
Abstract
Background:
The accuracy of the Contour® Plus (Bayer HealthCare LLC, Diabetes Care, Whippany, NJ) blood glucose monitoring system (BGMS) was evaluated in two separate studies.
Materials and Methods:
In the laboratory study, fingerstick samples from 100 subjects were tested in duplicate using three test strip lots and assessed per International Organization for Standardization (ISO) 15197:2003, Section 7 (≥95% of results within ±15 mg/dL or ±20% of the reference result for samples with glucose concentrations <75 and ≥75 mg/dL, respectively) and ISO 15197:2013, Section 6.3 (≥95% of results within ±15 mg/dL or ±15% of the reference result for samples with glucose concentrations <100 and ≥100 mg/dL, respectively) accuracy criteria. In the clinical trial, 220 subjects with diabetes, naive to the BGMS, tested capillary glucose from fingertip and palm blood samples and completed an ease-of-use questionnaire. BGMS and YSI glucose analyzer results were compared.
Results:
In the laboratory study, 100% of results met ISO 15197:2003 and ISO 15197:2013 accuracy criteria. In the clinical trial, 100% and 99.1% of subject fingerstick results and 98.1% and 96.7% of subject palm results met ISO 15197:2003 and ISO 15197:2013 accuracy criteria, respectively. By Parkes Consensus Error Grid analysis, 100% of subject fingerstick results and 98.1% of subject palm results were within Zone A (remainder within Zone B). Questionnaire results showed most subjects found the BGMS easy to use.
Conclusions:
The Contour Plus BGMS meets ISO 15197:2003 and ISO 15197:2013 accuracy criteria in the laboratory and when used by untrained individuals.
Background
S
The Contour® Plus is a BGMS that has been developed for use with Contour Plus test strips (Bayer HealthCare LLC, Diabetes Care, Whippany, NJ), which utilize a flavin adenine dinucleotide–glucose dehydrogenase enzyme in combination with a proprietary electron mediator. The accuracy of the BGMS was assessed in two separate studies. In the laboratory study, the primary objective was to compare the analytical accuracy of the BGMS in the laboratory with both International Organization for Standardization (ISO) 15197:2003 and ISO 15197:2013 accuracy criteria. The primary objective of the clinical trial was to assess the accuracy of the BGMS with fingerstick blood based on ISO 15197:2003 accuracy criteria when used by subjects with diabetes who were naive to the system. Additional objectives included assessment of subject-obtained fingerstick results based on ISO 15197:2013 accuracy criteria; assessment of trial staff–obtained fingerstick, subject palm, and venous results based on ISO 15197:2003 and ISO 15197:2013 accuracy criteria; and obtaining subject feedback on the BGMS and the User Guide instructions.
Materials and Methods
Laboratory study: analytical accuracy (ISO 15197:2003, Section 7; ISO 15197:2013, Section 6.3)
The laboratory study was conducted in accordance with ISO 15197:2003, Section 7 and ISO 15197:2013, Section 6.3 requirements for system accuracy evaluations. Fingerstick capillary blood samples from 100 subjects were evaluated using three test strip lots, and each sample was tested in duplicate using six meters (two meters per test strip lot; n=600). The distribution of blood glucose concentrations of the samples used for the evaluation met the requirements of both the ISO 15197:2003 and ISO 15197:2013 standards. Most samples were tested fresh from the finger without modification; however, to obtain enough samples at the high (>400 mg/dL) and low (<50 mg/dL) end of the distribution, some of these capillary blood samples were modified to either a lower concentration (glycolyzed) or a higher concentration (supplemented with glucose). Samples were tested in parallel using a YSI 2300 STAT Plus™ glucose analyzer (YSI) (YSI Life Sciences, Inc., Yellow Springs, OH) as a laboratory reference. All testing was performed at 23±5°C (73.4±9°F).
Accuracy was assessed based on ISO 15197:2003, Section 7 criteria 14 (i.e., ≥95% of results shall fall within ±15 mg/dL of the mean YSI result for samples with glucose concentrations <75 mg/dL and ±20% for samples with glucose concentrations ≥75 mg/dL). Accuracy was also assessed based on ISO 15197:2013, Section 6.3 criteria 15 (i.e., ≥95% of results shall fall within ±15 mg/dL of the mean YSI result for samples with glucose concentrations <100 mg/dL and ±15% for samples with glucose concentrations ≥100 mg/dL). BGMS results were compared with YSI results using regression analysis and a modified Bland–Altman plot of the difference of BGMS results from the YSI results. The mean difference and mean percentage difference of BGMS results from the YSI results for samples with corresponding YSI values <100 mg/dL and ≥100 mg/dL, respectively, were also determined.
Clinical trial: user performance evaluation (ISO 15197, Section 8)
The clinical trial was conducted according to ISO 15197:2003 and ISO 15197:2013, Section 8 standards for user performance evaluations and enrolled people with type 1 or type 2 diabetes. Subject testing was conducted at two clinical sites between May 7, 2012, and May 22, 2012, in harmony with the World Medical Association Declaration of Helsinki (as amended), Good Clinical Practice standards, and requirements of Bayer HealthCare LLC, Diabetes Care. Potential subjects were recruited from the database at the Consumer Product Testing Company, Inc. (Fairfield, NJ) and the database at the Midwest Institute for Clinical Research (Indianapolis, IN).
Potential subjects meeting trial inclusion/exclusion criteria were given a verbal description of the risks and benefits of the trial. They were allowed to ask questions to which they received answers in terminology that they understood. Upon completion of the informed consent process, each potential subject executed an informed consent form by signing and dating the document. The potential subject then became a subject in the trial.
Subjects were excluded from the trial if they had previously participated in a trial using the BGMS, were employed in a clinical setting that involves training on and use of blood glucose monitors, were pregnant, had hemophilia or another bleeding disorder, or had any condition that in the opinion of the investigator would put the subject or trial conduct at risk. Subjects were also excluded if they, their immediate family member, or someone living in their household, was employed by a competitive medical device company. There were no exclusions for medications or supplements. During the single trial visit, prior to blood glucose testing, subjects were provided with the BGMS and the instructional materials (User Guide and Quick Reference Guide) and were given time to review the materials to learn how to use the system; subjects' review of the instructional materials was limited to the study site, and no additional training was provided. Subjects were randomly assigned to one of three test strip lots.
Subjects performed a fingerstick to test blood glucose on the meter; using a separate blood drop from the same fingerstick, trial staff then tested the subject's blood glucose with the BGMS. Subjects lanced and obtained blood from the palm for an alternative site testing blood glucose test using the BGMS. For both fingerstick and palm blood samples, subjects used a Microlet®2 lancing device (Bayer HealthCare LLC, Diabetes Care) and were requested to use a deeper setting on the lancing device to obtain more blood. All BGMS results for fingerstick and palm samples were compared with laboratory reference results from the YSI laboratory glucose analyzer using plasma from a trial staff–obtained fingerstick. In addition, trial staff drew venous blood from subjects for testing on the BGMS. This venous sample was also tested on the YSI for comparison with the venous result obtained using the BGMS. Accuracy was assessed based on ISO 15197:2003 accuracy criteria and ISO 15197:2013 accuracy criteria. Per-protocol analyses included modified Bland–Altman plots and Parkes Consensus Error Grid analysis. 16 Additional analyses, which were not prespecified in the protocol, included mean difference for subject-obtained capillary fingerstick samples with corresponding YSI values <100 mg/dL, as well as mean percentage difference for subject-obtained capillary fingerstick samples with corresponding YSI values ≥100 mg/dL.
After blood glucose testing, subjects completed a questionnaire on the BGMS and instructions for use. Possible responses to the questions on the subject questionnaire were based on a 5-point Likert scale: 1 (strongly disagree), 2 (disagree), 3 (neutral), 4 (agree), and 5 (strongly agree).
Results
Laboratory study: analytical accuracy (ISO 15197:2003, Section 7; ISO 15197:2013, Section 6.3)
In total, 600 BGMS results were obtained by testing 100 capillary blood samples. The plasma glucose concentration of the blood samples ranged from 22 mg/dL to 548 mg/dL, and the hematocrit ranged from 32% to 54%.
Analysis of BGMS results based on ISO 15197:2003, Section 7 accuracy criteria showed that 100% (600/600) of results were within ±15 mg/dL or ±20% of the YSI result for samples with glucose concentrations <75 mg/dL and ≥75 mg/dL, respectively. Also, 100% (78/78) of the results for samples with glucose concentrations <75 mg/dL were within ±10 mg/dL of the YSI result and 99.4% (519/522) of the results for samples with glucose concentrations ≥75 mg/dL were within ±10% of the YSI result (Table 1).
ISO 15197:2003, Section 7 accuracy criteria.
ISO 15197:2013, Section 6.3 accuracy criteria.
Analysis of BGMS results based on ISO 15197:2013, Section 6.3 accuracy criteria showed that 100% (600/600) of results were within ±15 mg/dL or ±15% of the YSI result for samples with glucose concentrations <100 mg/dL and ≥100 mg/dL, respectively. Furthermore, 100% (198/198) of the results for samples with glucose concentrations <100 mg/dL were within ±10 mg/dL of the YSI result and 99.5% (400/402) of the results for samples with glucose concentrations ≥100 mg/dL were within ±10% of the YSI result (Table 1).
Regression analysis confirmed strong agreement between BGMS results and YSI results (Fig. 1). A modified Bland–Altman plot of the difference of BGMS results from YSI results is shown in Figure 2A. The mean difference and mean percentage difference of BGMS results from the YSI results were 2.66 mg/dL and 2.37% for samples with corresponding YSI values <100 mg/dL (n=198) and ≥100 mg/dL (n=402), respectively.
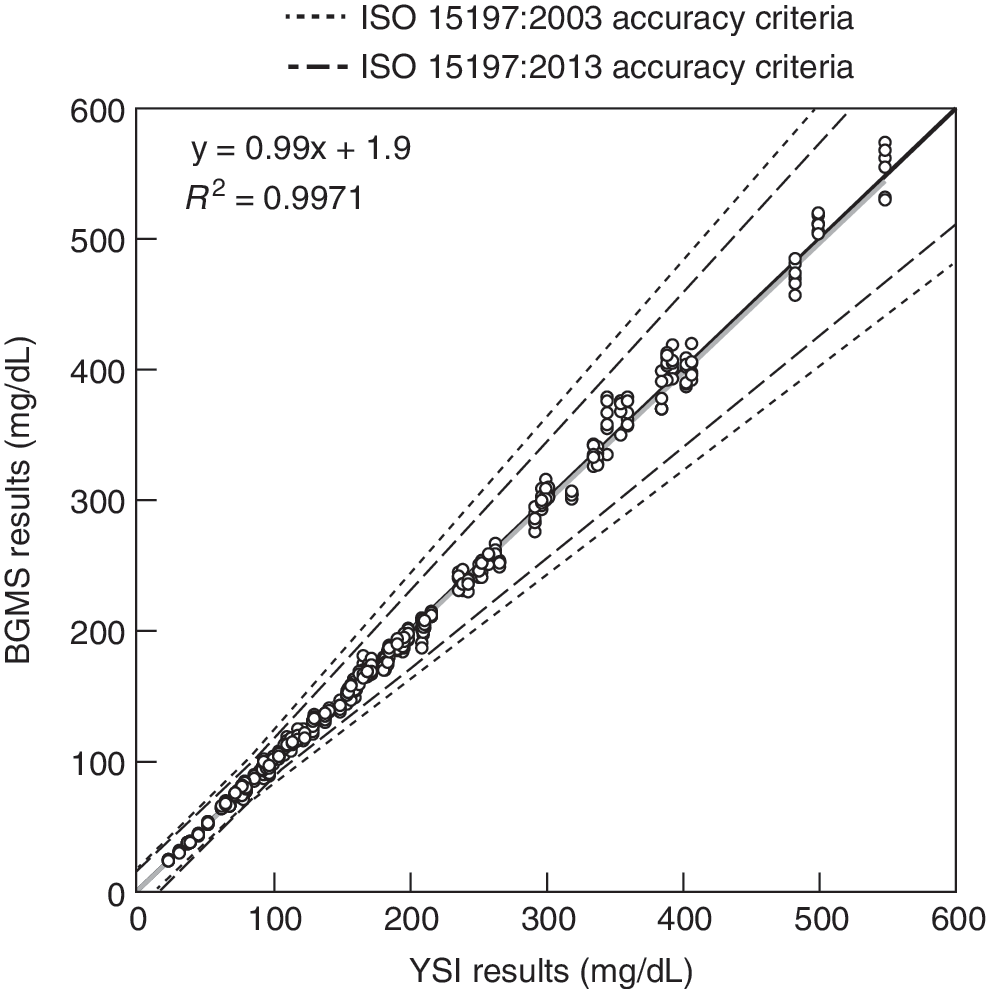
Regression analysis of blood glucose monitoring system (BGMS) results from the laboratory study compared with YSI glucose analyzer (YSI) results (International Organization for Standardization [ISO] 15197:2003, Section 7; ISO 15197:2013, Section 6.3). The gray line denotes the regression line.
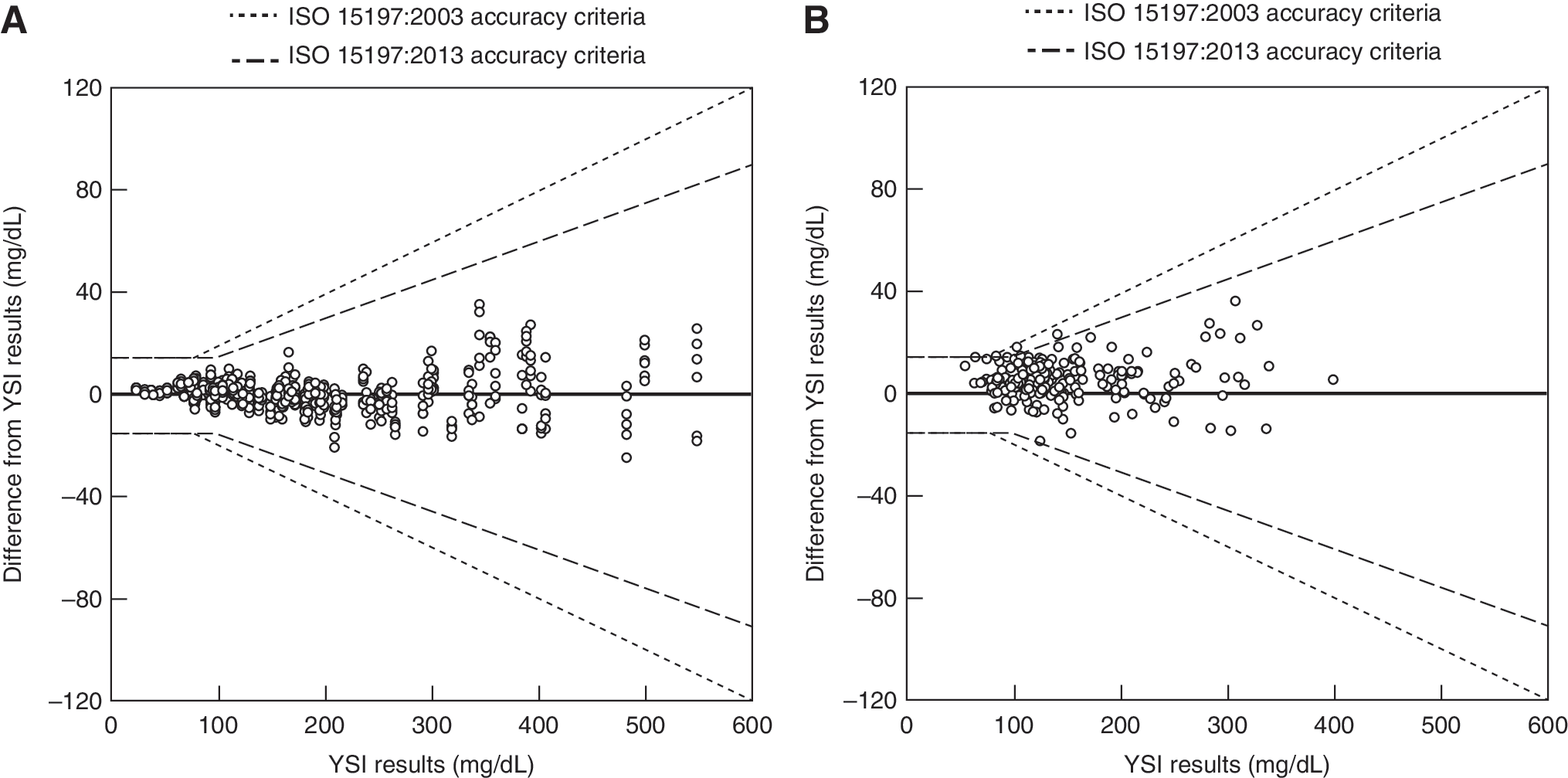
Difference of blood glucose monitoring system results from YSI glucose analyzer (YSI) results for
Clinical trial: user performance evaluation (ISO 15197, Section 8)
Subjects
In total, 220 subjects 26–86 years of age (mean, 60 years) were enrolled and qualified for the clinical trial. There were slightly more females (54%). Most subjects had type 2 diabetes (n=185), 32 had type 1 diabetes, and three subjects had diabetes of unknown type. The race of the subject panel was approximately two-thirds white and approximately one-third black/African American. The subjects' duration of diabetes ranged from less than 1 month to more than 10 years, with the vast majority (98%) being more than 1 year. The majority of subjects (75%) tested their blood glucose one to three times daily; nine (4%) subjects reported that they did not test their blood glucose, 18 (8%) tested less than one time per day, and 28 (13%) tested four or more times per day.
Fingerstick results were analyzed from 216 subjects for self-testing and from 217 subjects for trial staff testing; 213 subjects had results from palm and venous blood testing. The glucose concentration of the subjects' blood samples, as measured by YSI, ranged from 53 mg/dL to 399 mg/dL for fingertip blood and from 52 mg/dL to 386 mg/dL for venous blood. Hematocrit measurements were performed in duplicate for each subject; average hematocrit values for each subject ranged from 18% to 51%, with a mean of 40%.
Accuracy
Evaluation of capillary fingerstick results showed that 100% (216/216) of subject-obtained results and 99.5% (216/217) of trial staff–obtained results met the ISO 15197:2003 accuracy criteria. Furthermore, 99.1% (214/216) of subject- and 99.1% (215/217) of trial staff–obtained capillary fingerstick results met the ISO 15197:2013 accuracy criteria. Evaluation of subject palm results showed that 98.1% (209/213) of results met the ISO 15197:2003 accuracy criteria and that 96.7% (206/213) of results met the ISO 15197:2013 accuracy criteria. For venous blood testing, 99.5% (212/213) of results met the ISO 15197:2003 accuracy criteria, and 99.5% (212/213) of results met the ISO 15197:2013 accuracy criteria. The percentage of BGMS results that fell within specific error limits of the YSI result for each sample type is shown in Table 2.
Within the International Organization for Standardization (ISO) 15197:2003 accuracy criteria.
Within the ISO 15197:2013 accuracy criteria.
YSI, YSI glucose analyzer.
A modified Bland–Altman plot of the difference of BGMS results from YSI results for subject-obtained capillary fingerstick samples is shown in Figure 2B. In addition, these differences were quantified using several analyses; for subject-obtained capillary fingerstick samples with a YSI measurement <100 mg/dL (n=49), the mean difference was 4.16 mg/dL, and for samples with a YSI measurement ≥100 mg/dL (n=167), the mean percentage difference was 3.68%.
By Parkes Consensus Error Grid analysis, 100% (216/216) of subject-obtained capillary fingerstick results and 100% (217/217) of trial staff–obtained capillary fingerstick results were within Zone A. Furthermore, 98.1% (209/213) of subject palm results were within Zone A, with the remainder within Zone B. For venous samples, 99.5% (212/213) of results were within Zone A, and one result was within Zone C. The single venous result within Zone C was due to an unknown cause.
Subject questionnaire
Based on ease-of-use questionnaire results, most subjects agreed or strongly agreed that “I find it easy to do a fingerstick blood test with this meter” (96.8%), “The instructions (User Guide and Quick Reference Guide) were easy to understand” (98.2%), “The meter display is easy to see and read (the test result)” (99.6%), and “It was easy to understand my test results” (99.5%) (Fig. 3).
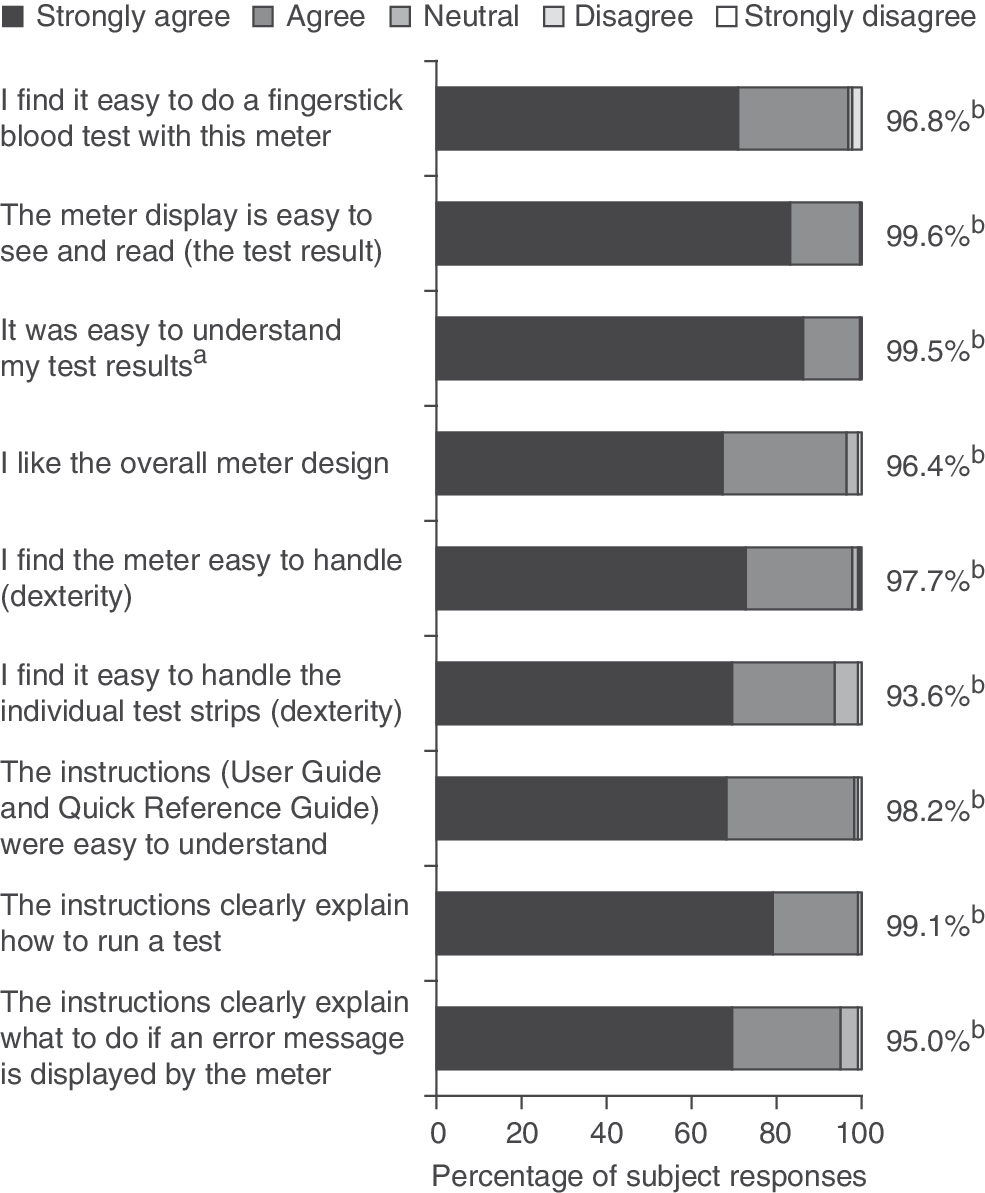
Results of the ease-of-use questionnaire from the clinical trial (International Organization for Standardization 15197, Section 8; n=220). a n=218. bSubjects responding “strongly agree” or “agree.”
Safety
There were two non-serious, non–device-related adverse events: one hypoglycemic event and one hyperglycemic event. The subject who experienced hypoglycemia was withdrawn from the trial. The adverse events were anticipated, considered mild, and resolved before the subjects left the trial site.
Discussion
Blood glucose results from SMBG are used by people with diabetes and their healthcare providers to make decisions about lifestyle modifications, including meal planning and physical activity, as well as to adjust treatment, such as insulin dose. 6,7 Inaccurate blood glucose results can lead to administration of an incorrect insulin dose or failure to treat hypoglycemia or hyperglycemia. 8,9 Therefore, it is important to use a BGMS that reliably produces accurate results. 10 The ISO issues criteria for the assessment of BGMS accuracy to be used by regulatory authorities responsible for evaluating the performance of these systems. New, more stringent criteria were recently issued by the ISO based on input from medical experts and reflecting improvements in technology. The laboratory study and the clinical trial compared the accuracy of the BGMS against both ISO 15197:2003 and the new ISO 15197:2013 accuracy criteria. In addition to analytical accuracy of the BGMS itself, there are other factors that can also contribute to the accuracy of SMBG results. 6,11,12 For example, ease of use is an important consideration because the accuracy of blood glucose results can be affected by user technique. 6,11,12
The BGMS evaluated in the two studies described herein demonstrated accuracy and ease of use. In the laboratory study, the BGMS met and exceeded both ISO 15197:2003 and ISO 15197:2013 accuracy criteria, with 100% of results falling within the specified limits. Furthermore, 99.5% of results were within ±10 mg/dL or ±10% of the YSI result for all samples. In the clinical trial, >96% of BGMS results using capillary fingerstick, palm, or venous blood samples met and exceeded both ISO 15197:2003 and ISO 15197:2013 accuracy criteria. The accuracy of the results was similar whether the system was being used by trial staff or by people with diabetes who had no prior experience with the BGMS. Similar accuracy profiles were also obtained in the hands of untrained users and in the laboratory, as shown by a graphical comparison of results under these two sets of conditions (Fig. 2). Together, these results suggest that the BGMS is easy for a lay person with diabetes to use, without any training other than the User Guide. Based on questionnaire results, the majority of subjects in the clinical trial rated the ease of use of the BGMS favorably.
The clinical trial included a Parkes Consensus Error Grid analysis to assess the clinical significance of inaccuracies in SMBG measurements. This analysis assigns a level of risk to each possible SMBG error, as judged by a large group of endocrinologists, and reflects the absolute value of both the measured and reference blood glucose values. 16 Out of five levels of clinical risk, increasing in severity from Zone A through Zone E, the results of this trial showed that nearly all subject-obtained measurements with the BGMS were within Zone A and that none were in Zone C, D, or E; thus, any inaccuracies presented minimal clinical risk.
In conclusion, accuracy and ease of use are important considerations for people who use SMBG to manage their diabetes, and the results of these studies demonstrate both qualities in the BGMS evaluated. The laboratory study demonstrated analytical accuracy, and the clinical trial showed a high level of accuracy in the hands of subjects with diabetes who had no prior experience with the system. The clinical trial also demonstrated the ease of use of the BGMS, based on the finding that subjects with diabetes with no prior experience with the BGMS were able to use the system to obtain accurate results, as well as the questionnaire results, which showed that the majority of subjects felt that the BGMS was easy to use.
Footnotes
Acknowledgments
These studies were supported by Bayer HealthCare LLC, Diabetes Care, Whippany, NJ. We would like to thank Phillip D. Toth, MD, and his site, the Midwest Institute for Clinical Research, for their participation in the clinical trial. We would also like to thank Jane F. Wallace, of Bayer, for her contributions to the clinical trial and the manuscript. Medical writing assistance was provided by Allison Michaelis, PhD, of MedErgy, Yardley, PA, and was supported by Bayer HealthCare LLC, Diabetes Care.
Author Disclosure Statement
S.P., N.D., M.E.W., and R.M. are full-time employees of Bayer HealthCare LLC, Diabetes Care. M.T.V. was a full-time employee of Bayer HealthCare LLC, Diabetes Care at the time of the study. M.C. and J.F. are full-time employees of Consumer Product Testing Company, Inc.
J.F. and M.C. contributed to the development of the clinical trial protocol and were responsible for the conduct of the clinical trial. M.T.V. contributed to the acquisition and interpretation of data for the clinical trial. S.P. wrote the statistical analysis plan and performed the statistical analyses for the clinical trial. N.D. contributed to the interpretation of data for the work. M.E.W. contributed to the acquisition and analysis of data for the laboratory study. R.M. reviewed, revised, and approved the study protocol. All authors revised the manuscript and approved the final version to be published.