1 Diabetes Prediction and Prevention Project (DIPP) cohorts, which were screened for islet autoantibodies beginning at birth, revealed that insulin autoantibody titers correlate to diabetes progression (i.e., the higher the insulin autoantibody titers, the earlier in life diabetes developed, and lower titers had longer time periods to diabetes onset). 28,29 Insulin has an important role in the development of T1D, especially in young children diagnosed with diabetes.
The final component of the trimolecular complex is receptors on T cells that recognize peptides presented by the MHC molecule. Studying T cells in the peripheral blood of patients has been an arduous task. 30 However, recent studies may shed light on the manner in which insulin peptides are presented by MHC molecules to T cells. These studies highlight the importance of the “register” of insulin peptide binding to MHC molecules such that polymorphisms in HLA genes may lead to identical insulin peptides being presented, or “shown,” to T cells in different registers. 31 –33 For example, we hypothesize that the insulin B:9–23 peptide may be presented differently by HLA-DQ8 or -DQ2 as opposed to the protective HLA-DQ6. Development of T cells with specificity for insulin may be changed depending upon a given HLA molecule such that DQ8 and DQ2 have the potential to lead to diabetes development. George wholeheartedly believed that the studying the components of the insulin trimolecular complex in the mouse and the human would lead to a better understanding as to why T1D develops.
Therapies Targeting the Trimolecular Complex
With the components of the trimolecular complex in place, George hypothesized that targeting each part may lead to novel therapies capable of preventing T1D in humans (Fig. 1). As a new energetic Fellow in George's lab, one of my initial projects was to target the MHC Class II molecule of the NOD mouse and DQ8, the homologous molecule in the human. With our collaborators from the University of Florida in Gainesville, in silico molecular modeling and docking with a supercomputer were used to identify potential small “drug-like” molecules capable of binding to pockets along the MHC peptide binding groove. A library of approximately 140,000 compounds from the National Institute of Health Developmental Therapeutics Program was screened in which each compound was placed in 1,000 orientations by a supercomputer into each of four pockets that anchor peptides to MHC molecules. Those small molecules with the highest predicted energy of binding were screened with a bioassay in George's lab. We were able to identify several compounds that blocked peptide binding specifically to a given MHC molecule, which resulted in T cells not being activated. One compound, tetraazatricyclododecane, blocked stimulation of T cells responding to whole insulin, necessitating endocytosis, processing, and presentation of insulin peptides. The compound also inhibited T cell activation in the presence of whole NOD islets, which have been shown to contain insulin peptides including B:9–23. 34 Tetraazatricyclododecane was also predicted to bind to the human DQ8 peptide-binding groove and blocked activation of a human B:9–23-responsive T cell. 35 It is conceivable that small drug molecules that specifically block DQ8 antigen presentation to T cells will delay or prevent diabetes onset.
To our surprise, we found several compounds effective at enhancing T cell responses. One of these compounds, glyphosine, was studied in further detail and found to enhance protective T cell responses. In the presence of glyphosine and the insulin B:9–23 peptide, interleukin (IL)-10 was produced from both NOD mouse spleen cells and human peripheral blood mononuclear cells from T1D patients having HLA DQ8. 35 IL-10 is an anti-inflammatory cytokine and is associated with regulatory T cells. 36,37 Furthermore, glyphosine was able to prevent diabetes onset in the NOD mouse while therapy was administered. We hypothesize that glyphosine changes the register of insulin B:9–23 presentation to T cells resulting in an IL-10 response. 38
Using the trimolecular complex as a roadmap to design novel and specific therapies for diabetes prevention, others have had success developing and preventing diabetes in preclinical models. Li Zhang, a fellow in George's lab, developed a monoclonal antibody that binds to both the insulin B:9–23 peptide and MHC molecule of the NOD mouse. 39 Interfering with peptide presentation then blocks the ability of a T cell to become activated. Conceptually, a monoclonal antibody to any peptide/MHC complex could be generated for disease intervention as long as the pathogenic peptide and register of binding to a MHC molecule are known.
Antigen-specific therapies have been used in several clinical intervention trials for diabetes prevention and in new-onset patients. 40 The insulin B:9–23 peptide has been well documented to prevent and delay diabetes onset in NOD mice. 41,42 A recent study using knowledge regarding the “register of binding” to a MHC molecule found that a low dose of an insulin B:9–23 mimotope protected against diabetes in NOD mice early in the disease course before insulin autoantibodies developed. 43 The mimotope peptide had a single amino acid substitution (B22 arginine to glutamic acid) allowing binding to the mouse MHC Class II molecule in the appropriate register for T cell activation. Treatment with a continuous low dose of the mimotope peptide but not native insulin B:9–23 resulted in regulatory T cells and diabetes prevention. The register of peptide presentation by a given MHC molecule, dose, and frequency of dosing are all important considerations in antigen-specific therapies for T1D. 40,44
Finally, therapies targeting TCRs involved in diabetes onset in rat models of autoimmune diabetes have been assessed. Specific TCRs in these rat models have been targeted with a monoclonal antibody to prevent diabetes development. A specific β-chain of the TCR, Vβ13, is found in the CD4 T cells infiltrating the islets in these animal models. 45 A depleting monoclonal antibody directed against Vβ13 prevented diabetes onset in a spontaneous autoimmune diabetes rat model and a model in which diabetes is induced by activation of the innate immune system. 46
Conclusions
Our foundation for understanding T1D pathogenesis as an immunologic autoimmune disorder occurring in stages comes from the lifelong work of George Eisenbarth. As previously mentioned, T1D is a predictable disease because of the biochemical islet autoantibody assays developed by George and his colleagues. With the ability to predict disease development, diabetes prevention will naturally follow. George was passionate about preventing diabetes throughout his career. The focus of designing safe and specific therapies targeting the insulin trimolecular complex is a rational approach. Having a well-defined molecular target and tailoring therapies to specific HLA genes is truly personalized medicine, which George believed would ultimately prevent T1D. Translating these novel therapies from bench to bedside was a major focus for George, and the future holds promise for targeting the components of the trimolecular complex to prevent diabetes.
Footnotes
Acknowledgments
This work was supported by grants from the National Institute of Diabetes and Digestive Kidney Diseases (RO1 DK032083 and K08 DK09599), the Juvenile Diabetes Research Foundation, the Children's Diabetes Foundation, and the Brehm Coalition.
Author Disclosure Statement
No competing financial interests exist.