
Abstract
Background:
Glucose fluctuation often remains to be corrected under basal-supported oral therapy. We investigated the efficacy of adding once-daily rapid-acting insulin in Japanese diabetes patients treated with basal-supported oral therapy.
Subjects and Methods:
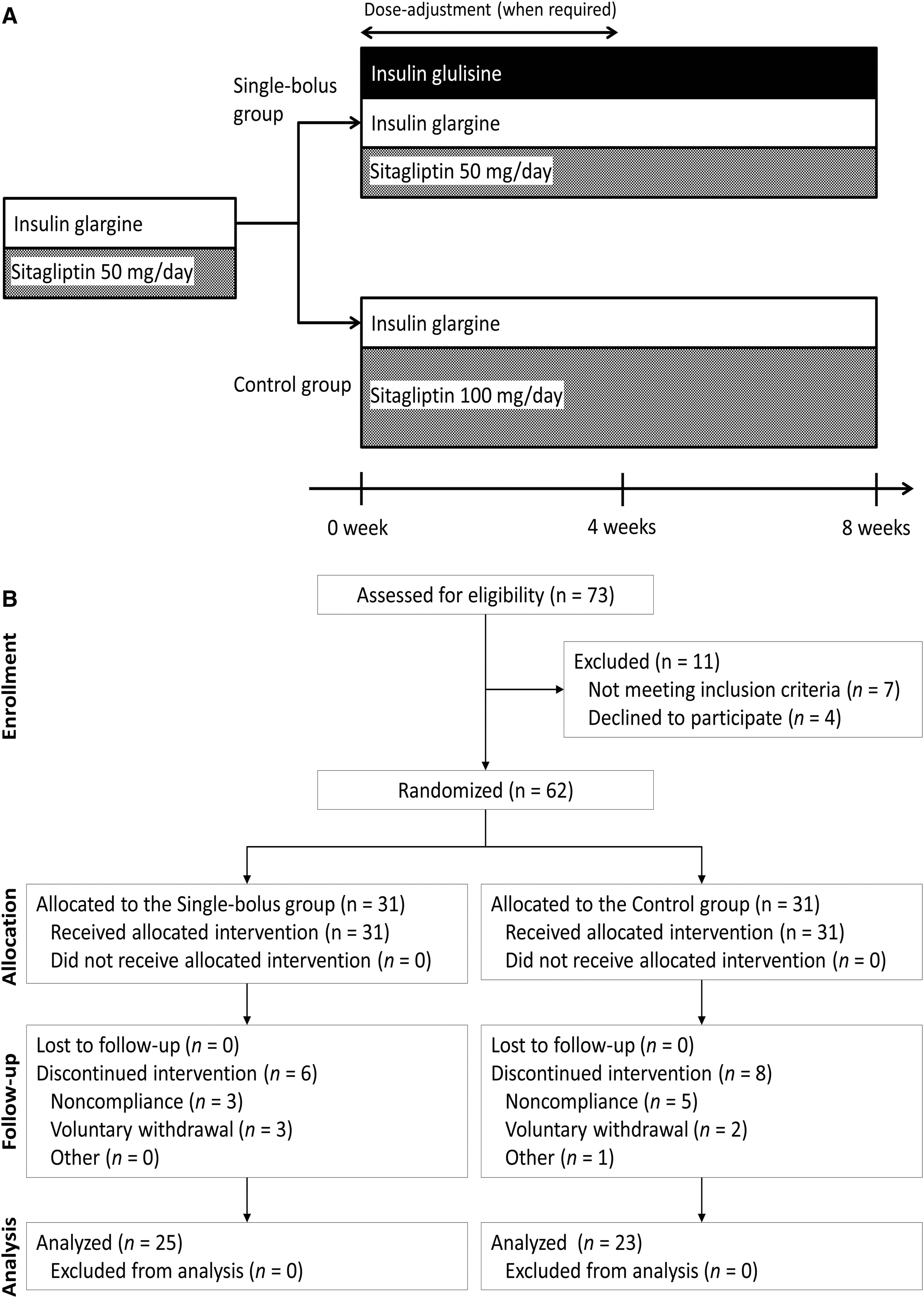
In this 8-week, parallel-group, randomized, open-label trial, 62 Japanese adults with type 2 diabetes treated with insulin glargine and 50 mg of sitagliptin were randomized into the following two arms: the single-bolus group, in which once-daily insulin glulisine was initiated at a main meal at a fifth (i.e., 20%) the dose of insulin glargine, and the control group, in which the dose of sitagliptin was maximized to 100 mg. The primary end point was the change of glycemic fluctuation assessed with the M-value.
Results:
Baseline hemoglobin A1c levels, mean blood glucose profiles, and M-value were 7.2±0.6%, 9.3±1.7 mmol/L, and 21±13 units, respectively. At the end of the study, the single-bolus group had a greater reduction of M-value than the control group (P=0.02); the difference was 6.5 units (95% confidence interval, 1.1–11.9 units). The single-bolus group also had a greater reduction of mean blood glucose levels (P=0.01). There were no significant differences in the incidence of hypoglycemia or the weight change between the two groups (P>0.05).
Conclusions:
Adding once-daily insulin glulisine was more effective in controlling the glycemic fluctuation in Japanese type 2 diabetes patients treated with insulin glargine together with sitagliptin.
Introduction
T
However, some patients receiving BOT have uncontrolled postprandial hyperglycemia, despite their good control of fasting glucose levels. 9,10 Consequently, daily glycemic variability, or fluctuation, is observed in these patients. Although the additional multiple injection of rapid-acting insulin at every meal, so-called intensive insulin therapy, may reliably lower postprandial glycemia, 11,12 substantial numbers of patients in clinical practice hesitate to receive this therapy because the inconvenience of many injections would burden their lifestyle.
In previous reports, proposals were made to initiate a single daily prandial bolus of a rapid-acting insulin analog, as the first step toward intensive insulin therapy in these patients. 13,14 However, few clinical studies have investigated the efficacy of adding a once-daily prandial bolus on glycemic control, by comparing with other strategies, such as an increase in dosage of ongoing oral hypoglycemic agents.
The aim of the current study was to investigate whether initiating once-daily rapid-acting insulin according to a simple regimen would be more beneficial than maximizing the dosage of an ongoing DPP-4 inhibitor in Japanese type 2 diabetes patients treated by long-acting insulin together with the DPP-4 inhibitor.
Subjects and Methods
Study design
This 8-week, parallel-group, randomized, open-label trial compared the efficacy and safety between two study arms in Japanese type 2 diabetes adults treated with insulin glargine, a long-acting insulin analog, plus sitagliptin, a DPP-4 inhibitor, at 50 mg/day. In one arm (the single-bolus group), once-daily insulin glulisine, a rapid-acting insulin analog, was initiated at a prespecified dose, whereas in the other (the control group), the dosage of ongoing sitagliptin was doubled. In Japan, 50 mg/day of sitagliptin is approved and recommended as the normal dosage. Increase of the dosage up to 100 mg/day is also approved, in cases in which the glucose-lowering effect is insufficient.
The current study was conducted at Shiraiwa Medical Clinic, Osaka, Japan, between March and June 2013. The current study was performed in accordance with the Declaration of Helsinki and was approved by the ethics committee of Shiraiwa Medical Clinic. Written informed consent was obtained from every participant in the current study.
Study population and procedures
The study population comprised Japanese adults (≥20 years old) with type 2 diabetes mellitus, who were treated by a titrated dose of insulin glargine together with 50 mg/day of sitagliptin but who had postprandial hyperglycemia and accompanying glycemic fluctuations. The participants had either postprandial glucose levels of ≥10.0 mmol/L (180 mg/dL) or hemoglobin A1c levels of ≥7.0%, or both, even after insulin glargine was titrated to target preprandial glucose levels of <6.1 mmol/L (110 mg/dL). The exclusion criteria were difficulty in performing self-monitoring of blood glucose (SMBG), moderate or severe renal impairment (creatinine clearance below 50 mL/min or serum creatinine ≥1.5 mg/dL in males and 1.3 mg/dL in females, according to the manufacturer's labeling), severe hepatic and/or cardiac disease, hypersensitivity to the drug using in the current study, and pregnant or breast-feeding females. We also excluded patients treated together with antidiabetes drugs other than low-dose sulfonylureas (defined as less than one-quarter of the highest approved dose) and/or metformin, for the purpose of minimizing the heterogeneity within the study population.
Eligible participants were randomized and allocated to the single-bolus group or the control group (Fig. 1A). The allocation was performed using stratified block randomization, with a block size of 4. The stratification factors were sex (male or female) and age (<65 or ≥65 years). Accordingly, randomization was blocked within four strata. In the single-bolus group, a single daily prandial bolus of insulin glulisine was administered before the main meal, defined as the meal that led to the highest postprandial blood glucose levels. The administration time of insulin glargine was accommodated to that of insulin glulisine, without changing the insulin glargine dose, simply because providing the injections at one time was expected to be more convenient for patients than at different times. Insulin glulisine was initiated at a fifth (i.e., 20%) the dose of insulin glargine (Week 0). The current initiating dose of insulin glulisine was derived from the data of type 2 diabetes patients who were treated with both long-acting and rapid-acting insulin by diabetologists in the clinic and was supported by their empirical opinions. The dose was adjusted during the first 4 weeks when required. The dose adjustment was according to the following protocol: insulin glulisine was increased in dose by 2 units (or, alternatively, 1 unit in some patients for safety) when postprandial glucose levels were 10.0 mmol/L or higher for 3 days. It was decreased in dose by 1 unit (or, alternatively, 2 units in some patients for safety) when postprandial glucose levels were below 6.1 mmol/L or hypoglycemia occurred. On the other hand, insulin glargine was increased in dose by 2 units (or, alternatively, 1 unit in some patients for safety) when fasting glucose levels were 6.1 mmol/L or higher for 3 days. It was decreased in dose by 1 unit (or, alternatively, 2 units in some patients for safety) when fasting glucose levels were below 4.4 mmol/L or hypoglycemia occurred. Note that selection of an alternative less intensive option was allowed to give top priority to safety (i.e., avoidance of hypoglycemia) in some patients, at the diabetologist's discretion. In the control group, the dosage of sitagliptin was maximized to 100 mg/day at Week 0. Sitagliptin was administered once daily, and the dosage was maintained during the study period. The dose of insulin glargine could be adjusted based on the aforementioned dose-adjustment protocol, when required. The participants in both groups were asked to visit the clinic during Weeks 4 and 8. They were requested to perform seven-point SMBG (before and 2 h after breakfast, lunch, and dinner and at bedtime) for 5 days prior to the clinic visit. SMBG was performed using OneTouch® UltraVue™ (Johnson & Johnson K.K., Tokyo, Japan). 15 They were also asked to maintain their usual physical activity during the study.
Study outcomes
The primary end point was the change of the glycemic fluctuation evaluated in terms of the M-value, 16 calculated from the records of SMBG, at the end of the study, using last observation carried forward data analysis. We also evaluated the mean amplitude of glycemic excursions, 17 interquartile range, postprandial blood glucose levels, and mean blood glucose levels derived from the SMBG data, as well as hemoglobin A1c levels. Safety was evaluated in terms of the incidence of hypoglycemic episodes, changes in body weight, and other adverse events. The threshold of hypoglycemia was defined as lower than 3.3 and 3.6 mmol/L irrespective of the presence of symptoms.
Statistical analysis
Data are presented as mean and SD values for continuous variables or as percentages for dichotomous variables. A P value of <0.05 was considered to be significant. The difference between the two groups was tested using the unpaired t test for continuous variables, Fisher's exact test for dichotomous variables, and the χ 2 test for other discrete variables. The incidence of hypoglycemia was compared using the χ 2 test of two Poisson rates. The sample size was set at 30 per group, or 60 in total, which was sufficient to detect 0.8 SD of the intergroup difference in the primary end point, with a power of 80%, a two-sided significance level of 5%, and a dropout rate of 20%.
Results
A flow diagram of the current study is shown in Figure 1B. In total, 62 patients were randomized. During the follow-up, six participants in the single-bolus group and eight in the control group were discontinued from the intervention. The most common reasons were voluntary withdrawal and noncompliance with frequent SMBG. Finally, the full analysis set comprised a total of 48 patients (single-bolus group, n=25; control group, n=23). They were 64±9 years old, and 33 patients (69%) were male. The dosage of insulin glargine was 15±9 units per day. Hemoglobin A1c levels, mean blood glucose levels, and M-value at baseline were 7.2±0.6%, 9.3±1.7 mmol/L, and 21±13 units, respectively. There were no significant differences in baseline characteristics between the two groups (Table 1).
Data are mean±SD values or n (percentage) as indicated.
The main meal was defined here as the meal with the highest postprandial blood glucose levels.
IQR, interquartile range; MAGE, mean amplitude of glycemic excursions.
In the single-bolus group, once-daily insulin glulisine was initiated at the dosage of 3±1 units per day. Ten patients (40%) injected insulin before breakfast, six patients (24%) before lunch, and nine patients (36%) before dinner. During the study period, the dosage was reduced in one patient (by 1 unit per day), whereas the dosage was increased in two patients (by 1 and 2 units per day); the dosage was unchanged in the remaining patients. Consequently, the dosage of insulin glulisine at the end of the study was 3±1 units per day. The dose of insulin glargine was increased in one patient in the single-bolus group and one patient in the control group, whereas it was decreased in one patient in the single-bolus group and one patient in the control group. Consequently, the dose of insulin glargine at the end of the study was 16±7 units per day in the single-bolus group and 15±10 units per day in the control group (P=0.87).
Figure 2 shows the change of M-value during the study period. At the end of the study, the single-bolus group had a significantly greater reduction of M-value compared with the control group (P=0.02); the intergroup difference reached 6.5 units (95% confidence interval, 1.1–11.9 units). In addition, as shown in Table 2, the single-bolus group also had a significantly greater improvement of other indices related to glycemic control than the control group.
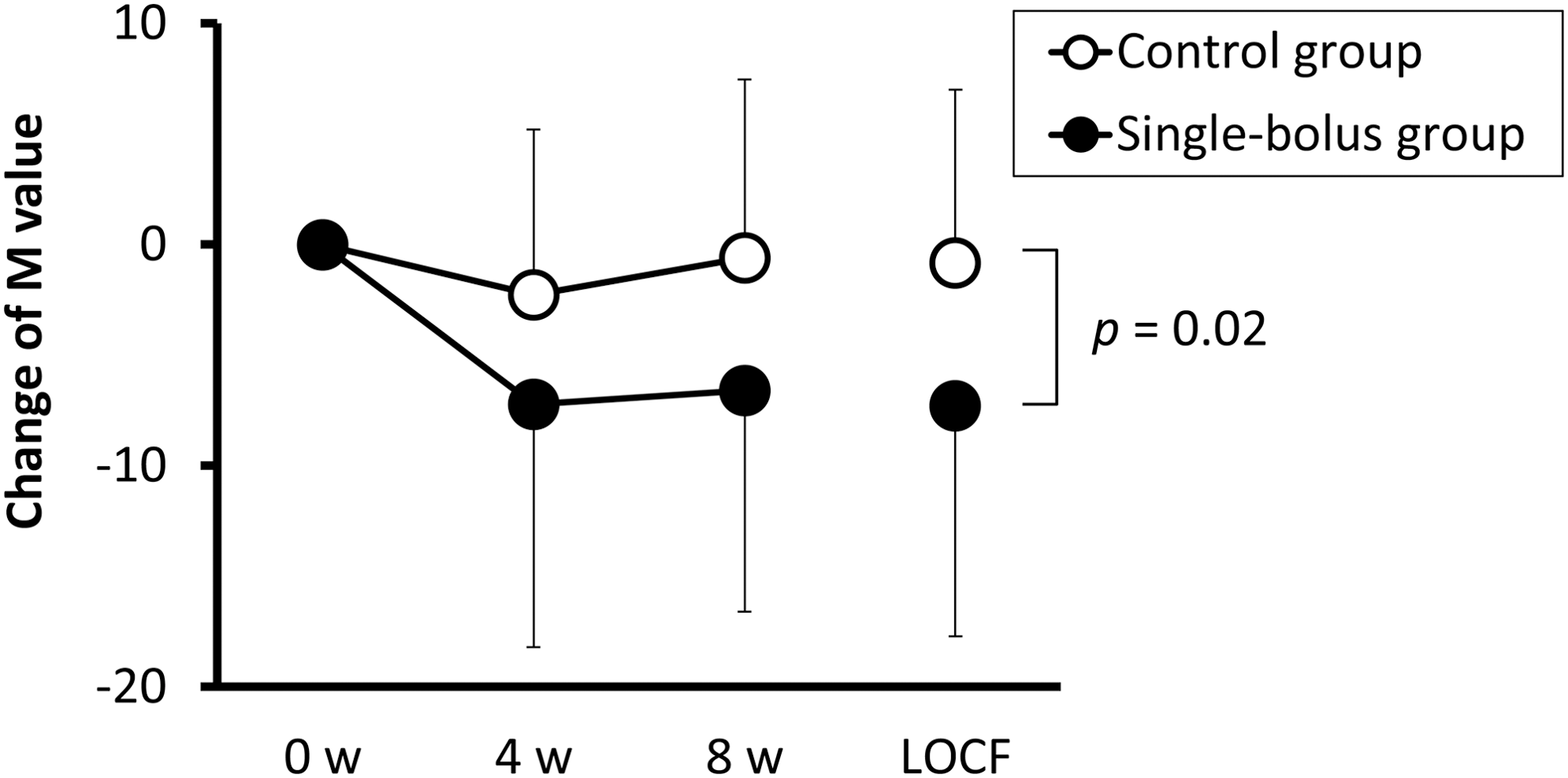
Blood glucose fluctuation during the study period. Data are mean and SD values. LOCF, last observation carried forward; w, week.
Data are mean±SD values.
IQR, interquartile range; MAGE, mean amplitude of glycemic excursions.
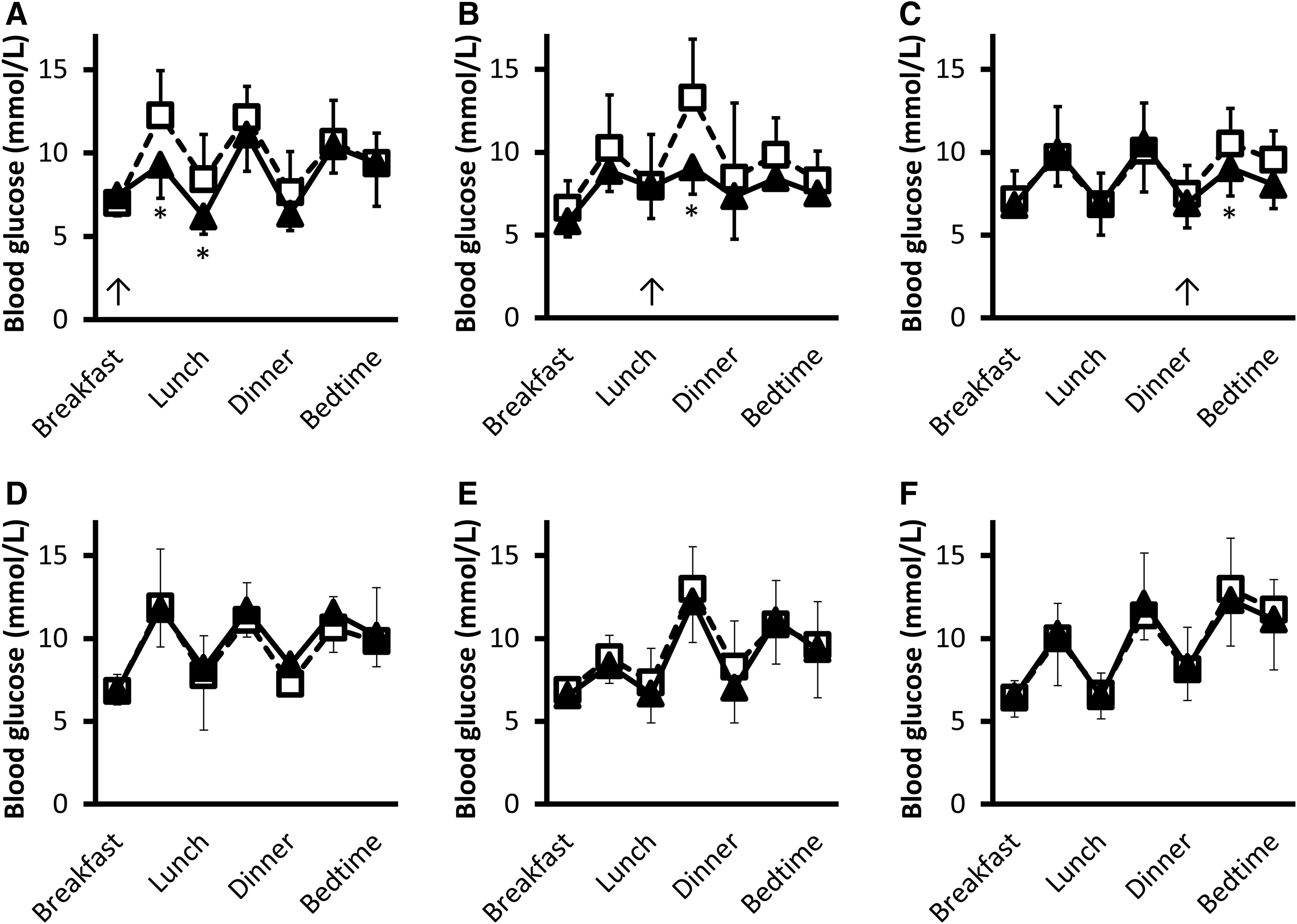
Figure 3 shows seven-point blood glucose profiles before and after the intervention. The introduction of once-daily insulin glulisine at the main meal was significantly associated with reduced blood glucose levels right after the meal, whereas postprandial blood glucose levels after the other meals were not significantly improved (Fig. 3A–C). No significant reduction of blood glucose profiles was observed in the control group (Fig. 3D–F). Supplemental analysis with the linear mixed model demonstrated that postprandial glucose levels after the main meal (i.e., the meal with the highest postprandial glucose levels at baseline) were significantly decreased in the single-bolus group (P<0.01) but not in the control group; the change was −3.6 mmol/L (95% confidence interval, −5.0 to −2.1 mmol/L) and −0.6 mmol/L (95% confidence interval, −1.5 to 0.3 mmol/L), respectively. The change was significantly different between the two groups (P<0.01). On the other hand, the change of postprandial glucose levels after the other meals was −0.3 mmol/L (95% confidence interval, −1.6 to 0.9 mmol/L) (P=0.35) in the single-bolus group, and 0.3 mmol/L (95% confidence interval, −0.4 to 1.0 mmol/L) (P=0.26) in the control group; the difference was not significant between the two groups (P=0.23).
Daily blood glucose profiles in
The incidence of hypoglycemia of <3.6 mmol/L was 0.29 episodes per week per person in the single-bolus group and 0.01 episodes per week per person in the control group (P=0.13). The corresponding incidence of hypoglycemia of <3.3 mmol/L was 0.03 and 0.04 episodes per week per person, respectively (P=0.92). There was no significant difference in weight change between the two groups (0.1±1.0 kg in the single-bolus group versus 0.4±1.2 kg in the control group; P=0.29). No other remarkable adverse events were observed in the current study.
Discussion
The current parallel-group, randomized, open-label study demonstrated that the introduction of once-daily insulin glulisine significantly reduced the glycemic fluctuation as assessed in terms of M-value, compared with increasing the dosage of ongoing sitagliptin, in Japanese type 2 diabetes patients treated by insulin glargine together with sitagliptin.
Recent studies demonstrated the efficacy of BOT using DPP-4 inhibitors. 2 –8 However, postprandial hyperglycemia sometimes remains uncontrolled, albeit preprandial glucose levels are well controlled by the titration of long-acting insulin analogs. Consequently, daily glycemic variability or fluctuation was observed in some patients. The postprandial glucose excursion and the glycemic fluctuation are reported to be associated with an increased risk of vascular endothelial dysfunction, atherosclerosis, cardiovascular diseases, and mortality, independently of fasting glucose levels, mean glucose levels, or hemoglobin A1c levels. 18 –24 Their correction is now a challenging issue in clinical practice. 25 –28 Previous reports proposed initiating a single daily prandial bolus of a rapid-acting insulin analog, as the first step toward intensive insulin therapy for correcting glycemic control. 13,14 However, few clinical data are so far available in regard to whether this strategy is a more effective way to correct glycemic control than other “less invasive” strategies, especially in Asians. Insulin secretory capacity and severity of insulin resistance are reported to be different among different ethnic groups, 29,30 which may influence the efficacy of some insulin regimens. 31,32 Our data would serve as a basis for encouraging patients to start once-daily bolus insulin instead of increasing the dosage of oral agents in Japanese diabetes patients treated with BOT.
In the current study, insulin glulisine was introduced with a very simple regimen in the single-bolus group; the injection was initiated at one-fifth (i.e., 20%) the dose of insulin glargine. Consequently, the dose of insulin glulisine was reduced in only one patient during the study period, and the reduction was only 1 unit/day. Nonetheless, hypoglycemic episodes were as scarcely observed in the single-bolus group as in the control group, indicating that the current simple regimen to determine the initiating dose would be clinically safe. On the other hand, during the study period, the dose of insulin glulisine was increased only slightly (up to 2 units/day) in two other patients, and the dose was unchanged in the remaining, majority (88%) of the patients. Nonetheless, the reduction of glycemic fluctuation was significantly greater than that in the control group, indicating the clinical efficacy of the current regimen in the single-bolus group.
In general, one practical issue in initiating the insulin injection for some clinical practitioners is to determine an appropriate (that is, not excessive or insufficient) initiating dose of the insulin. An insufficient dose would lack the clinical efficacy, whereas an excessive dose would in turn cause increased hypoglycemic episodes, both of which would disappoint and discourage the patients who have at long last agreed to initiate the additional insulin injection. The current study provided a simple, safe, and effective regimen to determine the initiating dose, which would be useful in clinical practice.
The current study adopted a 4-week dose-adjustment period in the single-bolus group, simply based on the empirical hypothesis that it would take about 4 weeks for dose adjustment in some patients. Consequently, the remaining study period was only 4 weeks in this 8-week study design. However, the effect of a rapid-acting insulin analog on glycemic control can be immediately reflected by daily blood glucose profiles. We therefore believe that this remaining 4-week period was not too short to assess the glycemic control, as long as it was evaluated with a calculation from daily blood glucose profiles.
There were some limitations in the current study. First, the current study was an open-label, and not double-blind, trial. This design would reduce validation of results, although the design has been widely adopted in clinical trials on insulin therapy. 1,9 –11 Second, the dropout rate of this study was relatively high. The major reason for dropping out was the difficulty in performing SMBG as directed. In the current study, the participants were requested to perform seven-point SMBG for 5 days before each visit. However, such a frequent SMBG protocol was found to be difficult for these patients to perform in practical daily life. The dropouts had higher hemoglobin A1c levels at baseline (7.7±1.0% vs. 7.2±0.6%) (P=0.04). Similarly, SMBG-evaluated glycemic control tended to be poorer, although the data were available only in three dropouts, and therefore it was difficult to test significant differences (36±15 units of M-value, 123±15 units of mean amplitude of glycemic excursions, 5.2±1.4 mmol/L of interquartile range, and 11.6±1.6 mmol/L of mean blood glucose levels). There was no significant difference in other baseline characteristics (P>0.05). Although baseline characteristics were not different between the dropouts in the single-bolus group and those in the control group, this high dropout rate might have some influence on the outcomes. Third, the study period was limited to 8 weeks, which was relatively short to evaluate the safety measures and the change of hemoglobin A1c levels. 33 Fourth, the accepted level of noninferiority as well as superiority in glucose fluctuation remains to be fully established. Given that an M-value of up to 18 units was defined as good control, 16 it might be alternatively and safely said that two interventions would be similarly effective in clinical practice if the M-value decreased in both arms to ≤18 units. Fifth, for the purpose of minimizing the heterogeneity within the study population, we simplified the study protocol and limited the combined use of other antidiabetes agents. Several combinations of antidiabetes agents are now available in clinical practice. Future studies will be needed to reveal whether the introduction of insulin glulisine with the current simple regimen will similarly provide a beneficial effect in patients treated with other combinations of antidiabetes agents.
In conclusion, the current parallel-group, randomized, open-label study demonstrated that initiating once-daily insulin glulisine at 20% the dose of insulin glargine provided a significantly smaller glycemic fluctuation, assessed in terms of M-value, than increasing the dosage of sitagliptin to 100 mg/day in Japanese type 2 diabetes patients treated with insulin glargine plus sitagliptin.
Footnotes
Acknowledgments
M. Takahara was a Research Fellow of the Japan Society for the Promotion of Science.
Author Disclosure Statement
The authors received honoraria for lectures and advisory activities, and research funding, from Sanofi K.K., MSD K.K., and Ono Pharmaceutical Co. Ltd.