
Abstract
Objective:
This study was undertaken to investigate the effect of an insulin infusion site warming device, the InsuPatch40 ™ (IP40) (InsuLine Medical Ltd., Petach-Tikvah, Israel), on insulin aspart pharmacodynamics (PD) and pharmacokinetics (PK) in adolescents with type 1 diabetes.
Subjects and Methods:
Seventeen subjects with type 1 diabetes (age, 15±1 years; hemoglobin A1c, 7.5±0.2% [58±2.2 mmol/mol]) underwent two euglycemic clamps performed on separate mornings with and without IP40 activation with warming temperature at 40°C. On both days, the basal infusion was suspended, and glucose levels were maintained between 90 and 100 mg/dL by a variable rate dextrose infusion for up to 5 h after a 0.2 U/kg bolus of insulin aspart.
Results:
Time to peak insulin action and time to half-maximal action occurred earlier with a greater early glucodynamic effect (area under the curve [AUC] for glucose infusion rate from 0 to 30 min) with IP40 than without the IP40, whereas the AUC for the time–action profile and the peak action did not differ with and without infusion site warming. PK parameters were in agreement with PD parameters, namely, a significantly earlier time to reach the maximum increment in insulin concentrations and greater early bioavailability (AUC for the change in insulin concentration from 0 to 30 min) with the IP40. The tail of the plasma insulin response curve was also shortened with infusion site warming, with the time to reach baseline insulin concentration occurring significantly earlier (P=0.04).
Conclusions:
Our data demonstrate that skin warming around the infusion site to 40°C with the IP40 is an effective means to accelerate absorption and action of rapid-acting insulin. These improvements in time–action responses have the potential to enhance the performance of open- and closed-loop insulin delivery systems.
Introduction
T
Problems with the relatively slow time–action profiles of subcutaneously administered insulin analogs are exaggerated in closed-loop systems that use external insulin pumps owing, in part, to the delay between the start of the meal and increases in interstitial glucose concentrations that trigger automatic increases in insulin delivery, resulting in large postprandial glycemic excursions. Even more important, with closed-loop insulin delivery, is that the “meal bolus” is stretched out over more than 2 h as the algorithm responds to changes in interstitial glucose concentrations after a meal. 4 Thus, a major focus of current research in artificial pancreas development has been on methods to accelerate the absorption of insulin from the subcutaneous space.
It has long been known that increasing blood flow to an injection site by warming the skin increases the rate of insulin absorption. 5 –7 A novel insulin pump, an insulin infusion site warming device, the InsuPatch™ (InsuLine Medical Ltd., Petach-Tikvah, Israel), was designed on this principle. 8 We have recently shown that using this device to heat the skin surface to 38.5°C reduces the time to reach maximal action of a standard 0.2 U/kg bolus dose of insulin aspart from approximately 125 min to approximately 90 min in adolescents with type 1 diabetes. 1 The objective of this randomized, crossover study was to test the effect of this device at a higher temperature of 40°C because studies indicate that blood flow to the infusion site could be increased further by warming the skin to the higher temperature. 5 –7,9,10
Subjects and Methods
Subjects
The study was conducted in adolescents with type 1 diabetes who attended the Yale Children's Diabetes Clinic (New Haven, CT). Eligibility criteria included a clinical diagnosis of type 1 diabetes for ≥1 year, age between 12 and 18 years, continuous subcutaneous insulin infusion therapy for at least 3 months, hemoglobin A1c (HbA1c) <10.0% (86 mmol/mol), body mass index <95% for age and sex to eliminate the effect of insulin resistance due to obesity as a confounding factor, and the ability to comprehend written and spoken English. Subjects were excluded for any other medical disease aside from type 1 diabetes or for treated hypothyroidism, use of medications that might affect glycemic control, pregnancy or breast-feeding, not consistently using barrier methods or abstinence as contraception, or any other condition that in the judgment of the investigators would interfere with the subject's or parent's ability to provide informed consent or the investigator's ability to perform the study. The Yale University Human Investigation Committee approved the study.
At the initial enrollment visit, the risks and benefits of the study were explained. Informed consent was obtained from the parents or subjects who were 18 years of age, and informed assent was obtained from the subjects <18 years of age. History and physical examinations were performed, and the HbA1c level was measured.
InsuPatch at 40°C
In this device, the warming element is incorporated into the adhesive layer of the insulin infusion set and connected by wires to batteries that are carried in a modified insulin pump carrying case. The warming element contains a temperature sensor and controller unit that maintains the skin warming at a fixed temperature. In these experiments, the skin warming temperature was set at 40°C. When activated around the time of a bolus injection, the device applies controlled heat around the insulin infusion site that, in turn, increases blood flow into the area.
Procedures
Five-hour euglycemic clamps were conducted on two separate occasions for each subject separated by <8 weeks. One clamp was performed with the InsuPatch at 40°C (IP40) activated and the other without IP40 activation in random order, allowing the subjects to act as their own control. On each occasion, subjects were admitted on the afternoon prior to the euglycemic clamp procedure. A new insulin infusion set was inserted into the subcutaneous tissue of the anterior abdominal wall, and an intravenous catheter was placed for overnight blood sampling. Blood glucose levels were measured hourly during the night, and the basal insulin infusion was adjusted as needed to achieve glucose levels between 80 and 120 mg/dL at the start of the euglycemic clamp procedure the next morning.
All subjects fasted overnight and throughout the 5-h clamp study. A second intravenous catheter was placed on the contralateral arm for infusion of exogenous glucose on the morning of the clamp study; all subjects received insulin aspart at 0.2 U/kg of body of weight bolus with or without IP40 activation at the start of the study. During IP40 studies, IP40 was activated to warm the insulin infusion site for 15 min prior to the bolus and was kept on for 60 min after administration of the bolus. In all studies, the basal infusion of insulin via the insulin pump was suspended after the bolus was given.
A variable rate of 20% dextrose was infused and adjusted every 5 min based on bedside measurements of plasma glucose to maintain blood glucose levels from 90 to 100 mg/dL during the study for a period of 5 h. The serum insulin levels were measured by serum samples that were collected at 10-min intervals for the first 90 min, at 15-min intervals during 91–180 min, and then every 30 min during 181–300 min of the clamp study.
Biochemical methods
HbA1c was measured by the DCA Vantage® analyzer (Siemens Medical Equipment, Malvern, PA), plasma glucose by the YSI glucose analyzer (Yellow Springs Instrument Life Sciences Inc., Yellow Springs, OH), and plasma insulin by the Mercodia iso-insulin enzyme-linked immunosorbent assay test, with a reported cross-reactivity of 80% with insulin aspart (MercodiaAB, Uppsala, Sweden).
Statistical analyses
The exogenous glucose infusion rate (GIR) was analyzed every 10 min and adjusted for changes in the glucose space, as previously described.
11
The PD parameters that were calculated for each clamp study included the maximum glucose infusion rate (GIRmax), time to maximum glucose infusion rate (
Increments in plasma insulin levels measured from baseline at each time point throughout the clamp study were used for analysis to adjust for within subject differences in baseline insulin levels. Mean increment (Δ
Statistical comparisons were performed using GraphPad Prism® version 5.0 software (GraphPad Software Inc., La Jolla, CA). Paired t tests were used where applicable to compare plasma glucose level, insulin concentration, and glucose clamp data, which are reported as mean±SEM values.
Results
Seventeen of the 20 adolescents (six female, 14 male) who enrolled in the study completed both clamp studies. Two subjects were withdrawn from the study because they were started on medications that might affect metabolic responses between the first and the second clamp, and another patient who consented was subsequently withdrawn because of a history of polycystic ovary syndrome. The PK data were not available in one subject because of problems with processing samples for the insulin assay. Thus, data from 17 subjects were analyzed for the comparison of PD parameters, and data from 16 subjects were analyzed for PK measures. The mean age was 15±1 years, mean body mass index was 21±0.5 kg/m2, and mean HbA1c was 7.5±0.2% (58±2.2 mmol/mol). Mean plasma glucose concentrations did not differ between the two studies during the 5-h clamps (100±1 mg/dL with IP40 and 101±1 mg/dL without IP40, P=0.9).
As illustrated in Figure 1 and Table 1, IP40 activation shifted the time–action curve of insulin aspart to the left, with an earlier
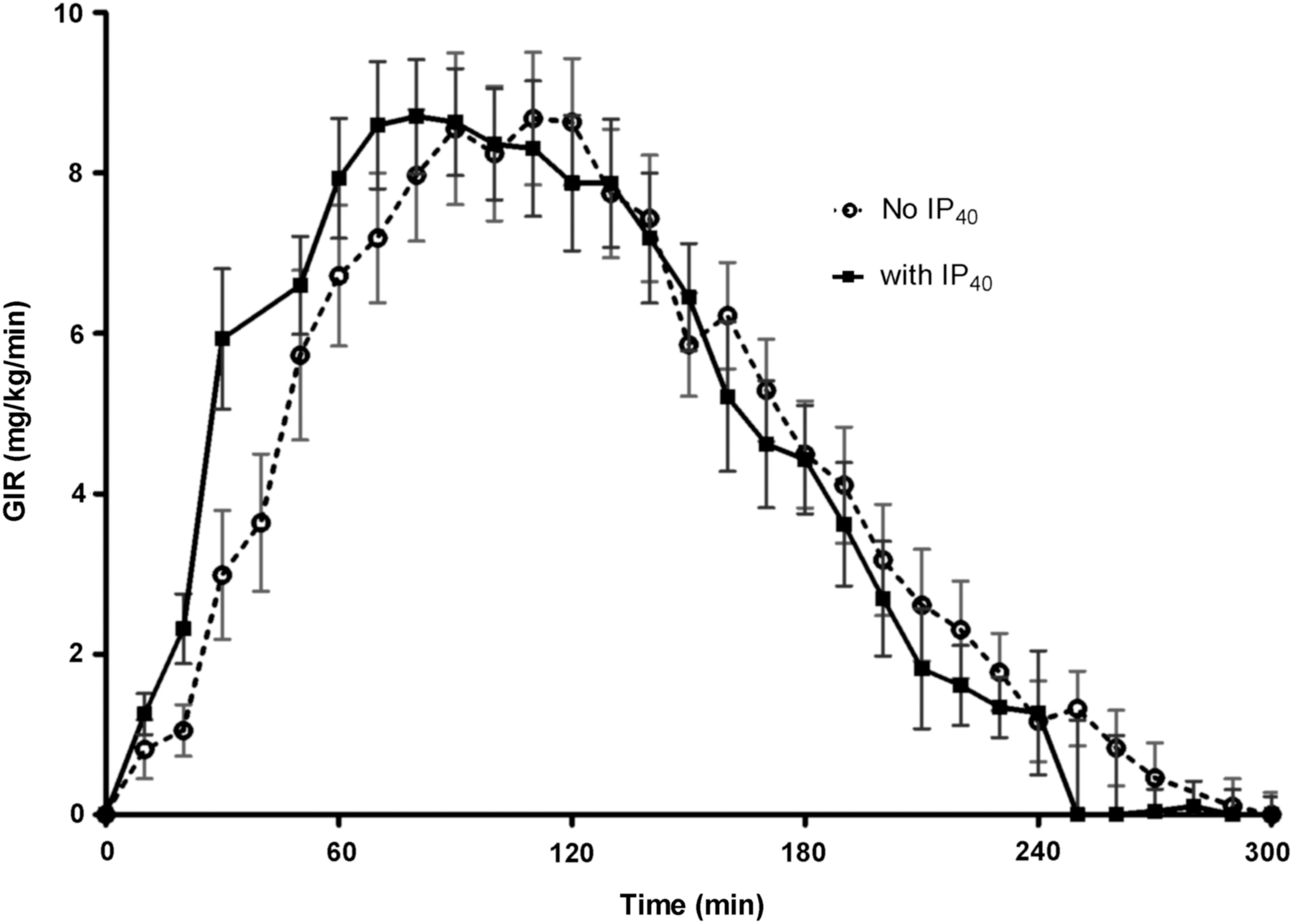
Average glucose infusion rate (GIR) values by time required to maintain euglycemia under glucose clamp conditions with (closed squares, solid line) and without (open circles, dotted line) activation of the InsuPatch at 40°C (IP40). Data are mean±SEM values.
Data are mean±SEM values. Plasma insulin concentrations as a measure of insulin pharmacokinetics are calculated as increments above baseline (Δ
AUC, area under the curve;
The mean baseline plasma insulin concentrations were similar between the two studies (27±3 μU/mL vs. 28±4 μU/mL with and without IP40, respectively, P=0.2). The increments in plasma insulin that were achieved after the 0.2 U/kg bolus of insulin aspart are shown in Figure 2. As shown in Table 1, the mean Δ
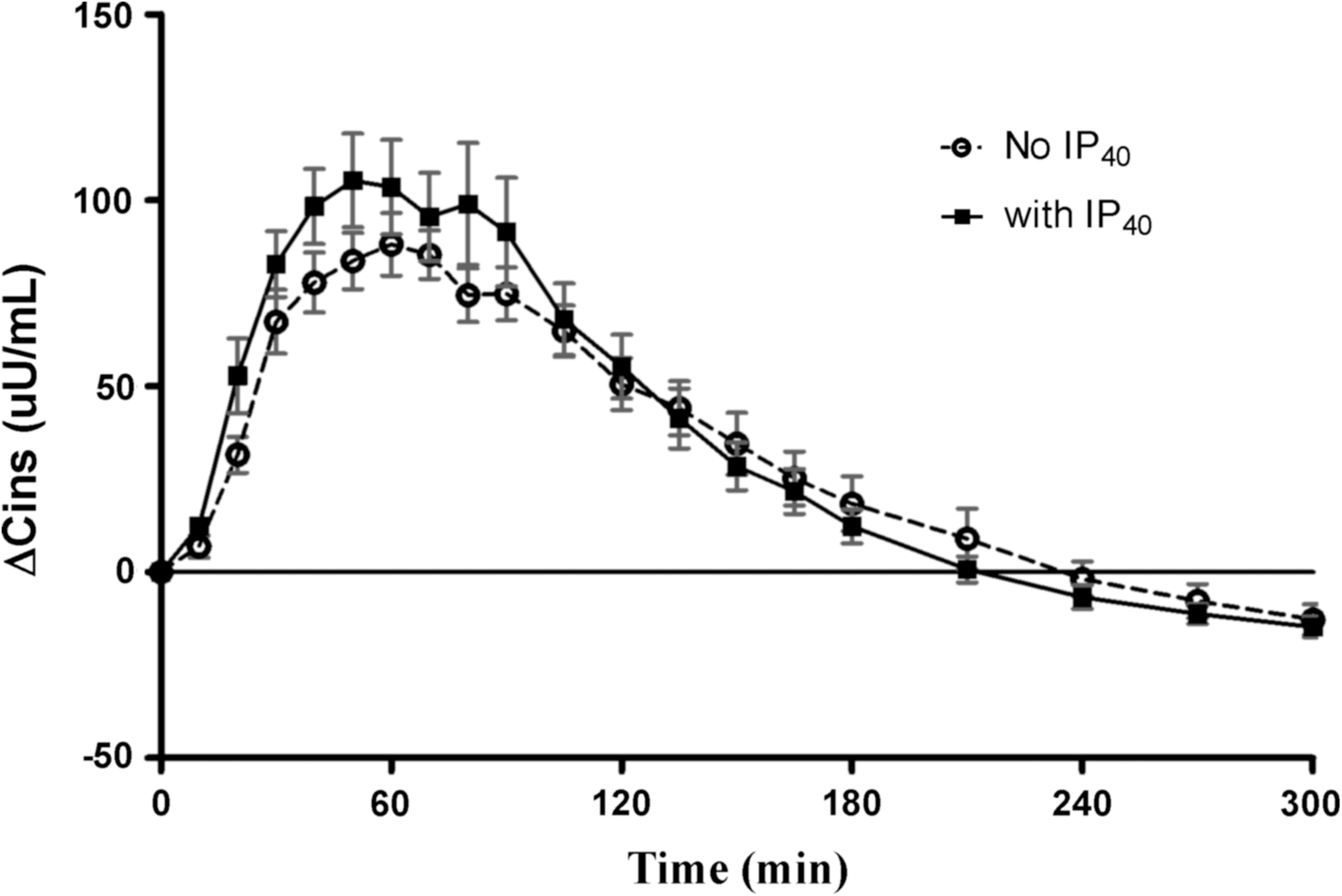
Increments in insulin plasma concentration (ΔCins) from baseline during euglycemic clamps with (squares) and without (circles) activation of the InsuPatch at 40°C (IP40) following bolus administration of insulin aspart at 0.2 U/kg. Data are mean±SEM values.
Discussion
Our previous study established that warming the skin surface around an insulin infusion set to 38.5°C with the InsuPatch (IP38.5) was effective in accelerating the time–action profile of a standard bolus dose of insulin aspart.
1
This finding was confirmed and extended in the present study with the use of IP40. As expected, in comparison with control studies without site warming, IP40 resulted in a much faster absorption and action of the insulin aspart bolus, especially during the first 30 min following administration. Moreover, the
It is particularly noteworthy that the PK analyses demonstrated that skin warming with the IP40 promoted more rapid elimination of the rapid-acting insulin bolus from the circulation. Despite higher peak increments in plasma insulin levels with infusion site warming, plasma insulin concentrations returned to baseline values significantly earlier during IP40 active clamp studies, an outcome that we had not observed in our previous IP38.5 study. 1 Accelerating the disappearance of the insulin bolus has been an important aim for ultra-fast-acting insulin development because it offers a means to reduce the risk of late postprandial hypoglycemia, especially after the last meal of the day.
We took a conservative approach in our first study by warming the skin to only 38.5°C because this might increase battery life in future clinical use devices, even though warming the skin to 40°C has been shown to enhance the magnitude of increase in local blood flow compared with the lower temperature.
7,10
We anticipated that skin warming to 40°C would be well tolerated by the patients because devices that warm the skin surface to 42°C have been approved by the Food and Drug Administration. Moreover, previously published studies investigating temperature threshold for skin burn injury have shown that no signs of thermal injury were observed when skin was exposed to temperatures up to 43°C for a prolonged period of time.
12
–15
The concern that skin warming might reduce the bioavailability of the insulin bolus by denaturing some of the insulin in the subcutaneous depot was not supported by our findings: overall PK (mean Δ
There are a few limitations of this study. The study was nonblinded for both the investigator and the subject for practicality. The dose of insulin for our study was 0.2 U/kg for all subjects, and even though variability in PK/PD depending on insulin dose has been shown for regular insulin, it is possible that the acceleration of insulin action could vary based on the amount of insulin dose delivered, with possibly even faster action for lower insulin doses. 2,3,16 We excluded subjects with potential insulin resistance due to obesity and polycystic ovary disease to limit confounding factors for insulin action. 17,18 The negative impact of adiposity to insulin absorption could have been an additional confounding factor as shown in tracer absorption studies performed in subjects without diabetes using regular insulin. 19
The effectiveness of IP40 compares very favorably with other approaches aimed at increasing the rate of absorption and action of subcutaneously injected insulin. Changing the excipients that are used to keep insulin in solution has been successful in accelerating the rate of absorption of regular human insulin and insulin aspart, as has pretreating the infusion site with recombinant human hyaluronidase to break down barriers to fluid dispersion in the subcutaneous space. 20 –23 Alternative insulin delivery methods such as inhaled insulin and intradermal delivery with microneedles have been shown to confer ultra-fast-acting profiles during meal and insulin clamp studies. 24 –26 Further studies are needed to determine whether the time–action profiles of rapid-acting insulin analogs can be accelerated even more by combining site warming with one or another of these alternative approaches.
Conclusions
The infusion site warming appears to be a well-tolerated, safe, and effective method to speed the absorption of subcutaneous insulin boluses, with potential for use in both open- and closed-loop insulin delivery.
Footnotes
Acknowledgments
This work was made possible by grants from the JDRF (JDRF 17-2010-426) and the National Institutes of Health Clinical and Translational Science Award (TR000142) that supported the staff of the Yale-New Haven Hospital Research Unit. We thank Yale Pediatric Diabetes Clinic & Research Center Team members, our patients, and their families.
Author Disclosure Statement
W.V.T. is a consultant for Medtronic Diabetes, Novo Nordisk, Sanofi, Unomedical, and Insuline Medical. S.A.W. is a consultant for Animas, Becton Dickinson, and Insuline Medical, has received in-kind grant support from Medtronic, and serves as a speaker for Eli Lilly. E.C., J.L.S., E.M.T., D.C., A.S., and L.C. have no disclosures.