
Abstract
Background:
The ASPIRE in-clinic study established that automatic suspension of insulin with the threshold suspend (TS) feature reduces the duration of induced hypoglycemia. The study's crossover design allowed the effects of antecedent hypoglycemia to be studied.
Subjects and Methods:
The study enrolled 50 subjects who exercised until plasma glucose (YSI glucose and lactate analyzer; YSI, Inc., Yellow Springs, OH) reached ≤85 mg/dL. Hypoglycemia was evaluated after the YSI value reached <70 mg/dL. In TS experiments, insulin was stopped for 2 h once a sensor glucose (SG) value of ≤70 mg/dL was detected; in control experiments, basal insulin delivery continued. Subjects were randomly assigned to Group A (TS in Period 1; control in Period 2) or Group B (control in Period 1; TS in Period 2). Experiments were separated by 3–10 days.
Results:
Hypoglycemia was 63.7 min shorter in Period 1 TS experiments (no preceding control experiment) than in Period 2 TS experiments (one or more preceding control experiment(s)) (P<0.01). The number of experiments prior to a successful TS experiment was lower for Period 1 than for Period 2 (0.36±0.64 vs. 1.57±0.84; P<0.001), as was the cumulative duration of antecedent hypoglycemia (16.6 min vs. 204.6 min; P<0.001). The between-groups difference in hypoglycemia duration was not attributable to differences in SG rates of change, the duration of exercise, or area under the curve of <70 mg/dL×min in the 2 days before the successful experiment (all P>0.3).
Conclusions:
The TS feature's ability to mitigate hypoglycemia was decreased by an episode or episodes of prolonged antecedent hypoglycemia, suggesting hypoglycemia begets hypoglycemia. The effect of antecedent hypoglycemia should be taken into consideration in the design of future experiments assessing strategies to reduce hypoglycemia.
Introduction
S
In the ASPIRE in-clinic study, 3 we examined the glycemic response to overnight fasting and exercise in adults with type 1 diabetes and compared the effects of continued basal insulin delivery with the effects of automatic insulin pump suspension triggered at a preset sensor threshold (threshold suspend [TS], formerly known as low glucose suspend). As expected, hypoglycemia was attenuated in the experiments that included automatic pump suspension (TS experiments) compared with experiments with continued basal insulin delivery (control experiments). 4 Specifically, the TS feature was found to reduce the duration of hypoglycemia (138.5±76.68 min vs. 170.7±75.91 min in TS vs. control experiments, respectively; P=0.006) and its severity (mean nadir glucose, 59.5±5.72 vs. 57.6±5.69 mg/dL in TS vs. control experiments; P=0.015). 4 In addition, the risk of subsequent rebound hyperglycemia after the 2-h pump suspension was found to be low.
Because of the ASPIRE in-clinic study's crossover design, subjects participated in at least two hypoglycemic induction experiments that were separated by 3–10 days. The a priori study design included evaluating the order effect on duration and severity of hypoglycemia. It was found that the duration of hypoglycemia in initial TS experiments was significantly shorter than those in second or subsequent TS experiments. The factors contributing to the order effect on hypoglycemia duration were evaluated and are reported in this manuscript. Preliminary results have been presented at the 72nd Scientific Sessions of the American Diabetes Association. 5,6
Study Design and Methods
The design and methods of the ASPIRE in-clinic study are described elsewhere. 3 A history of hypoglycemic seizure or hypoglycemic coma within the last 2 years was an exclusion criterion. The protocol required that subjects were to have been diagnosed with type 1 diabetes and that they had at least 3 months of experience with a Medtronic (Northridge, CA) insulin pump; subjects were required to use Veo™ pumps and wear Sof-sensor® glucose sensors throughout the study. The experiments to induce hypoglycemia were to involve repeated exercise sessions until the YSI glucose value (measured with the YSI 2300 STAT Plus™ glucose and lactate analyzer [YSI, Inc., Yellow Springs, OH]) reached ≤85 mg/dL, a rest period until the YSI glucose value reached <70 mg/dL, and an observation period. In the postexercise observation period, the protocol required the level glucose to be measured via the YSI analyzer every 5–15 min to calculate duration and nadir between 50 and 70 mg/dL. The pump was to be set to suspend insulin delivery for 2 h at a sensor glucose (SG) value of ≤70 mg/dL in TS experiments or to deliver basal insulin regardless of the SG value in control experiments. Subjects were to be randomly assigned to Group A (TS experiments in Period 1, followed by control experiments in Period 2) or Group B (control experiments in Period 1, followed by TS experiments in Period 2).
The protocol required the duration and severity of hypoglycemia to be quantified in frequently drawn plasma samples with the YSI 2300 STAT Plus analyzer. Hypoglycemia duration was defined as the length of time that YSI values were <70 and >50 mg/dL; hypoglycemia severity was defined as the lowest observed YSI value. Experiments were abandoned in the interest of patient safety if the YSI value fell below 50 mg/dL or exceeded 300 mg/dL; data from such experiments were not analyzed. The primary end point was a comparison of the duration and severity of hypoglycemia measured with the YSI analyzer during successful TS and control experiments. The effect of the order of TS and control experiments was deemed significant for P≤0.1. If this order effect criterion was met, pre- and post-crossover sessions were to be analyzed separately. The two-sample t test was used to compare attributes of successful experiments between periods. Efficacy of the TS feature was defined as a reduction in either duration or severity of hypoglycemia at the 0.0154 level of significance.
Results
The glycated hemoglobin (A1C) level (mean±SD) of all 50 subjects was 7.9±0.6%. Comparison of the 48 successful TS Period 1 experiments (which, by design, were not preceded by any control experiments but might have been preceded by an experiment that had been terminated early because of a YSI value of <50 mg/dL or patient issues) with the 50 successful TS Period 2 experiments (which were preceded by one or more control experiments) showed that the duration of hypoglycemia was 63.7 min shorter in Period 1 than in Period 2 (107.8±71.2 min in Period 1 versus 171.5±67.0 min in Period 2; P<0.01).
Additional analysis was performed to assess the order effect. Table 1 shows the cumulative duration of antecedent hypoglycemia was also significantly less prior to Period 1 TS experiments than prior to Period 2 TS experiments (16.6 min vs. 204.6 min; P<0.001). In addition, there were significantly fewer induction experiments prior to the Period 1 experiments than prior to the Period 2 experiments (0.36±0.64 vs. 1.57±0.84; P<0.001). However, the order effect did not appear to be attributable to differences in YSI rates of change, the duration of exercise, or area under the curve (AUC) of <70 mg/dL×min in the 2 days before the successful experiment (all P>0.9). Table 2 shows the disposition of all attempted and failed experiments.
Data are mean±SD values. P values refer to Period 1 versus Period 2 comparisons.
Total time spent with YSI values between 50 and 70 mg/dL in previous successful and unsuccessful experiments.
Number of previous successful and unsuccessful experiments.
Largest negative rate of change of YSI glucose readings on the day of the experiment.
Time from the initiation of exercise to the first YSI value≤85 mg/dL.
AUC, area under the curve; CGM, continuous glucose monitoring; TS, threshold suspend.
Values represent the total for Period 1 and Period 2 experiments, followed in parentheses by the number of experiments or subjects in each individual period.
TS, threshold suspend.
Figure 1 shows the order effect by plotting mean YSI values at various times after hypoglycemia was achieved. In TS Period 1 experiments, YSI values returned to the normal range faster than in TS Period 2 experiments. YSI values in TS Period 1 experiments were consistently higher than YSI values from TS Period 2 experiments. The mean glucose values in control experiments remained in the hypoglycemic range for the entire 4-h observation period and were similar in Periods 1 and 2.

Mean (±SEM) YSI glucose values during hypoglycemia induction experiments: solid lines, Period 1; dashed lines, Period 2; triangles, threshold suspend (TS); and circles, control. Time 0 represents the time when the YSI glucose value fell below 70 mg/dL.
Figure 2 shows the percentage of subjects with YSI values in the hypoglycemic range (50–70 mg/dL) at various times after the start of hypoglycemia in Period 1 and Period 2 experiments. There was an early (within 60 min) decrease in the percentage of subjects who remained hypoglycemic in TS Period 1 experiments; this low percentage of hypoglycemic subjects was maintained throughout the observation period (Fig. 2A). This is in contrast to TS Period 2 experiments, where most patients experienced >120 min of hypoglycemia and approximately 50% of patients were hypoglycemic at the end of the observation period (Fig. 2B). In control experiments in both Period 1 and Period 2, most subjects' YSI values were in the hypoglycemic range for the entire observation period. No serious adverse events occurred, as reported previously. 4
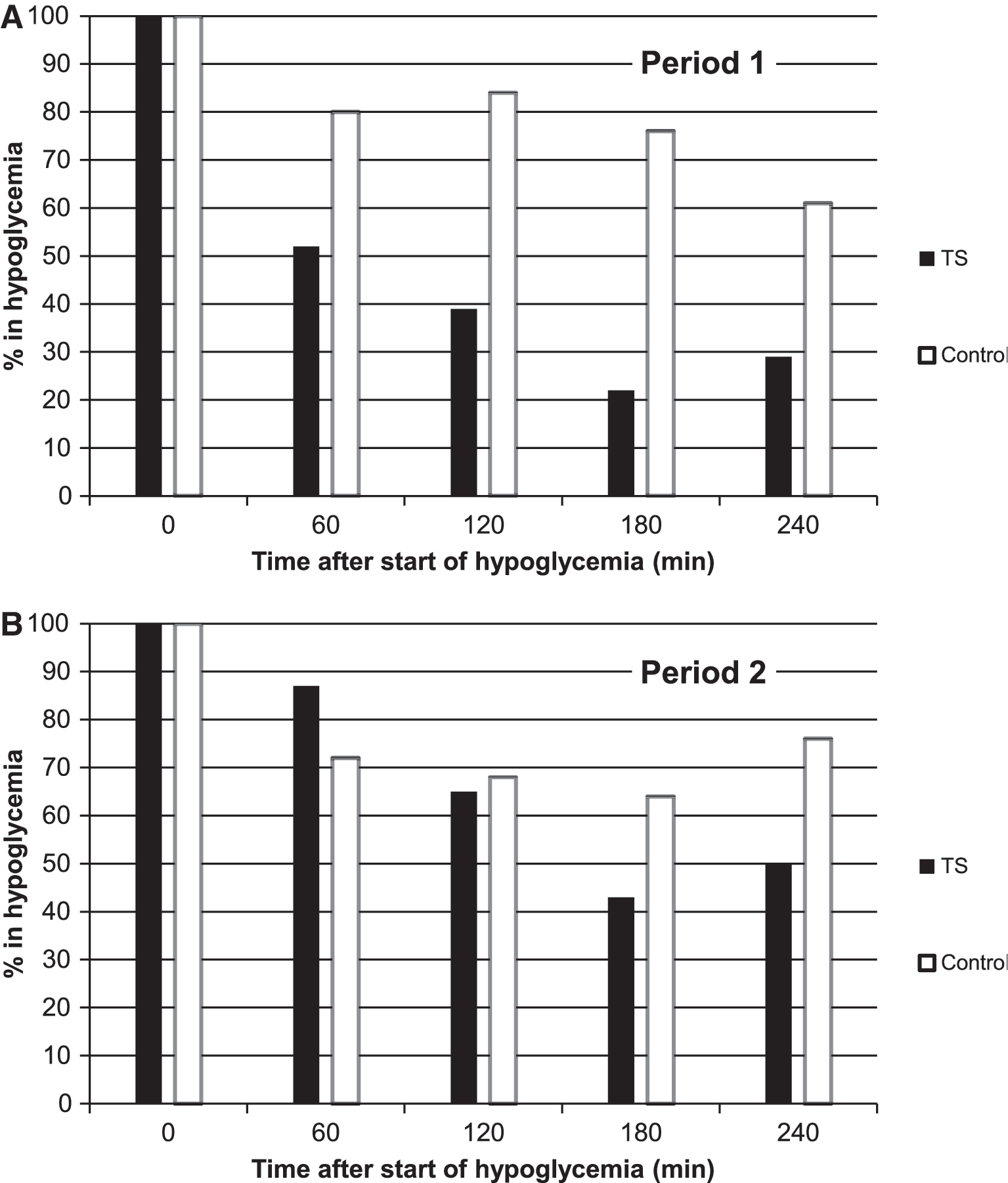
Percentage of subjects in hypoglycemia (YSI glucose value of 50–70 mg/dL) at various times after the start of a hypoglycemia episode in
Discussion
Several studies of the TS feature have now been reported. These have shown a reduction in the duration of hypoglycemia in children 7 and in the overnight hours among those at greatest risk. 8 Analysis of pump suspensions lasting for 2 h (the maximum allowed by the Veo pump) showed that they do not result in severe hypoglycemia, 9,10 and regular use of the TS feature was associated with reductions in the number and severity of severe hyperglycemic episodes. 10 In a randomized controlled trial, use of the TS feature over a 3-month period in the home setting was shown to significantly reduce the mean AUC of nocturnal hypoglycemic events, as well as the weekly rate of those events, without significantly changing A1C levels. 11
The ASPIRE in-clinic study's crossover design allowed comparison of subjects' recovery from hypoglycemia under various conditions and showed that recent hypoglycemia is detrimental to recovery from subsequent hypoglycemia. The effect was only apparent in experiments that stopped insulin delivery (i.e., the TS experiments), where spontaneous recovery from exercise-induced hypoglycemia was possible. In TS Period 1 experiments, with no recent exposure to severe and prolonged hypoglycemia, this recovery was significantly faster than the recovery in TS Period 2 experiments, where subjects had been exposed to recent episode(s) of severe and prolonged hypoglycemia. This suggests that one or more mechanisms for glucose homeostasis remained impaired when Period 2 TS experiments were initiated.
In TS Period 1 experiments, subjects' recovery from hypoglycemia at 60 and 180 min might represent the decay of insulin from the subcutaneous depot (at rates that are dependent on individual factors), combined with rapid increases in glycogenolysis and later increases in gluconeogenesis. In TS Period 2 experiments, the relatively protracted hypoglycemia may be due to more glycogen depletion from the prior hypoglycemic episode(s), which we would expect to have been further depleted in the recovery phase. Impaired autonomic responses to prolonged hypoglycemia may also have played a role in TS Period 2 experiments (not evaluated in this study).
When basal insulin delivery continued throughout the hypoglycemic episode (i.e., the control experiments), no detrimental effect of antecedent hypoglycemia was seen. This ability of continued basal insulin delivery to impair recovery from hypoglycemia may be due to its ability, at physiological concentrations, to suppress gluconeogenesis by approximately 20% and to completely block glycogenolysis, 12 combined with its activation of glycolysis and glycogenesis.
When basal insulin delivery is suspended during hypoglycemia, the liver and sympathoadrenal system play critical roles in the timing and magnitude of recovery, and a detailed mathematical model of hepatic glucose metabolism 13 suggests a multifaceted etiology for the order effect. Early in hypoglycemia, glycogenolysis predominates; with time, glycogen stores are depleted, and the relative contribution of gluconeogenesis to overall hepatic glucose production increases. In Period 2 TS experiments, the modest decrease in the percentage of subjects in hypoglycemia at 60 min may be attributable to a relative lack of glycogen, and the recovery of subjects after 60 min may be attributable to increased rates of gluconeogenesis (Fig. 2). The order effect may also be due to other effects of exercise that can significantly modify the metabolic and endocrine responses to subsequent exercise. 14 Antecedent hypoglycemia is known to attenuate the sympathoadrenal and symptomatic responses to hypoglycemia, 15 which may further contribute to the observed order effect.
This analysis of the ASPIRE in-clinic study has several limitations, including that it did not measure or attempt to control for the fitness of the participants, caloric expenditures, or counterregulatory hormones. In addition, a wide range of between-experiment intervals (3–10 days) was allowed, and the time between experiments was not adjusted for the duration or extent of prior hypoglycemic exposure. The 50 mg/dL glucose threshold at which experiments were halted helped to ensure patient safety but limited the study's ability to resolve potential differences in hypoglycemia severity; the observed difference in nadir glucose values of approximately 2 mg/dL is likely not clinically significant. The rate of failed experiments (36 out of 134 attempts) attests to the difficulty of achieving and maintaining hypoglycemia in subjects in the absence of carbohydrate administration or alterations in preprogrammed insulin delivery. The mean and median sensor bias values in the 40–70 mg/dL range were 6.3±13.3 mg/dL and 7.7 mg/dL, respectively. Although this positive bias may have triggered the pump to suspend at reference glucose values higher than 70 mg/dL and sensor heterogeneity may have contributed to differences in the severity and/or duration of induced hypoglycemia episodes, no attempt was made to relate the performance characteristics of individual sensors to the outcomes of individual experiments.
Scrupulous avoidance of hypoglycemia is critical to breaking the cycle of HAAF. 2 The value of the automatic pump stoppage feature therefore includes not just acute mitigation of hypoglycemia, but also preservation of the normal autonomic response to existing or impending hypoglycemia. Complete reversal of HAAF is difficult to predict or establish, but sustained euglycemia is now a reasonable goal for many people with type 1 diabetes. We anticipate that improvements in closed-loop insulin delivery systems will help more people reach this goal.
Conclusions
Prolonged hypoglycemia was induced by overnight fasting, exercise, and continued basal insulin delivery in the ASPIRE in-clinic study, regardless of prior exposure to hypoglycemia. Automatic insulin pump suspension triggered by low sensor glucose concentrations significantly reduced the duration and severity of hypoglycemia. Because this effect was attenuated in subjects with recent hypoglycemia, we conclude that recent hypoglycemia is a risk factor for prolonged hypoglycemic episodes—that “hypoglycemia begets hypoglycemia.” 16 This effect was not due to the duration of exercise, the rate of change of glucose concentration, or spontaneous exposure to hypoglycemia during the preceding 2 days. By mitigating the duration of hypoglycemic episodes, automatic pump suspension may help to preserve the normal autonomic response to hypoglycemia in patients with type 1 diabetes.
In future experiments or clinical trials of hypoglycemia, our observations suggest that the crossover design should be used with caution, if at all, and that avoidance of hypoglycemia for more than 10 days may be necessary to allow for near-normal responses to hypoglycemia.
Footnotes
Acknowledgments
The authors thank Scott W. Lee, MD, an employee of Medtronic, Inc., for comments on an earlier draft of this manuscript, and the subjects who participated in the study. This research was funded by Medtronic, Inc.
Author Disclosure Statement
J.S., J.B.W., and F.R.K. are employees of Medtronic, Inc. S.K.G., R.L.B., T.S.B., B.A.B., R.H.S., and D.C.K. have received research support from Medtronic, Inc. D.C.K. is a consultant to Google, Insuline, Voluntis, and Sanofi. No other potential conflicts of interest relative to this article were reported.