
Abstract
Background:
Closed-loop control of blood glucose levels in people with type 1 diabetes offers the potential to reduce the incidence of diabetes complications and reduce the patients' burden, particularly if meals do not need to be announced. We therefore tested a closed-loop algorithm that does not require meal announcement.
Materials and Methods:
A multiple model probabilistic predictive controller (MMPPC) was assessed on four patients, revised to improve performance, and then assessed on six additional patients. Each inpatient admission lasted for 32 h with five unannounced meals containing approximately 1 g/kg of carbohydrate per admission. The system used an Abbott Diabetes Care (Alameda, CA) Navigator® continuous glucose monitor (CGM) and Insulet (Bedford, MA) Omnipod® insulin pump, with the MMPPC implemented through the artificial pancreas system platform. The controller was initialized only with the patient's total daily dose and daily basal pattern.
Results:
On a 24-h basis, the first cohort had mean reference and CGM readings of 179 and 167 mg/dL, respectively, with 53% and 62%, respectively, of readings between 70 and 180 mg/dL and four treatments for glucose values <70 mg/dL. The second cohort had mean reference and CGM readings of 161 and 142 mg/dL, respectively, with 63% and 78%, respectively, of the time spent euglycemic. There was one controller-induced hypoglycemic episode. For the 30 unannounced meals in the second cohort, the mean reference and CGM premeal, postmeal maximum, and 3-h postmeal values were 139 and 132, 223 and 208, and 168 and 156 mg/dL, respectively.
Conclusions:
The MMPPC, tested in-clinic against repeated, large, unannounced meals, maintained reasonable glycemic control with a mean blood glucose level that would equate to a mean glycated hemoglobin value of 7.2%, with only one controller-induced hypoglycemic event occurring in the second cohort.
Introduction
M
Insulin pumps and the recent, ongoing development of continuous glucose monitors (CGMs) offer an opportunity to reduce the patient burden and may potentially decrease the risk of both hypo- and hyperglycemia through closed-loop control. Several different closed-loop control algorithms have been proposed and tested for use in a closed-loop artificial pancreas, as reviewed by Bequette, 3,4 Cobelli et al., 5 and Hovorka. 6 Algorithms include on–off predictive low glucose suspend systems to prevent overnight hypoglycemia, 7 proportional integral derivative, 8,9 fuzzy logic, 10 –14 and model predictive control. 15 –22
The algorithm used in this article—multiple model probabilistic predictive control (MMPPC)—is in the class of model predictive control. The initial MMPPC design was optimized using in silico simulation studies. 23 Here, we have focused on full closed-loop control in which meals are unannounced. In this study, we specifically provided large meals (0.8–1.2 g of carbohydrate/kg). Also, unlike multihormone systems, 24 we only used insulin to control the glucose levels.
Full closed-loop control algorithms are at a significant disadvantage compared with ideal insulin dosing for a meal, where, because of the delayed onset of action of current analog insulins, the meal injection should be given 20 min before the meal. 25 In contrast, fully closed-loop systems must delay meal insulin dosing until the meal-induced increase in glucose levels is detected and recognized as a meal event lest insulin is given for a nonexistent meal.
Materials and Methods
Protocol
The protocol was approved by both the Food and Drug Administration (IDE G100105) and the Stanford Human Subjects Review Board. Informed consent was obtained from all patients. Patients were between 21 and 45 years of age with diabetes duration of more than 1 year and had used an insulin pump for more than 3 months. At the enrollment visit, two Abbott Diabetes Care (Alameda, CA) Navigator® CGMs were inserted, and subjects were trained in their use as per the manufacturer's instructions. Between the enrollment and research center admission, subjects were contacted once every 3–4 days to help optimize their control. New sensors were inserted 2 days and 1 day before the research center admission. Subjects arrived fasting prior to 8 a.m. on the day of admission, and full closed-loop control was initiated by 9 a.m. The most accurate sensor was linked to a study Navigator device that communicated by a serial port to the study computer. The patient's insulin pump was replaced with an Insulet (Bedford, MA) OmniPod® pump infusing insulin lispro (Humalog®; Eli Lilly & Co., Indianapolis, IN). The modular artificial pancreas software developed at the University of California, Santa Barbara allowed communication and data transfer from both the Navigator sensor and OmniPod pump to the bedside computer. 26 Reference glucose measurements were obtained through a peripheral intravenous line every 30 with the YSI® (Yellow Springs, OH) glucose and lactate analyzer and the Glucoscout® (International Biomedical, Austin, TX) used for reference glucose values. Blood glucose measurements were obtained every 15 min for 2 h after each meal. When the GlucoScout was used, a YSI measurement was obtained every 2 h. Only YSI measurements were used when the blood glucose or sensor glucose level was ≤70 mg/dL. If the YSI blood glucose level was ≤70 mg/dL or the subject was having symptoms of hypoglycemia, YSI glucose values were obtained every 15 min until the blood glucose level was above 70 mg/dL. The GlucoScout calibration solution did not contain heparin. The patient's total daily dose and basal insulin profile were entered into the controller.
No premeal insulin was provided, nor were any meals “announced” to the control algorithm. Meals were set to be eaten at 9 a.m., 1 p.m., and 5:30 p.m. with one snack at 8 p.m. per patient desire. The meals were to be sized between 0.8 and 1.2 g of carbohydrate/kg. The meal schedule was allowed to shift up to 1 h earlier. The protocol forces the meals to be spread out at 4-h intervals to allow time to observe for overly aggressive meal dosing causing postprandial hypoglycemia.
Treatment for hypoglycemia was given when the subject requested treatment or the YSI glucose level was <60 mg/dL. If hypoglycemia treatment was given, the glucose value was entered into the controller through the artificial pancreas system platform, 26 allowing a temporary reduction in aggressiveness by the controller.
Subjects exercised by walking for up to 20 min between blood draws, but there was no strenuous exercise.
Methods
The two patient cohorts that were enrolled used two distinct, although similar, controllers. Each controller has a prediction and optimization component. The prediction component predicts the future glucose distribution (mean and SD), explicitly taking into account uncertain future meals, endogenous glucose production, and insulin sensitivity. The optimization component uses the resultant estimates and predictions to calculate the insulin bolus. This division allows for the separate verification of the prediction stage against preexisting datasets.
The predictor for the first four patients has been previously described, 27 and the second set of six patients used a predictor that was published in 2012. 28 The second predictor uses statistical data from the National Health and Nutrition Examination Survey 29 to anticipate the next meal between 8 a.m. and 5 p.m.
More specifically, both algorithms are based on seven-state linear models, with two states for insulin action, two states for meals, and one state each for the glucose level, the glucose rate of change, and the endogenous glucose production. Each uses a “bank” of these models where the models differ by when each assumes that the last meal started. Over time, new models are added assuming new meals, while old models are discarded or combined to prevent having too many different models. The models are weighted based on a combination of how well they fit the data and how probable they are. For example, a new model that was based on an old model that assumed a meal 10 min ago would have a very low initial weighting because two significant meals 10 min apart is highly unlikely. The seven states, including the meal size, are estimated using the Kalman filter time and measurement updates. Because each model includes uncertainty estimates for the states, we predict both the combined mean and SD of the model states 5 h into the future. The predictor for the second cohort incorporates the potential future meals into its predictions. So, predictions coming into 8 a.m. will trend upwards for the expected breakfast. At the same time, the uncertainty will balloon because of the uncertainty about the size and even existence of the impending meal.
For the first four patients the only controller-tuning parameters were the patient's total daily dose and an average basal rate. For the second cohort of patients the controller used the patient's total daily dose and his or her basal rate profile. The relevant information was taken from the patients' pumps on the morning of the admission visit.
The optimization component for each controller simply chose the insulin dose to generate a predetermined risk of decreasing glucose levels below a predetermined lower threshold over the next 5 h. This approach is predicated on the idea that insulin should be administered to decrease the glucose as close as possible to the lower threshold while allowing a small risk of hypoglycemia. For the first four patients the risk and thresholds are depicted in the left-hand graphs in Figure 1, whereas the risk and threshold factors for the second cohort are depicted in the right-hand graphs. For the second cohort, we ignore the glucose uncertainty at night, resulting in a proportional integral derivative–like control. To make the control more basal-like, we spread the commanded bolus over 75 min. This reduces the aggressiveness and allows for averaging out the effect of CGM noise.

Our results include the Low Blood Glucose Risk Index and the corresponding High Blood Glucose Risk Index. 30 These metrics serve as a composite measure of the duration and severity of low and high glucose levels, respectively. We also specify our results for a 24-h period to enable comparison of results between different clinical trials of different lengths. Here, because we have a 32-h trial, the 24-h metrics give half weighting to the first and last 8 h and full weighting to the middle 16 h.
Results
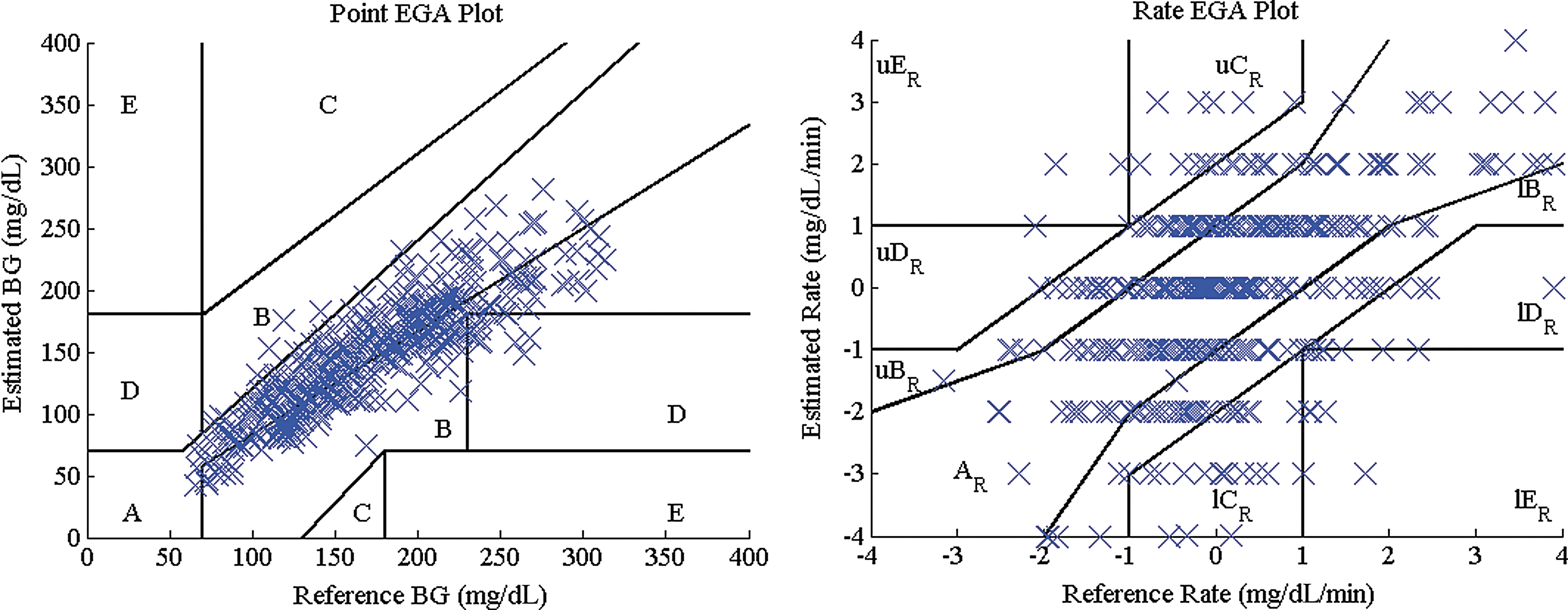
During this trial, the sensors were recalibrated only per the manufacturer's instructions. The reference glucose values were consistently above the CGM values for the last cohort, with a mean bias of −25 mg/dL. This corresponded to a mean absolute difference and mean absolute relative difference of 28.8 mg/dL and 16.4%, respectively. Figure 2 shows the Point Error Grid Analysis 31 and Rate Error Grid Analysis 32 plots.
Given the two distinct versions of the algorithm, we present each as a distinct dataset. Table 1 shows summary statistics across the entire study for each individual patient and across the two cohorts. The individual plots for each patient are included in Supplementary Figures S1–S10 (Supplementary Data are available online at
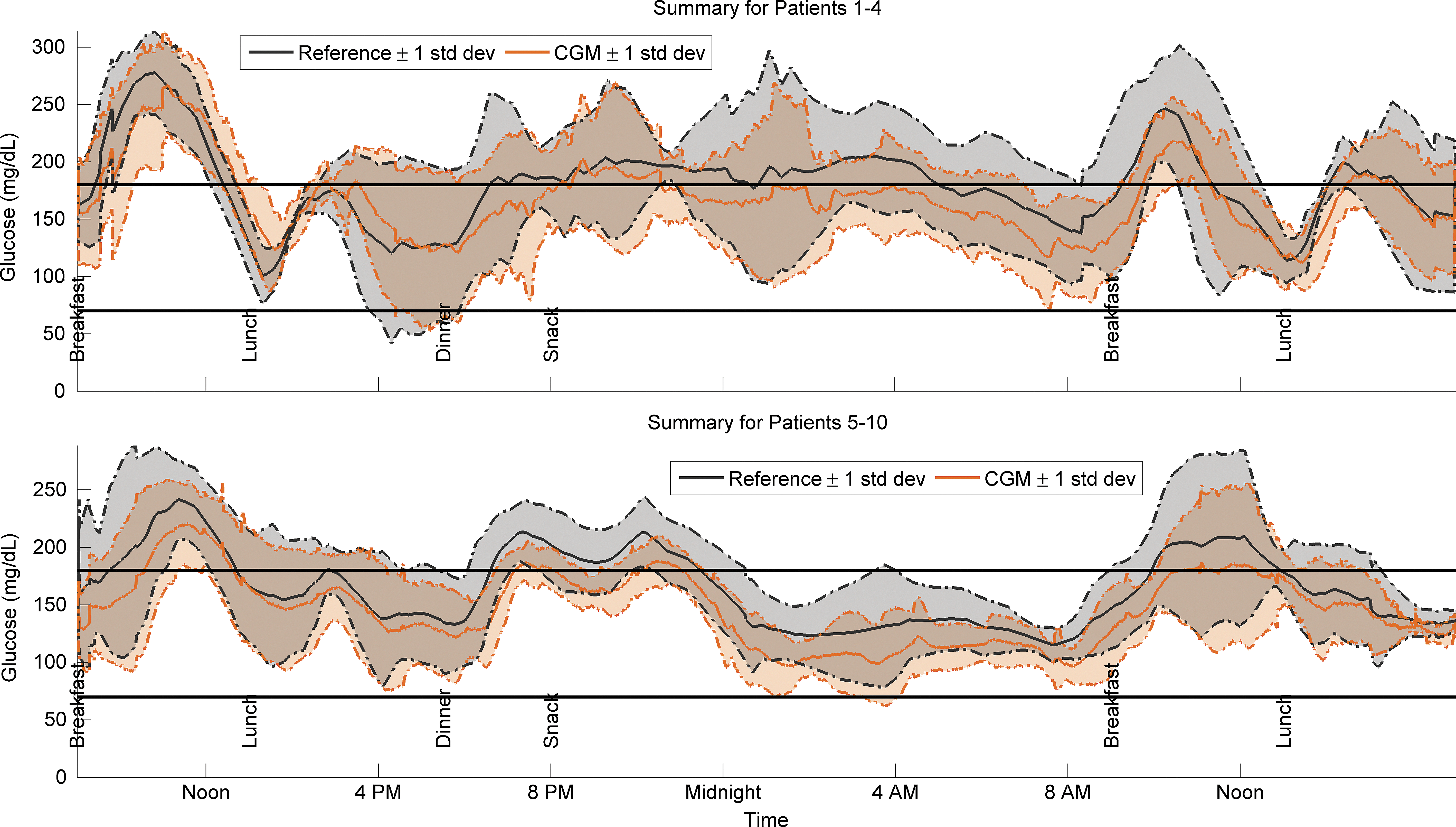
Summary plots:
Only data where the controller was properly initialized are shown.
There were two instances of hypoglycemia treated with extra carbohydrates.
There was one instance of hypoglycemia treated with extra carbohydrates.
The next lowest reference value is 89 mg/dL. No treatment was given.
The noted value was caused by a system error. The next lowest nadir value was 82 mg/dL.
The noted value was caused by a system error. The next lowest nadir value was 64 mg/dL.
CGM, continuous glucose monitor; TDD, total daily dose.
Approximated from the mean glucose level. 33
CGM, continuous glucose monitor; HbA1c, glycated hemoglobin; HBGI, High Blood Glucose Risk Index; LBGI, Low Blood Glucose Risk Index.
As indicated in Table 1, in the first cohort there were four postprandial periods where overly aggressive controller-commanded insulin injection required carbohydrate treatments. For the second patient cohort there were three interventions for hypoglycemia. For subject 7 a failed wire caused an extended period without closed-loop control. During this time, a physician administered lunch meal bolus, using the subject's preprogrammed settings, resulted in hypoglycemia. A loss of connectivity for subject 6 required a system restart, causing the controller to be unaware of past delivered insulin, and there was an over bolus for breakfast. The last intervention was controller induced. We provided juice to subject 7 at 3:45 a.m. when she had a YSI value of 66 mg/dL and a rate of change of −0.25 mg/dL/min. Thus, the first cohort had a rate of glucose interventions of 0.75 per day, and the second had a rate of controller-induced interventions of about 0.125 per day.
The controller for the second cohort was specifically modified to provide better control, as noted in Methods above. Primarily, the improvements resulted in a 43 mg/dL average reduction in the overnight glucose levels and an associated reduction in the glycemic risk (Low Blood Glucose Risk Index+High Blood Glucose Risk Index) from 9.2 to 6.0. These changes were not statistically significant because of the small sample size.
The second cohort of patients had estimated HbA1c values of 7.3% and 6.6% based on their respective mean daily reference and CGM glucose values. 33 For reference, the mean HbA1c values for the conventional and intensive control groups in the Diabetes Control and Complications Trial were roughly 9% and 7%, respectively. 1 The American Association of Clinical Endocrinologists recommends a goal of achieving an HbA1c target of 6.5%, 34 whereas the American Diabetes Association recommends a goal of 7%. 3
Discussion
Meals are the primary challenge for automatic control of glucose levels in type 1 diabetes. Many studies have used hybrid control with meal announcement to address this issue. 9,10,24 Several groups have managed the transition from announced to unannounced meals by testing their controllers with small and/or isolated unannounced meals/snacks. 36 –38 This lessens the challenge of responding to meals by shrinking the size of the disturbance and/or ensuring no further unannounced meals before the meal response is complete. This is a sensible and safe testing regimen. We structured our study to challenge the system by having repeated, large unannounced meals separated by roughly 4 h. Although this 4-h separation serves to isolate the meals, there are still multiple cases where a meal starts before glucose levels have stabilized. We have adjusted our algorithm to anticipate future meals between 8 a.m. and 5 p.m. More research is necessary to ensure that we can be adequately aggressive while still safe in the instance of a skipped meal.
Research shows, however, that patients, particularly adolescents, often forget to deliver a meal bolus. 39,40 With a controller in place that would compensate for the meal disturbance, albeit less well, patients may be even less likely to announce their meals. As controllers improve, specifically when insulin acts more rapidly and sensors accuracy improves, the benefit of announcing meals will decrease.
When a patient is sleeping, his or her blood glucose levels are free from new meal disturbances. Most other disturbances, such as prior exercise, cause gradual changes in the blood glucose level. Although this allows for simpler, safer nocturnal controller designs, we need to manage the transitions between the daytime and nighttime regimens carefully. For instance, the response to the last meal of the day is inherently riskier because there are no more meals to counter an overly aggressive insulin response. Alternately, pressure-induced sensor attenuations at night 41 can cause large positive glucose slopes that could be detected improperly as meals (see patient 3 in Supplementary Data). Because meals primarily occur when the patient is upright and pressure-induced sensor attenuations when they are lying down, we would consider using an accelerometer to detect the orientation of the patient's torso. This would help us detect and remove pressure-induced sensor attenuation–affected CGM readings.
Conclusions
For the second cohort of six patients, the controller rejected repeated, large (1 g of carbohydrate/kg of patient weight), unannounced meals while maintaining mean reference and CGM 24-h glucose levels of 161 and 142 mg/dL, respectively. Assuming a reasonably well-calibrated CGM, this controller could potentially result in glucose levels that over a longer study would result in subjects meeting the 7% HbA1c target recommended by the American Diabetes Association. 35 It did this with a low rate of carbohydrate intervention (0.125 interventions per day).
We are continuing clinical development with addition trials in a controlled outpatient environment. We will improve the algorithm by relaxing the assumptions about the time of day for meals. Additionally, we are including accelerometer readings to indicate activity and sleep.
Footnotes
Acknowledgments
This research was supported by grants from the JDRF Artificial Pancreas Project (22-2006-1108, 22-2007-1801, 22-2009-795, and 3-2011-80) and the Stanford Clinical and Translational Science Award (CTSA) to Spectrum (UL1 TR001085). We also thank Mark Taub, PhD, Abbott Diabetes Care, Eyal Dassau, PhD, University of California, Santa Barbara Department of Chemical Engineering, and the subjects who so altruistically made these studies possible.
Author Disclosure Statement
B.A.B. is on the Medical Advisory Board for Metronic Minimed, Novo-Nordisk, and Sanofi. He has also received research support from Medtronic Minimed and Dexcom. F.C., G.N., D.M.W., B.W.B., K.S.B., and P.C. declare no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.