
Abstract
Purposes:
Obesity and its correlation with other pathological conditions determine the onset of the metabolic syndrome, which exposes the patient to a higher risk of major cardiovascular complications. Laparoscopic sleeve gastrectomy (LSG) is a bariatric surgical procedure that appears to influence both the reduction of fat mass and the action of some gastrointestinal hormones.
Patients and Methods:
Between January 2011 and July 2013, 23 patients with morbid obesity underwent LSG and follow-up. In the evaluation of patients, the criteria for metabolic syndrome given by the International Diabetes Federation were followed. A multidisciplinary team of experts evaluated patients before surgery and in subsequent scheduled postoperative visits at 7, 30, 60, and 90 days and 4, 5, 6, 9, and 12 months. Anthropometric and metabolic parameters were analyzed.
Results:
The mean excess weight loss was 8.57±3.02%, 17.65±6.40%, 25.47±7.90%, 33.76±9.27%, 41.83±10.71%, 46.02±13.90%, 52.60±14.05%, 58.48±16.07%, and 62.59±21.29% at 7, 30, 60, and 90 days and 4, 5, 6, 9, and 12 months, respectively. In the same observational period there was an excellent improvement of metabolic indices. None of the patients previously taking prescribed hypoglycemic drugs restarted therapy. Mean fasting plasma glucose significantly decreased compared with the preoperative values. Blood pressure had a statistically significant improvement. Modification in the lipid profile was more variable. During the period of observation 22 of 23 patients reported in this study did not fit the criteria for metabolic syndrome.
Conclusions:
Morbid obesity and related diseases may benefit from a surgical approach in selected patients. Randomized controlled trials are needed to evaluate the role of LSG.
Background
M
The prospective study of Vanhala et al., 3 performed on a sample of individuals with an average age below 50 years, reports a risk of total and cardiovascular mortality within 10 years of diagnosis, more than three times higher in subjects with a clinical picture of metabolic syndrome compared with those who were affected by this condition. This initial study was followed by other studies 4,5 on samples of the general population, and the medical community has recognized that the syndrome is an independent risk factor with regard to morbidity and mortality.
According to the current American Diabetes Association and the National Heart, Lung, and Blood Institute guidelines, bariatric surgery is a treatment option to be offered to patients who have clinically severe obesity (body mass index [BMI] >40 kg/m2) or a BMI of >35 kg/m2 and serious comorbid conditions. 6,7 The laparoscopic sleeve gastrectomy (LSG) is the most recently introduced bariatric surgery technique and has already gained a broad consensus on its efficacy and safety. 8
We report the experience of our center in the treatment of a series of patients with morbid obesity (BMI >40 kg/m2) as part of a general metabolic syndrome clinical picture.
Patients and Methods
Between January 2011 and July 2013, 23 consecutive patients with morbid obesity underwent LSG and subsequent follow-up at the Department of Digestive Surgery and the Multidisciplinary Obesity Centre at the S. Maria Hospital, Terni, Italy.
A multidisciplinary team of experts, including an endocrinologist, nutritionist, internist, psychologist, and bariatric surgeon, evaluated patients. After careful evaluation of the patient's medical history, the anthropometric and metabolic parameters were recorded. Each patient was thoroughly informed about his or her medical condition and treatment options proposed and signed a written document consenting to surgery.
Surgical procedure
At our center and according to current guidelines, the sleeve gastrectomy was performed laparoscopically.
Pneumoperitoneum is performed with a Veress needle in the left subcostal region. The optical trocar is positioned at approximately 15 cm from the ensiform apophysis on the median. Three 12-mm trocars were placed on the left pararectal region and right and right subcostal region, respectively, and another trocar (5 mm) was inserted in the left paraumbilical region. Marking was performed on the large gastric curve at 6 cm from the pylorus. From this site, progressive skeletrization of the greater curvature was performed with an ultrasonic scalpel, and then the sectioning and coagulation of the vessels with release of the gastric fundus to the left diaphragmatic pillar were carried out to dissect the gastrophrenic ligament. After placement of an orogastric probe (36 Fr), vertical sectioning and suturing of the stomach (sleeve resection) were done on the guide of the probe with an Echelon60 stapler (Ethicon Endo-Surgery, Cincinnati, OH) (charged green and blue) up to the angle of His. After a thorough review and hemostasis of the suture, these were sealed with methylene blue. Finally, a nasogastric and an abdominal drainage in aspiration were placed. After removal of the specimen, trocars were removed under vision, and the surgical mini-incisions were sutured.
Criteria of the metabolic syndrome
In the evaluation of patients, we considered the definition given in 2005 by the International Diabetes Federation
9
: patients with central obesity (defined as waist circumference≥94 cm for Europid men and ≥80 cm for Europid women, with ethnicity specific values for other groups or, alternatively, a BMI of >30 kg/m2) and at least two of the following criteria: • Raised triglyceride levels: >150 mg/dL (1.7 mmol/L) or specific treatment for this lipid abnormality • Reduced high-density lipoprotein (HDL) cholesterol: <40 mg/dL (1.03 mmol/L) in males, <50 mg/dL (1.29 mmol/L) in females, or specific treatment for this lipid abnormality • Raised blood pressure: systolic blood pressure >130 mm Hg, diastolic blood pressure >85 mm Hg, or treatment of previously diagnosed hypertension • Raised fasting plasma glucose (FPG): >100 mg/dL (5.6 mmol/L) or previously diagnosed type 2 diabetes
Follow-up
Patients were subjected to periodic checks of their metabolic situation with visits at 7, 30, 60, and 90 days and 4, 5, 6, 9, and 12 months during the first year after surgery. The parameters analyzed were as follows: body composition measurements, weight, BMI, excess weight (%EW), %EW loss (%EWL), blood pressure, FPG, and lipid profile including total cholesterol, HDL, low-density lipoprotein, and triglycerides.
The remission of comorbidities was defined as the normalization of the parameters considered in the absence of drug therapy in place.
Statistical analysis
Data were analyzed with a statistical computer software (MedCalc version 12.2.1; MedCalc Software, Ostend, Belgium).
Patient characteristics were expressed as mean±SD values and medians for continuous data and as frequencies for categorical data. Student's t tests were used to compare data before and after surgery. A value of P<0.05 defined the results as statistically significant.
Results
Table 1 shows the characteristics of patients. All patients had morbid obesity with a mean BMI of 45.97±5.49 kg/m2. Fifteen patients had an FPG level >100 mg/dL or previously diagnosed type 2 diabetes mellitus, eight patients had hypertriglyceridemia (>150 mg/dL), fourteen patients had hypo-HDL cholesterolemia (<40 mg/dL), fifteen patients showed elevated systolic blood pressure (>130 mm Hg), and fourteen patients had elevated diastolic blood pressure (>85 mm Hg).
FPG, fasting plasma glucose; HDL, high-density lipoprotein; T2DM, type 2 diabetes mellitus.
Table 2 shows starting anthropometric and metabolic parameters. All surgical procedures were performed using the minimally invasive laparoscopic technique, and none of the interventions was converted to open surgery. Median operative time was 115 min (range, 75–130 min). No intraoperative complications occurred.
BMI, body mass index; DBP, diastolic blood pressure; EW, excess weight; HDL, high-density lipoprotein; SBP, systolic blood pressure.
Hospitalization was carried out regularly for all patients; the mean hospital stay was 6 days (range, 5–7 days). No major complications or postoperative reoperations occurred. A quick return to daily activities without any limitation was demonstrated in all patients, as shown through the Short Form-12 assessment scales, administered to the clinical control performed after surgery.
Table 3 summarizes the results of the main outcomes analyzed. The mean EWL% values were 8.57±3.02%, 17.65±6.40%, 25.47±7.90%, 33.76±9.27%, 41.83±10.71%, 46.02±13.90%, 52.60±14.05%, 58.48±16.07%, and 62.59±21.29% at 7, 30, 60, and 90 days and 4, 5, 6, 9, and 12 months, respectively. The respective mean BMI in the same observation interval was 43.92±5.08, 41.92±5.55, 40.11±5.56, 37.83±5.53, 35.74±5.47, 34.80±6.08, 32.93±5.68, 31.43±5.81, and 30.66±6.79 kg/m2.
P<0.05 compared with preoperative value.
BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; SBP, systolic blood pressure.
Figure 1 shows the significant difference in BMI between the preoperative values and those obtained at follow-up. In the same observational period there was an excellent improvement of metabolic parameters as shown in Figure 2.
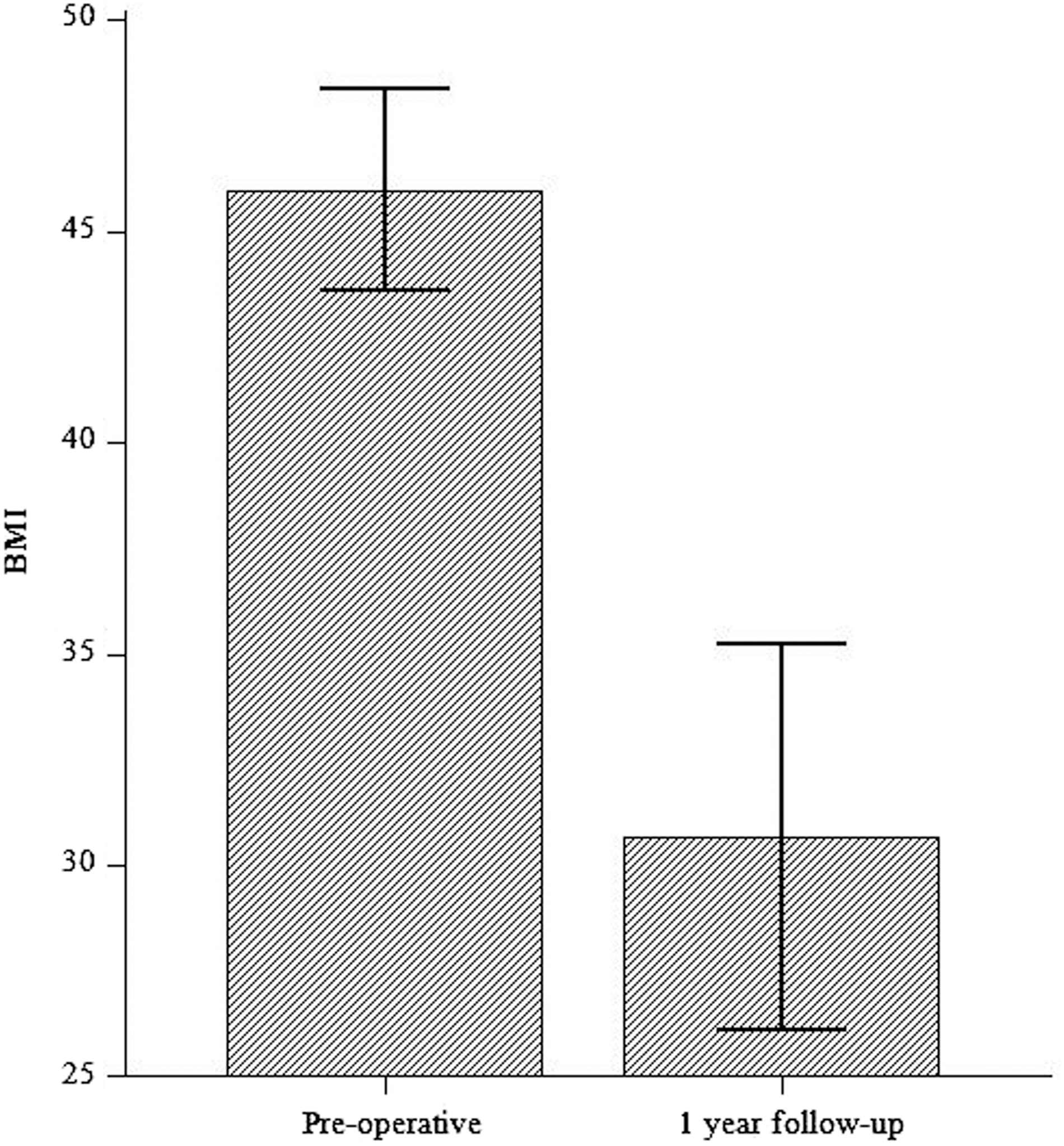
Comparison between preoperative body mass index (BMI) and BMI at 12 months after surgery.
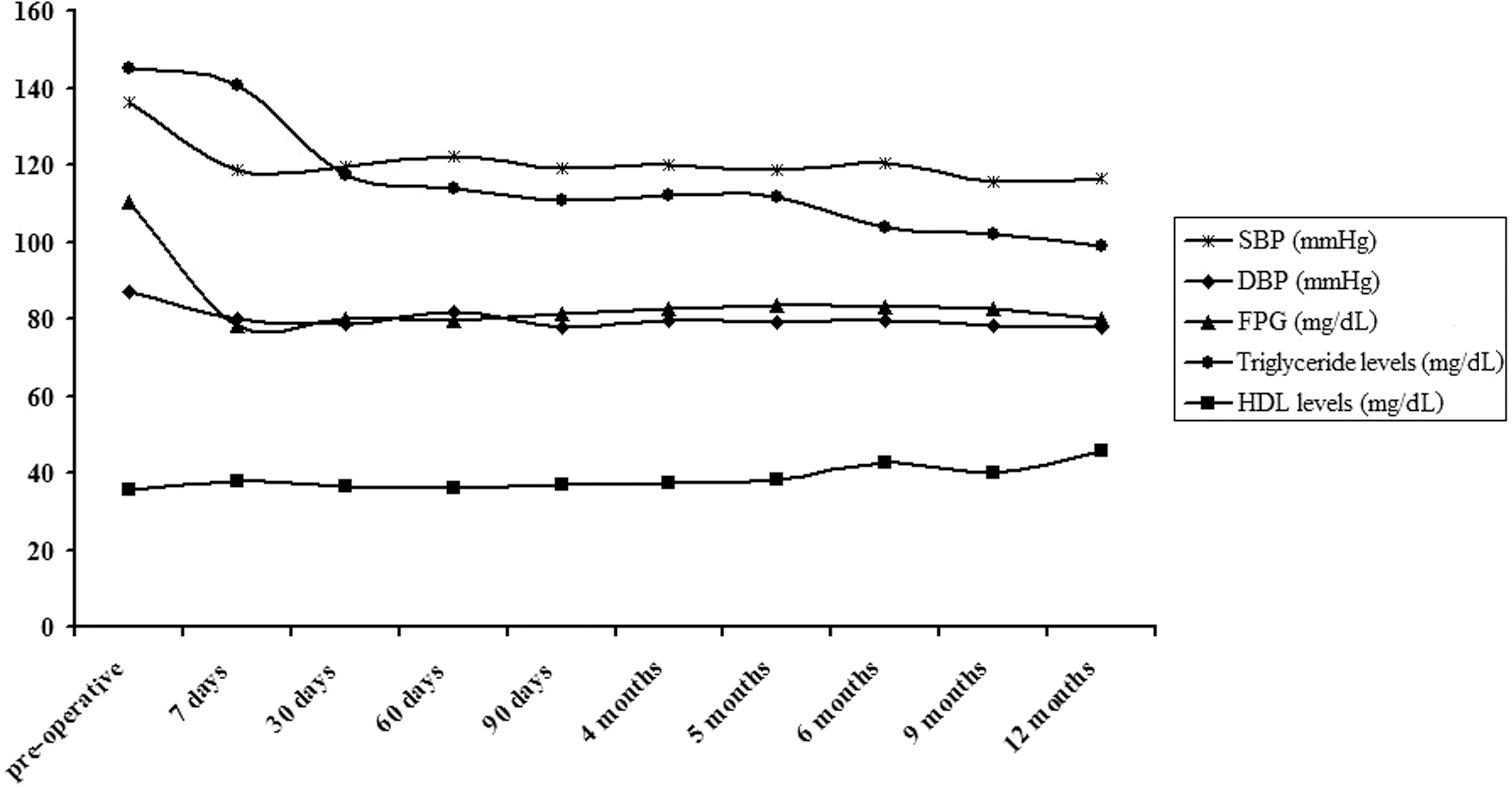
Evolution of the main outcomes at different periods after surgery during the follow-up: systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), triglycerides, and high-density lipoprotein (HDL).
None of the five patients previously taking prescribed hypoglycemic drugs restarted therapy, and mean FPG significantly decreased, since the first days after surgery, compared with the preoperative values.
Throughout the follow-up period, systolic and diastolic blood pressures showed a clear statistically significant improvement.
Five of nine patients, at an interval of 6 months after surgery, completely suspended the previously prescribed antihypertensive therapy with a good control of systolic and diastolic pressures. Four of nine patients reduced previously prescribed therapy by 30%.
In contrast, the modification in the lipid profile was much slower and more variable. During the observation period, triglyceride levels were significantly reduced since the fifth month after surgery.
Regarding HDL cholesterol, although there was a growing trend of the measured values, it did not reach statistically significance compared with the values before the LSG. The HDL cholesterol level values were higher by 40 mg/dL in 10 of 14 patients who showed these alterations before surgery. In contrast, six of nine patients with elevated levels of triglycerides had a significant reduction with values below 150 mg/dL at the end of the observation period.
Discussion
Obesity and its associated comorbidities are constantly increasing in Western populations and represent a major public health problem. The World Health Organization has defined obesity as a global epidemic and estimates that it affects at least 400 million adults (9.8% of the world's population). 10 The effects of this condition have a direct impact on the life expectancy of patients and their quality of life.
Surgical treatment in cases of morbid obesity constitutes the only remedy able to ensure an effective and lasting reduction in the weight and to improve or solve the pathologies responsible for the dramatic increase in related mortality. 11 Bariatric surgery procedures are divided into two categories: restrictive and malabsorptive. The former are based on the reduction of gastric capacity and on the emergence of an early sense of satiety with a consequent decrease in energy intake. On the other hand, the malabsorptive procedures ensure long-term weight loss due especially to malabsorption induced by intestinal bypass.
The LSG has been affirmed in the last few years. It was originally designed as the first phase of biliopancreatic diversion. This procedure has proved easy to implement through laparoscopy; it is safe and effective with a significant postoperative morbidity. For these reasons, it has spread rapidly around the world and has been approved by three International Consensus Summits. 12 –14 Currently, LSG is the most carried out procedure at our institute and has widespread consensus among patients.
Given the strong correlation between obesity and other metabolic disorders, weight loss has always been considered the first and only responsible factor for the resolution or improvement of comorbidities after surgery. This is based on evidence showing that the adipocytes secrete numerous biological constituents (leptin, tumor necrosis factor-TNF-α, free fatty acids, adiponectin) that modulate different hormone actions affecting insulin secretion and its effect that contributes to cause insulin resistance. However, in recent years, several clinical studies have shown resolution mechanisms of diabetes and other comorbidities beyond simple reduction of excessive body mass.
In particular, LSG does not only show restrictive action, but studies have highlighted its metabolic function. 15 –17 Following the intervention, there is a strong reduction of the level of ghrelin, which is produced mainly from the gastric fundus and is removed with the surgical procedure. This hormone inhibits insulin secretion and exerts diabetogenic effects. Furthermore, experimental studies 18,19 have shown that increased levels of glucagon-like peptide-1 and peptide YY are able to exert a trophic mechanism on the β-pancreatic cells by stimulating the biosynthesis of insulin. These effects may be at the basis of the improvement in the glucose metabolism indices shown in recent studies 20,21 and also observed in patients treated at our center. 17
Our data show a significant impact of LSG on weight loss in subjects with morbid obesity resulting in a mean EWL% of 62.59±21.29% at 1 year after surgery. In patients with diabetes and prediabetes, there has been a remission of the alteration observed in glycemic indices since the first postoperative period, remaining consistently below the pathological values for the entire period of the follow-up carried out so far.
Response to treatment was so effective that none of the patients previously taking hypoglycemic agents has continued prior therapy, and all 23 subjects followed up, in this study, achieved a constant reduction in FPG to <100 mg/dL.
The effects on the control of blood pressure (five patients completely discontinued therapy) and the HDL cholesterol values (there were no major changes in the patients) were more limited. Six of the nine patients with elevated triglyceride levels fell within the normal range.
Overall, during follow-up after LSG, 22 of the 23 (95.65%) patients studied no longer fell within the criteria defining the metabolic syndrome.
Conclusions
Currently there are few studies in literature regarding the role of LSG in treating both obesity and other associated diseases. Given the social importance of the topic and the significant results obtained in the case studies of other authors and in patients treated at our center, we believe randomized controlled trials and new evidence are needed. Metabolic syndrome is a complex of changes in the dynamic evolution of the organism that can lead to the progression of disease and, in the case of a correct medical management that must include the surgical treatment, may progress toward improving and, in some cases, the remission of the clinical picture.
Footnotes
Author Contributions
All authors contributed equally to this work and read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.