
Abstract
Background:
Sedentarism in the workplace, which accelerates risk of diabetes, is least explored in the Indian population. The primary objective of this study was to assess whether prolonged sitting hours in work place predisposes individuals to risk of diabetes and also to estimate risk of diabetes in sedentary workers with a positive family history of diabetes (FHD).
Subjects and Methods:
Data of age-matched 514 subjects previously undiagnosed with diabetes from two different occupational groups (bank employees and schoolteachers) in Chennai, India from opportunistic screening were taken for analysis. The important explanatory variables were body mass index, waist circumference, duration of physical activity, positive FHD, and random capillary blood glucose (RCBG). Logistic regression analyses were done separately to identify determinants of diabetes in each group. Another logistic regression was performed after combining data to estimate risk associated with diabetes among sedentary subjects with positive FHD.
Results:
Factors associated with elevated RCBG among schoolteachers were systolic and diastolic blood pressure, whereas among bank employees, in addition to blood pressure, duration of sitting in work place and positive FHD were significantly associated with diabetes. Combined data analysis showed that subjects with duration of sitting of ≥180 min/day and a positive FHD are three times at risk of developing diabetes. Adjusting for total physical activity revealed that risk was higher among male subjects.
Conclusions:
Increased sitting duration for ≥180 min/day at the workplace was associated with elevated RCBG. There was a threefold higher risk for diabetes among these subjects with positive FHD. Encouraging physical activities in such groups, particularly in men, can be beneficial.
Introduction
D
In India, according to the 2001 census, the work force consisted of more than 400 million people, constituting about 40% of the total population. 4 The economically productive age group spends most of their time in the workplace in India, with an average contractual weekly working time of 48 h. 5 Because of the rapid increase in mechanization of jobs in various occupational groups, the amount of physical activity in the work places has been decreasing among people, which has resulted in the rise of sedentary jobs. Sedentary work is defined as a job that demands that the majority of the time be spent in sitting, with occasional walking and standing. 6
In general, there are several studies to support the stronger association of sedentarism with the development of obesity, cardiovascular disease, and diabetes. 7 –9 About 1.2 million healthy U.S. individuals were followed up for a period of 14 years, and it was observed that the mortality rate was higher among those who spent sitting ≥6 h/day in leisure time after adjusting for other associated factors such as body mass index and smoking. 10 Choi et al. 11 reported that a low physical activity level at the workplace was associated with increased prevalence of general as well as central obesity. There are studies that have dealt with the association between prolonged sitting hours and the prevalence of cardiometabolic risk factors. 12,13
In general, there is a dearth of information on occupational risk factors associated with noncommunicable diseases in low- and middle-income countries. 14 In India, although there are not many studies to show the association between sedentarism and development of diabetes, the beneficial effects of physical activity in preventing or delaying the onset of diabetes among subjects with prediabetes has been documented. 15 Therefore, the current study was planned to assess the sedentary duration and physical activity level at workplaces of two different occupational groups and their association with random capillary blood glucose (RCBG) levels. It was also aimed to estimate the risk of development of diabetes in these subjects due to sedentary profession and the presence of a positive family history of diabetes (FHD).
Subjects and Methods
The data for this study were retrieved from various opportunistic screening programs for diabetes carried out in different occupational groups by the Department of Epidemiology in a specialized diabetes tertiary-care center during the period of January–December 2011 across Chennai city in the state of Tamil Nadu, India. The screening programs were conducted in two occupational groups: the banking sector (Group 1) and schoolteachers (Group 2). The total number of subjects screened was 747 from two banks and three schools, and from of these subjects, data of 94 subjects with a previous diagnosis of diabetes and 139 subjects whose age did not match were excluded from the analysis. Data of the remaining 514 age-matched individuals from the two groups were included for the final analysis as shown in Figure 1. Written consent was obtained from all the subjects at the time of screening, and the ethics committee of the Prof. M. Viswanathan Diabetes Research Centre, Chennai, approved the study.

Flowchart showing the details on selection of study subjects.
The screening was conducted by a team consisting of a medical officer, a physiotherapist, a phlebotomist, and social workers. Sociodemographic details, FHD, and details on the presence of hypertension were collected. The presence of a positive FHD was ascertained if the study subjects gave a history of diagnosis of diabetes among their blood relatives, irrespective of the fact whether they were alive or dead. Anthropometric and blood pressure measurements were taken, and body mass index (BMI) was calculated from the height and weight measurements and categorized, as per Indian obesity guidelines, as follows: normal BMI, 18.0–22.9 kg/m2; overweight, 23.0–24.9 kg/m2; and obesity, ≥25 kg/m2. Similarly, waist circumference was measured, and male subjects with a waist circumference of ≥90 cm and females with ≥80 cm were categorized as subjects with central obesity. 16
A set of questions was administered to assess the duration of the activities such as sitting, standing, and walking during the subjects' work routine. For example, to assess the time spent for walking, the question posed to the subject was “How many hours and minutes do you spend for walking at your workplace?” Similar questions were put forth for collecting information regarding sitting and standing. The self-reported duration of time spent in sitting, standing, and walking per day in the workplace was recorded from their responses. The duration of these activities was taken into consideration if it was >10 min and 30 min less than their reported total working hours per day. Involvement in leisure time physical activity (LTPA) after office hours, if any, and the type and duration of LTPA were collected for a week, and the average duration per day was calculated.
The RCBG test for diabetes was performed for each subject using a glucometer (One Touch® Ultra; Life Scan, Mumbai, India). In an earlier study conducted among a similar population, an RCBG level of ≥140 mg/dL showed higher sensitivity and specificity in diagnosing diabetes compared with all gold standard diagnostic methods for diabetes. 17 Based on this study, subjects with an RCBG level of ≥140 mg/dL were considered to be in the high-risk group for the present study. The study subjects in each group were subdivided into groups as to those with an RCBG value of <140 mg/dL and ≥140 mg/dL. Because of the lack of a general recommendation on maximum sitting hours per day to prevent adverse health outcomes in the Indian population, data from the two groups were pooled, and a χ 2 test was performed after categorizing the sitting duration to determine the association with RCBG groups. The sitting duration of ≥180 min/day was thus identified as the cutoff value to categorize the study subjects as sedentary and nonsedentary groups. Furthermore, all the study subjects were categorized into four groups as follows: those who had a positive FHD but who spent <180 min/day in sitting at the workplace formed Group II; all those with a negative FHD but who spent ≥180 min/day in sitting in the workplace were labeled as Group III; subjects with both positive FHD and who spent ≥180 min/day in sitting in the workplace were categorized as Group IV; and Group I was the reference group, with a negative FHD and who spent <180 min/day in the sitting position.
Statistical analysis
Descriptive statistics such as mean with SD and proportions were reported for continuous and categorical values, respectively. Logistic regression analysis was performed separately for each group with RCBG level of ≥140 mg/dL as the dependent variable and with RCBG level of <140 mg/dL as the reference group. The independent variables entered were age, gender, FHD, family history of hypertension, duration of sitting, standing, and walking in workplace, involvement in LTPA, duration of LTPA, systolic and diastolic blood pressure measurements, BMI, and waist circumference.
Another logistic regression analyses were done with RCBG level of ≥140 mg/dL as the dependent variable and three risk groups as independent variables. Estimation of risk of diabetes was done with three different models: Model 1, unadjusted for age and gender; Model 2, adjusted for age and gender; and Model 3, adjusted for age, gender, and the duration of other physical activities undertaken by the subjects. SPSS version 16.0 software (SPSS Inc., Chicago, IL) was used for performing all statistical analyses. A value of P<0.05 was considered as statistically significant.
Results
The data of 514 (male:female, 234:280) age-matched study subjects were included in this analysis. There were 244 subjects (male:female, 172:72) in Group 1 and 270 (male:female, 62:208) in Group 2. The general characteristics of study subjects are given in Table 1. There was no significant difference in mean age of the study subjects between Group 1 and Group 2 (P=0.565). The difference in mean BMI of the study subjects between the two groups was not statistically significant (P=0.295). The mean waist circumference of men in Group 1 was higher than that of men in Group 2 (P<0.01), but this difference was not observed among women (P=0.486). About 80.7% of Group 1 subjects had central obesity, whereas it was 73.4% in Group 2 (P=0.034). The proportion of subjects with a positive FHD was similar between the two groups, whereas positive family history of hypertension was significantly higher in Group 2 (P=0.003).
Data are mean±SD values.
Values are n (%).
BMI, body mass index; F, female; M, male; RCBG, random capillary blood glucose.
The mean systolic blood pressure was similar between the two groups. The mean diastolic blood pressure was significantly higher in Group 2 (P<0.001). The number of subjects with an RCBG value of ≥140 mg/dL was 56 (23%) in Group 1 and 61 (22.6%) in Group 2, and the difference was not statistically significant (P=0.503).
Table 2 illustrates the duration of physical activity of study subjects in the work place in terms of duration of sitting, standing, and walking, and the other leisure time activities are expressed in min/day. The median duration spent in sitting was higher in bank employees compared with schoolteachers (420 vs. 120 min; P<0.001), whereas the median duration spent in standing was significantly higher in schoolteachers than in bank employees (300 vs. 120 min; P<0.001). Although the median duration of walking in schoolteachers and bank employees was the same (60 min), the mean rank was significantly higher in school teachers (165.4 vs. 126 min; P<0.001).The proportion of subjects involved in LTPA was higher in Group 1 (33.2%) than in Group 2 (28.5%); however, the difference was not statistically significant. There was no significant difference in the median duration of LTPA between the two groups (P=0.389). The majority of the study subjects (65.4%) of Group 1 and 44.2% of Group 2 reported walking as their LTPA. About 17.3% and 12.3% of bank employees and 31.2% and 22.1% of schoolteachers did aerobic exercise and yoga, respectively.
Values are n (%).
LTPA, leisure time physical activity.
Table 3 shows the results of binary logistic regression analysis in the study groups. Factors significantly associated with higher RCBG level in Group 1 (bank employees) were systolic blood pressure, with an odds ratio (OR) of 1.05 (95% confidence interval [CI] 1.02–1.08) (P=0.002), and positive FHD, with the highest OR (2.9) (95% CI 1.4–5.99) (P=0.004). Increase in the duration of sitting per minute was significantly associated with a higher RCBG value with an OR of 1.002 (95% CI 1.0–1.004) (P=0.032) (Table 3). Binary regression analysis for Group 2 (schoolteachers) showed that systolic blood pressure (OR=1.03; 95% CI 1.004–1.06) (P=0.026) and diastolic blood pressure (OR=0.95; 95% CI 0.91–0.99) (P=0.014) were associated with higher RCBG values (Table 3).
The dependent variable was random capillary blood glucose level ≥140 mg/dL versus <140 mg/dL.
Variables that were not significant were age, gender, positive family history of hypertension, body mass index, waist circumference, diastolic blood pressure, duration of standing or walking, and leisure time physical activity.
Variables that were not significant were age, gender, positive family history of hypertension, positive family history of diabetes, body mass index, waist circumference, duration of standing, sitting, or walking, and leisure time physical activity.
After the subjects were categorized based on the duration of sitting in the workplace for ≥180 and <180 min/day, bivariate analysis showed that there was significant association with higher RCBG values (P<0.002). The proportions of subjects with RCBG <140 and ≥140 mg/dL in the groups of subjects sitting in the workplace continuously for <180 and ≥180 min/day are reported in Figure 2. The proportion of subjects with an elevated RCBG level was significantly higher in the group with sitting duration of ≥180 min/day (27.8% vs. 16%) (P=0.001).
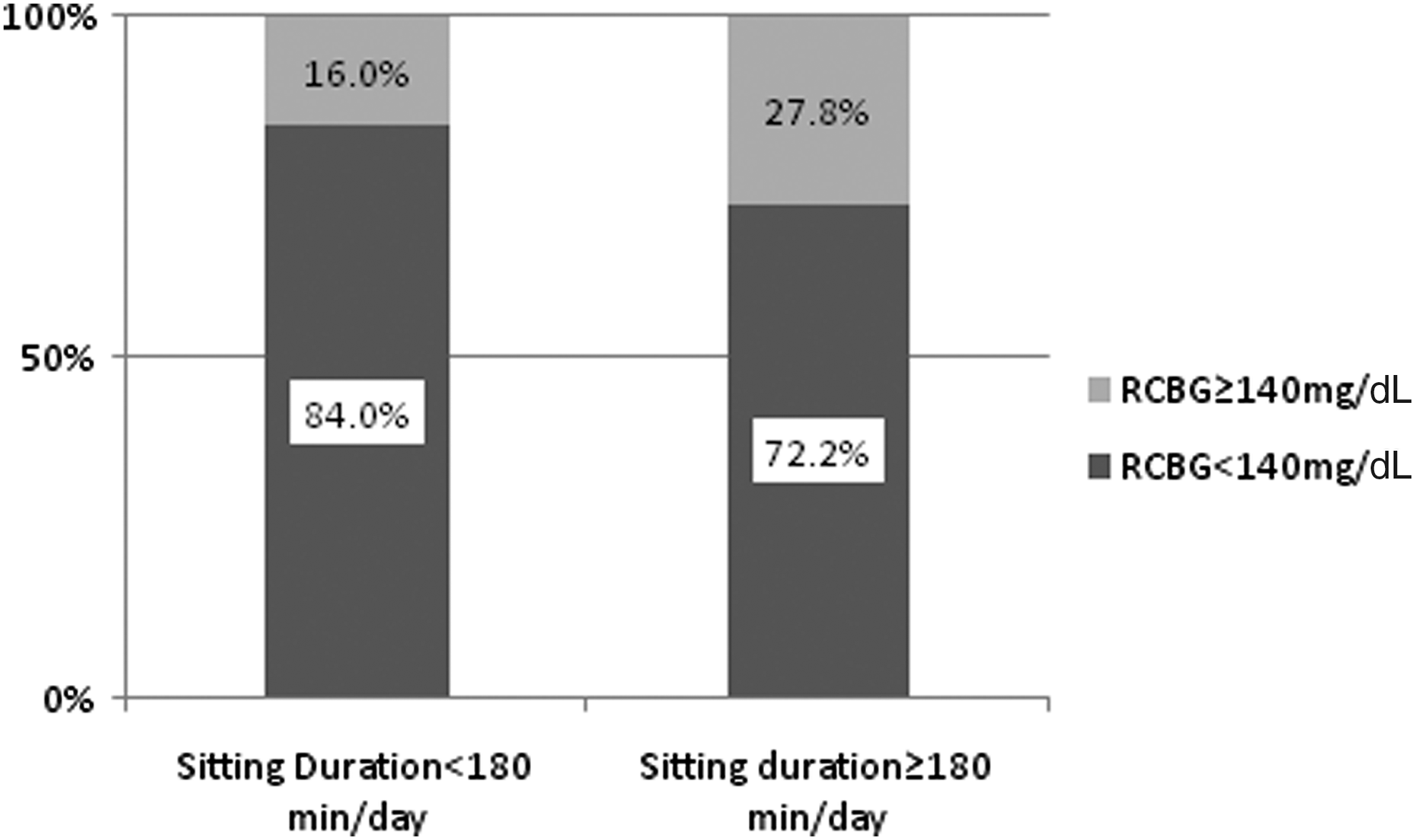
Proportion of subjects with random capillary blood glucose (RCBG) <140 mg/dL versus ≥140 mg/dL in the groups with sitting duration of <180 and ≥180 min/day.
Table 4 shows the results of logistic regression analysis estimating the risk for subjects with positive FHD and doing a sedentary job. The final model estimation showed that only Group IV subjects who had both FHD and spent ≥180 min/day in sitting in the workplace were at risk of having a higher RCBG value (OR=3; 95% CI 1.64–5.48) (P<0.0001). After adjusting for age and gender (Model 2), the risk remained same for Group IV subjects with a slight decrease in OR of 2.89 (95% CI 1.56–5.35) (P=0.001). Moreover, the analysis showed after adjusting for the duration of other activities such as LTPA, standing, and walking, the OR increased to 3.7 (95% CI 1.93–7.1) (P<0.0001). Male gender showed a significant risk after adjusting for physical activity compared with female gender as shown in Table 4.
The reference group (Group I) was sedentary <3 h and had no positive family history of diabetes. The dependent variable was random capillary blood glucose level ≥140 mg/dL versus <140 mg/dL. Model 1 was unadjusted, Model 2 was adjusted for age and gender, and Model 3 was Model 2 adjusted for physical activity. Group II was positive family history of diabetes only, Group III was sedentary duration ≥180 min/day only, and Group IV was sedentary duration ≥180 min/day and with positive family history of diabetes.
Discussion
This study highlighted the higher risk of diabetes for subjects with two risk factors (positive FHD and spending more than 3 h in sitting per day in the workplace). In the current study, the two occupational groups selected differed in demand of physical activity in the workplace. Bank employees performed a more sedentary job compared with schoolteachers. Although the two groups were age-matched, a significant difference was observed among the bank employees in the prevalence of central obesity (80.7%) compared with the schoolteachers (73.4%), with a significant difference in the mean waist circumference between men but not in women. However, there was no significant difference in general obesity between the two occupational groups.
There are several studies reporting a higher prevalence of generalized and central obesity among subjects with sedentary activities, highlighting them as a high-risk group for most of the noncommunicable diseases such as cardiovascular disease and diabetes. 18,19 A Delhi-based study among industrial workers showed that the general obesity was 58.5% (BMI >23 kg/m2) and central obesity (waist circumference >90 cm) was 43%. 20 Another study conducted in two industrial units in Chennai showed that 66.8% of study subjects had a BMI of >23 kg/m2 and that 70.2% of them had a waist circumference of >90 cm. 21
A previous report from Brazil also showed that compared with other occupational groups such as physicians, higher education professionals, and general and administrative service personnel in a healthcare center, nurses and health workers had a higher prevalence of diabetes, and increased waist circumference and sedentariness were the factors associated with them. 22
The proportions of subjects with high RCBG values did not differ between the groups in the present study. This may be attributed to the difference in the access to health care between the groups. Employees of the banking sector are more likely to have screening programs 23 –25 as well as facilities for annual screening of certain diseases and might have less of a chance of being undiagnosed with diabetes compared with the schoolteachers.
In the present study, separate regression analyses for the two groups showed systolic blood pressure measurement, positive FHD, and sitting duration at the workplace as the factors associated with higher RCBG values in subjects with sedentary jobs (bank employees). This particular association was not seen among the subjects with less sitting duration (schoolteachers) except for the blood pressure measurements. Our analyses also revealed that those with sedentary jobs having a positive family history and sitting continuously for more than 180 min in the workplace were 2.8 times at higher risk of developing diabetes compared with those without any of the above-mentioned risk factors. The study subjects with any one of the above two risk factors did not show any significant risk to develop diabetes. After adjusting for the duration of other physical activities, the OR estimated for the risk of diabetes increased, and males showed a significant association and were found to be at high risk of developing diabetes compared with females. So this finding implies that men with sedentary jobs can delay or prevent diabetes by being more active in their leisure time.
Similar to the findings in the current study, a cross-sectional study conducted among the bank employees in Surat, North India, showed a higher prevalence of hypertension and obesity. Moreover, the authors reported that male gender had a higher likelihood for prevalence of hypertension. 23 Another study conducted among 83,000 Japanese adults showed a stronger association of sedentary behaviors with increased death rate for men but not in women. 26 On the other hand, a prospective study conducted among a U.S. adult population by Patel et al. 10 reported that those with a 24 metabolic equivalent-h/week and sitting ≥6 h/day had a higher mortality risk due to cardiovascular disease for both men and women, but the risk was stronger for women. Yates et al. 27 also reported that increased sitting time in weekdays was positively associated with inflammatory biomarkers such as C-reactive peptide, interleukin-6, fasting insulin, leptin, and leptin/adiponectin ratio in women, but the association was not seen among men.
All the above studies were focused on the link between the total duration of sitting and physical activity level and mortality rates or cardiovascular risk, but in the current study the risk of development of diabetes and its association with duration of sitting in the workplace were evaluated. A recent review report showed a 112% increase in the relative risk of diabetes for sedentary subjects compared with nonsedentary subjects after doing a meta-analysis of 16 studies involving 794,577 subjects. 28 The duration of any kind of sedentary behavior has been positively associated with an increase in 2-h plasma glucose levels, 29 and this could be attributed to the decrease in insulin sensitivity associated with sedentary duration. The current study also showed that people with sedentary jobs are at risk of developing diabetes, but we have not estimated their insulin levels to assess insulin resistance among them.
The association of duration of sitting at the workplace for more than 3 h with the development of diabetes and the increase in the OR after adjusting for the duration of other physical activities clearly indicate that this particular high-risk group should focus on breaking the continuous sitting duration at the workplace and ought to be encouraged to participate in more physical activity, especially those with a positive FHD. Several studies have demonstrated that breaking long sitting hours resulted in the reduction of waist circumference, BMI, 2-h plasma glucose level, and triglyceride levels, to an improvement in insulin levels, and also a reduction in back and neck pain with an improvement in self-perceived health status. 30 –32 As such, a decline in the total physical activity level across the world population has been observed, 33 and it is evident that engaging in moderate physical activity reduces postprandial hyperglycemia, thereby improving other metabolic parameters as well. 34,35
There are a few limitations in the present study, such as the use of RCBG for categorizing the group as at risk for diabetes and the self-reported duration of activities. However, an RCBG level of ≥140 mg/dL was considered as the cutoff value, as it had the higher sensitivity and specificity for the fasting and postprandial glucose estimations from venous blood samples of an adequate number of people residing in the same region. 17
In conclusion, the sitting duration at the workplace, systolic blood pressure, and positive FHD were significantly associated with the development of diabetes in subjects involved in a sedentary profession. Moreover, the risk of onset of diabetes was three times higher in subjects with the combined risk factors of positive FHD and involvement in a sedentary occupation, demanding a sitting duration for ≥180 min/day. Enhancing leisure time physical activity and taking mobility breaks in between long sitting hours in the workplace should be recommended and encouraged among these high-risk groups.
Footnotes
Acknowledgments
We acknowledge the services rendered by the field team of the Department of Epidemiology. We thank Dr. V. Narayan Rao for his technical assistance in preparation of the manuscript.
Author Disclosure Statement
No competing financial interests exist.