
Abstract
Background:
Insulin resistance (IR) precedes type 2 diabetes, but tests used to detect it in clinical settings reported poor reproducibility. We assessed the reliability of the [13C]glucose breath test (13C-GBT) in a sample of subjects without diabetes. Repeatability of the test was compared with that of other IR surrogates derived from the fasting or oral glucose tolerance test (OGTT).
Subjects and Methods:
Eighty-six healthy volunteers received an oral load of 75 g of glucose in 150 mL of water followed by 1.5 mg/kg of [U-13C]glucose in 50 mL of water. Breath and blood samples were collected at baseline and at 10, 20, 30, 60, 90, 120, 150, and 180 min following the glucose load; the same procedure was repeated within 1 week. The enrichment of breath 13CO2 was measured by ratio mass spectrometry and expressed as percentage oxidized dose at a given time period. Intrasubject variability was assessed with Bland–Altman plots and coefficients of variation (CVs).
Results:
The overall CV of the 13C-GBT was 12.99±11.61%, compared with 18.42% of fasting insulin, 19.44% for homeostasis model assessment, 17.06% of the composite insulin sensitivity index, and 29.99% for insulin in the 2-h oral glucose tolerance test. The variability of the 13C-GBT tended to be higher in lean (17.40%) than in overweight (10.17%) and obese (12.61%) individuals.
Conclusions:
The variability of the 13C-GBT is lower than that of other IR surrogates, making it a reproducible method to estimate insulin sensitivity in overweight and obese adults without diabetes. Because the individuals did not have diabetes but were within a high range of insulin sensitivity, the test should have application in clinical and population-based studies, given the evidence for the utility and limitations of this surrogate.
Introduction
T
Because IR is the inverse of insulin sensitivity, the gold standard to identify it is the hyperinsulinemic-euglycemic clamp, which provides the most direct measurement of tissue insulin sensitivity. 10 However, this is an invasive, expensive, and time-consuming procedure, which is difficult to use in routine clinical practice or in large epidemiological studies. 11 Many attempts are being made to successfully identify IR using surrogate measurements. The simplest are those derived from fasting insulin and glucose determinations, such as the homeostasis model assessment (HOMA) index. 12 Other IR indexes developed from glucose and insulin concentrations obtained during an oral glucose tolerance test (OGTT), such as the 2-h insulin level after the glucose load, and the Matsuda–DeFronzo insulin sensitivity index (ISI-Composite) have demonstrated a strong correlation with the glucose clamp technique. 13,14 However, one major disadvantage of these methods is their poor reproducibility, 15 –18 making evident the need to develop less complex and less invasive but dependable tools to measure IR.
The [13C]glucose breath test (13C-GBT) is a noninvasive technique that has been proposed to measure glucose metabolism. The test is based on the assumption that ingestion of isotopically labeled glucose ([U-13C]glucose) results in the expiration of labeled CO2 (13CO2), which can be measured in breath. Breath 13CO2 abundance derives almost totally from [U-13C]glucose metabolism and represents an indirect measurement of glucose oxidation via the Krebs cycle. 19 Such abundance is blunted in T2DM and likely in other IR status. Recently, Lewanczuk et al. 19 reported that a 13C-GBT with 15 g of dextrose and 25 mg of [U-13C]glucose is effective to assess insulin sensitivity in T2DM and obese individuals (r=0.69 with clamp). Also, Dillion et al. 20 found that a 13C-GBT with 75 g of glucose and 150 mg of [U-13C]glucose was useful to recognize individuals with early-stage diabetes and prediabetes. However, although the validity of the 13C-GBT to identify T2DM individuals has been demonstrated, its reliability to identify IR in subjects without diabetes has not been established. In this regard, Singal et al. 21 reported that breath test–derived measurements from a sample of 20 lean, obese, or T2DM subjects exhibited lower within-subject variability than the 2-h glucose concentration obtained from an OGTT. In addition to the small sample size, the 2-h glucose level is a measurement of impaired glucose tolerance (IGT) instead of IR.
Therefore, the aim of our study was to establish the reliability of the 13C-GBT in a sample of subjects without diabetes within a wide range of body mass index (BMI) values and to compare the test variability with those of other IR surrogates derived from fasting and from an OGTT.
Research Design and Methods
The study was conducted in the Unit of Research in Medical Nutrition of the Mexican Institute of Social Security in Mexico City, Mexico. The protocol was approved (protocol number R-2007-3603-18) by the Ethics Committee of this Institute. Eighty-six volunteers were recruited on the likelihood that they would represent a wide spectrum of insulin sensitivity. For this, subjects were within a wide range of BMI values but were healthy otherwise. Individuals whose capillary blood glucose level was ≥126 mg/dL at entering (OneTouch® Ultra® glucometer; LifeScan, Inc., Milpitas, CA) were excluded. The study protocol included 2 days of activities separated from one another by no more than 1 week.
Study procedures
On the first day of the study (Test 1), subjects arrived at 8:00 a.m. after a 10–12-h fast and received a 75-g oral load of glucose (ACS reagent; Sigma-Aldrich, St. Louis, MO) in 150 mL of water, followed by 1.5 mg of [U-13C]glucose/kg of body weight (Cambridge Isotope Laboratories, Inc., Andover, MA) dissolved in 50 mL of water. Blood and breath samples were obtained at baseline and at 10, 20, 30, 60, 90, 120, 150, and 180 min following the glucose load. Breath samples were collected in Exetainer® test tubes (Labco Ltd., High Wycombe, UK) with a common straw. Blood samples were collected via an antecubital venous catheter. The same procedures were repeated within 1 week (Test 2). During Test 1 and Test 2, subjects were allowed activities such as watching TV, reading, or using a computer. The 13C-GBT was repeated in the 86 subjects for Test 2; only 27 individuals accepted blood sampling for OGTT-derived measurements for the second test.
Biochemical determinations and calculations
The plasma glucose level was determined by an enzymatic method (YSI 2300 Stat Plus™ glucose analyzer; YSI Inc., Yellow Springs, OH), and the plasma insulin level was determined by radioimmunoassay using commercial kits (Millipore, Billerica, MA). The coefficients of variation (CVs) for glucose and insulin were 3.9% and 7.5%, respectively.
To estimate IR surrogates the following equations were used
14
:
Breath CO2-derived measurements
13CO2 in breath samples were measured with an isotope ratio mass spectrometer (Finnigan Breath Mat Plus; Thermo Finnigan MAT GmbH, Bremen, Germany) with a CV of <1% and expressed as percentage oxidized dose at a given time period. Raw 13C/12C data were expressed as delta per mille versus the Pee Dee Belemnite standard (δ13 PDB) and transformed to percentage of oxidized dose. For calculations the formulas previously described by Braden et al. 22 were used.
Statistical methods
For statistical analysis SPSS software was used (version 19; SPSS Inc., Chicago, IL). Data were expressed as mean±SD values. Intrasubject variability was assessed with CVs and Bland–Altman plots. CVs for each individual observation, between Test 1 and Test 2, were computed as (SD/mean)×100; then the mean values for each surrogate were calculated. One-way analysis of variance with Dunnett's post hoc test was used to compare the CVs of each IR surrogate using the 13C-GBT as the control. For Bland–Altman plots, the mean discrepancy ratio was estimated as follows: (difference between tests/overall mean)×100. Bland–Altman limits of agreement with a 95% confidence interval were calculated with the following formula: (mean discrepancy±1.96)×(SD of discrepancies). Bivariate correlations between 13C-GBTand other IR surrogates were conducted with Pearson analysis.
Results
13C-GBT, fasting insulin, and HOMA were measured in 86 healthy subjects in two consecutive times within a period of 5.7±2.2 days. Participants were 21–65 years old, 36% were males, and BMI ranged from 19.56 to 46.66 kg/m2. According to BMI, 29.1% were lean (BMI<25 kg/m2), 37.2% overweight (BMI from ≥25 kg/m2 to <30 kg/m2), and 33.7% obese (BMI≥30 kg/m2). OGTT and derived indices were repeated only in a subset of 27 individuals. General characteristics and IR surrogates at baseline are presented stratified by nutritional status in Table 1. As denoted by HOMA, patients were within a wide spectrum of insulin sensitivity, and 53.5% had insulin resistance (HOMA>3.6). 9 Using a 2-h OGTT glucose limit of 140 mg/dL, 23.3% had IGT. Obese individuals presented the highest frequency of IR (χ2, P<0.001), but the frequency of IGT was not different among groups.
Data are mean±SD values.
By analysis of variance, P value among nutritional status groups.
BMI, body mass index; F, female; HOMA, homeostasis model assessment; ISI-Composite, composite insulin sensitivity index; M, male; OGTT, oral glucose tolerance test.
Excretion of 13CO2 became apparent in breath 30 min after the ingestion of the glucose load, and it increased gradually over time. Oxidation rates during Test 1 and Test 2 behaved almost identically (Fig. 1). The 13C-GBT, as percentage oxidized dose at 180 min, showed a lower variability compared with the other IR surrogates studied (Table 2). After stratification by nutritional status the 13C-GBT variability tended to be higher in lean individuals than in obese or overweight subjects, but no statistical significance was reached. Likewise, the CVs for post-load surrogates did not differ among lean, overweight, or obese individuals.
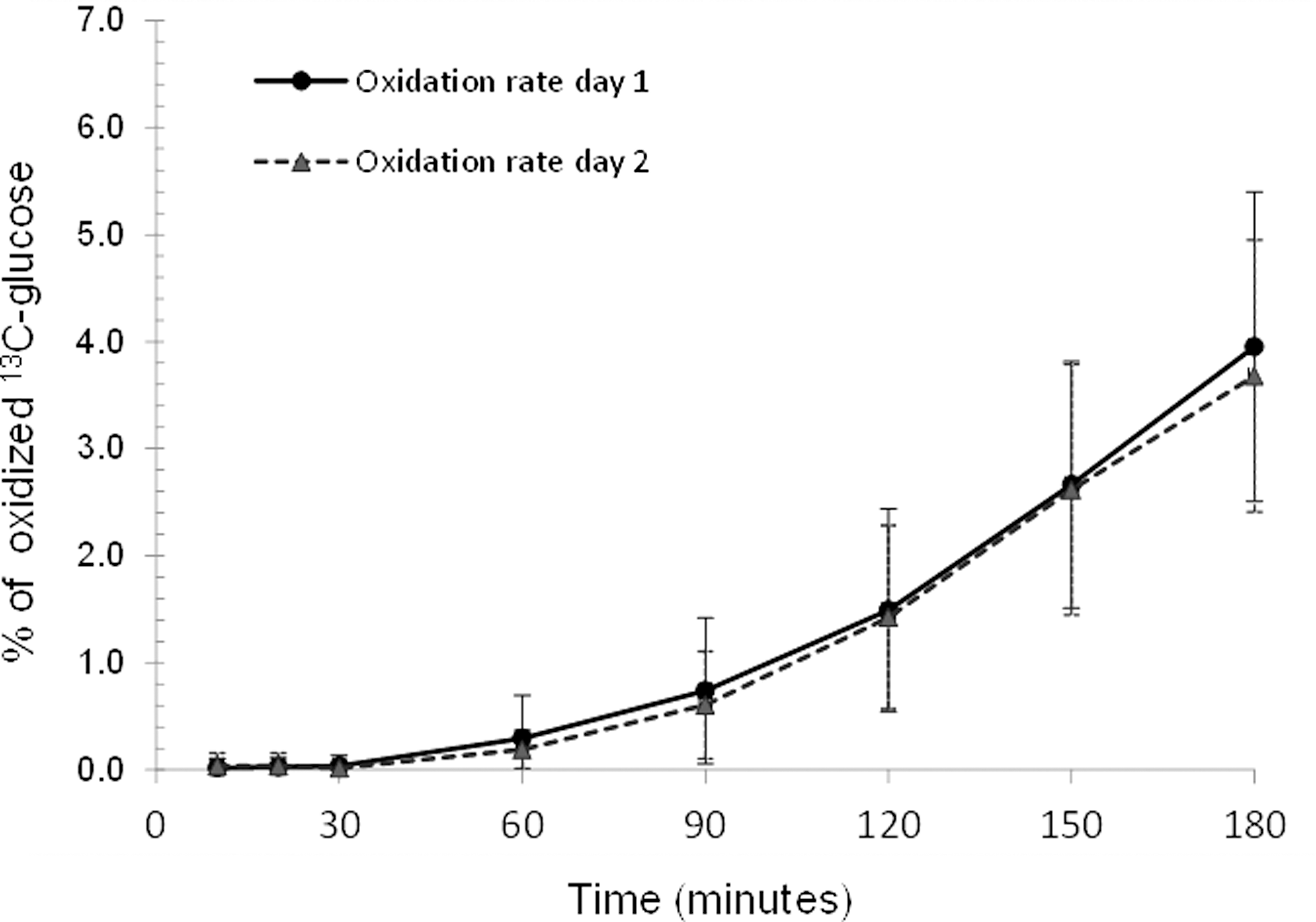
Oxidation rate curves for Test 1 and Test 2 (n=86).
Data are mean±SD values.
Significant differences by one-way analysis of variance and Dunnett's post hoc test between insulin resistance surrogates and the [13C]glucose breath test.
CV, coefficient of variation; HOMA, homeostasis model assessment; ISI-Composite, composite insulin sensitivity index; OGTT, oral glucose tolerance test.
Bland–Altman plots for the 13C-GBT and the other studied IR surrogates are presented in Figure 2. The breath test–derived measurements for each individual observation demonstrated a lower dispersion around the overall mean than that of the other IR surrogates. Also, the 13C-GBT exhibited the lowest discrepancy (7.16%) compared with fasting (HOMA, 26.26%; insulin, 24.3%) and OGTT-derived (ISI-Composite, 24.9%; 2-h insulin, 43.78%; 2-h glucose, 14.96%) surrogates.

Bland–Altman plots for [13C]glucose breath test and other insulin resistance surrogates:
Significant associations between the percentage of oxidized dose at 180 min and weight (r=−0.60), BMI (r=−0.58), HOMA (r=−0.41), 2-h OGTT glucose (r=−0.29), 2-h OGTT insulin (r=−0.21), and ISI-Composite (r=0.51) were found.
Discussion
Results from this study demonstrate that the 13C-GBT is a reliable method to assess IR in adult subjects who have not yet developed T2DM. In addition, we are confirming that the reliability of the 13C-GBT is better than that of other fasting and post-load IR surrogates.
To our knowledge, the reliability of the 13C-GBT has been approached only in one study that included lean, obese, and T2DM subjects. 21 The authors reported that the 13C-GBT exhibited low variability, with a CV for the oxidized dose at 180 min of 7.9±3.1%. Although such a CV is lower than that found in our study (12.99±11.60%), the disparity is probably due to methodological differences between the two studies. For instance, whereas we used two consecutive measurements, the other study included three determinations, which is expected to decrease variability. In addition, we excluded T2DM subjects, as opposed to the other study in which most of the studied individuals presented with T2DM, and therefore they exhibited by then severe impairment in glucose metabolism. This is important because if an individual has already developed an irreversible damage in glucose metabolism, the alteration in glucose oxidation is expected to be consistent throughout time. Nevertheless, despite the methodological differences, results from our study are still consistent with results of the above-mentioned study in that the 13C-GBT exhibits low intrasubject variability, making it a reliable method to detect IR even if diabetes has not developed.
In addition, our results are comparable to those of others regarding the high variability of the IR surrogates derived from fasting and from an OGTT, confirming that the applicability of such proxies is limited. For instance, the CV for HOMA identified in our study was 19.4%, which is comparable to the 23.5% reported by Sarafidis et al. 23 Likewise, the CV of 30% for 2-h insulin found in our study is similar to the 20–30% reported by Wolever et al. 16 We found a CV of 17.1% for ISI-Composite, and although this is a little higher than that reported by Gordon et al. 24 (14.4%), this difference is likely because they conducted four repeated measurements. In the case of the 2-h glucose, our CV of 10.6% is comparable to that reported in the studies of Wolever et al. 16 (12.7%), Schousboe et al. 17 (15%), and Singal et al. 21 (13%), and these CVs are lower than those of the 13C-GBT found in our study and in that of Singal et al. 21 However, it is important to take into account that the 2-h glucose value reveals IGT, which is a more severe alteration in glucose metabolism than IR.
We believe that our study accounted for several important concerns, improving the strength of our conclusions. Of important consideration is that the dose of [U-13C]glucose was calculated taking into account each subject's body weight, in the assumption that if the dose is similar among individuals with different nutritional status, those who are obese would receive less labeled glucose relative to body weight than their lean counterparts. For example, in the study of Lewanzuck et al., 19 in which a solution with a small dose of 25 mg of [U-13C]glucose was administered equally to lean and obese individuals, the authors found that those who were obese showed a rate of oxidation 38% less than that of nonobese subjects. However, from these data it is difficult to distinguish whether obese individuals are poor oxidizers or they only received a lower dose of labeled glucose. As opposed to the study of Lewanzuck et al., 19 the studies of Dillon et al. 20 and Singal et al. 21 used a much higher dose of [U-13C]glucose (150 mg), diminishing the possibility of misinterpretation, despite body weight not being taken into consideration, but the cost of the study would likely be increased.
Besides the adjustment by body weight, a mathematical correction was conducted to analyze oxidation data. That was done because we expected a quantitative competition between labeled and nonlabeled glucose uptake as [U-13C]glucose was calculated relative to body weight, whereas nonlabeled glucose was held constant (75-g OGTT). Whether this adjustment is the best approach to evaluate glucose oxidation is not yet defined. However, the correlation coefficients between oxidation rates and the results from other IR surrogates found in our study are comparable to those reported by others, 19 –21,25 suggesting that the correction was appropriate.
Also, we thought that if the proportion of carbon-13 varies among the different batches of the anhydrous glucose used for the OGTT, the natural abundance of 13CO2 in breath would vary accordingly. Hence, we measured the 13C/12C ratio in random batches of glucose by elemental analysis coupled to ratio mass spectrometry. The proportion of carbon-13, expressed as δ13 PDB units, was −10.72, similar to that reported by Mosora et al. 26 for maize glucose (−10.2 δ13 PDB units). It is noteworthy that Mosora et al. 26 observed an increment of 4.6 PDB units in exhaled CO2 after the ingestion of 100 g of maize glucose. This increment is considerably smaller compared with that provided by a common dose of [U-13C]glucose (approximately 40 PDB units). Thus, given that no differences between glucose batches were observed, we made certain that our results were not modified by the amount of carbon-13 in anhydrous glucose.
In addition to all of the above, other strategies were considered to strengthen our results. For instance, we recruited a larger sample of individuals than other studies so that numbers approached the validity and reliability of the breath test. Furthermore, we included individuals without diabetes but within a wide range of BMI to make sure that a wide spectrum of insulin sensitivity was included. Nevertheless, we recognize that because the IR surrogates, other than the 13C-GBT, were repeated only in 27 individuals, our conclusion regarding the variability of OGTT-derived surrogates may be limited. However, comparison between the CVs of the entire samples with those of the subset of 27 individuals, as presented in Table 2, demonstrates that with the small sample size a similar pattern is obtained, suggesting that our results are accurate.
Also, because 23% of our sample exhibited IGT, which could have influenced the results, we repeated the analysis excluding IGT subjects. This analysis showed that the 2-h insulin level was lower in this subset than in the entire sample (83.85±53.00 vs. 108.57±81.35 μU/mL, respectively), demonstrating that surrogates of insulin sensitivity change with varying degrees of glucose tolerance. The different results in insulin response suggest that the breath test can be a better alternative than glucose/insulin measures in populations with variable glucose tolerance.
In conclusion, we demonstrate that the13C-GBT is a reproducible method to identify adult individuals with alterations in glucose metabolism, including those with decreased insulin sensitivity and IGT. We also confirmed that the reproducibility of the 13C-GBT is better than that of other IR surrogates derived from fasting or from an OGTT. The identification of a valuable cutoff point is warranted; studies with that purpose are under way in our laboratory, using the clamp technique as the standard.
Footnotes
Acknowledgments
The authors acknowledge Pedro Morales, MSc, and Edith Cienfuegos, MSc, from the Geology Institute (Universidad Nacional Autónoma de México) for analytical determinations of 13C abundance in anhydrous glucose by isotope ratio mass spectrometry. This study was supported with grants from the Consejo Nacional de Ciencia y Tecnología and the Fondo de Investigación en Salud of the Mexican Institute of Social Security.
Author Disclosure Statement
No competing financial interests exist.