
Abstract
Objectives:
This study assessed the relationship between diabetic retinopathy (DR) and coronary artery diseases (CAD) in Asian Indians, who are known to be at high risk of CAD and diabetes but have lower prevalence of DR.
Subjects and Methods:
Type 2 diabetes subjects (n=1,736) were selected from the urban component of the population-based Chennai Urban Rural Epidemiology Study Eye Study. Four-field stereo retinal color photography was done, and DR when present was classified according to the Early Treatment Diabetic Retinopathy Study grading system. Among the 1,723 subjects with gradable fundus photographs, 12-lead electrocardiogram (ECG) was performed in 1,602 individuals, and analysis was restricted to this group. CAD was diagnosed based on documented medical history of CAD or Minnesota coding of ECGs.
Results:
The prevalence of CAD was significantly higher among subjects with DR compared with those without (11.3% vs. 6.7%; P=0.007). A significant association was observed between DR and CAD in subjects with glycated hemoglobin (HbA1c) levels >7% (P=0.002). After controlling for age and gender, only hard exudates were associated with CAD (P=0.032). Logistic regression analysis revealed that even after adjusting for age, gender, HbA1c, mean arterial blood pressure, smoking, serum cholesterol, triglyceride, and low-density lipoprotein cholesterol levels, DR was significantly associated with CAD among the study subjects (odds ratio [OR]=1.58; 95% confidence interval [CI], 1.00–2.49; P=0.049) and those subjects with duration of diabetes >10 years (OR=4.06; 95% CI, 1.55–10.60; P=0.004).
Conclusions:
This cross-sectional study shows a significant association between DR and CAD in South Indian subjects with type 2 diabetes.
Introduction
T
Asian Indians have increased susceptibility to type 2 diabetes 9 and have two- to fourfold higher rates of premature coronary artery disease (CAD) compared with whites. 10 However, the overall prevalence of DR as well as the prevalence of DR at diagnosis was lower in Asian Indians compared with whites. 11 –13 In view of the lower prevalence of DR and higher prevalence of CAD in Asian Indians, we thought it worthwhile to study the relationship between DR and CAD in this ethnic group.
Subjects and Methods
Study subjects were recruited from the urban component of the Chennai Urban Rural Epidemiology Study (CURES), an ongoing epidemiological study conducted on a representative population of Chennai (formerly Madras) in South India. The methodology of CURES has been published earlier. 14 In brief, in Phase 1 of the urban component of CURES, 26,001 individuals >20 years of age were selected by a systematic sampling technique from 46 randomly selected corporation wards of Chennai and screened for diabetes. Fasting capillary blood glucose was determined using a glucose meter (OneTouch® Basic; LifeScan, a Johnson & Johnson Company, Milpitas, CA) in all subjects. Self-reported diabetes subjects who were diagnosed by a physician or who were on diet and drug treatment for their diabetes were classified as “known diabetes subjects” (KD subjects).
In Phase 2 of CURES, all the KD subjects (n=1,529) were invited to the Center for detailed studies on vascular complications during the years 2003 and 2004. In addition, 15% of subjects with impaired fasting glucose and 10% of subjects with normal fasting glucose in Phase 1 were requested to undergo an oral glucose tolerance test. Thirty-seven of the former group and 14 of the latter group who were found to have diabetes according to World Health Organization Consulting Group criteria (2-h plasma glucose ≥200 mg/dL) 15 were added to the 320 randomly chosen newly detected diabetes (NDD) subjects from Phase 1 of the study. Of the total 371 NDD subjects, 354 consented for this study (response rate, 95.4%). Of the total 1,529 KD subjects, 1,382 (90.4%) participated in this study, in addition to the 354 NDD subjects, making a total of 1,736 diabetes subjects (1,382 KD+354 NDD). Institutional ethics committee approval was obtained, and informed consent was obtained from all study subjects.
Clinical and biochemical studies
Anthropometric measurements, including weight, height, and waist measurements, were obtained using standardized techniques. The body mass index was calculated using the definition of weight (kg)/height (m2). Blood pressure was recorded in the sitting position in the right arm to the nearest 2 mm Hg with a mercury sphygmomanometer (Diamond Deluxe Industrial Electronic and Products, Electronic Co-op Estate, Pune, India). Two readings were taken 5 min apart, and the mean of the two was taken as the final blood pressure reading of the individual.
A fasting blood sample was taken after ensuring 8-h overnight fasting for estimation of levels of plasma glucose and serum lipids using a Hitachi 912 Autoanalyzer (Roche Diagnostics GmbH, Mannheim, Germany) with kits supplied by Boehringer Mannheim (Mannheim). Fasting plasma glucose (glucose oxidase–peroxidase method), serum cholesterol (cholesterol oxidase–phenol–4-aminophenazone–peroxidase method), serum triglycerides (glycerol-3-phosphate peroxidase–phenol–4-aminophenazone–peroxidase method), and high-density lipoprotein cholesterol (by the direct method; polyethylene glycol–pretreated enzymes) were measured. Low-density lipoprotein cholesterol was calculated using the formula of Friedewald et al. 16 Non–high-density lipoprotein cholesterol was calculated by subtracting the high-density lipoprotein cholesterol from the total cholesterol. Glycated hemoglobin (HbA1c) was measured by the high-pressure liquid chromatography method using the Variant™ machine (Bio-Rad, Hercules, CA).
Ocular examination
A comprehensive ocular examination was done on all study subjects. Visual acuity was recorded using an illuminated Snellen's chart by trained optometrists. The pupils were dilated with one drop of phenylepherine (10%) and tropicamide (1%) in both eyes. Four-field stereo color retinal photography was carried out by trained and certified photographers using a Zeiss (Oberkochen, Germany) FF 450 plus camera and 35-mm color transparencies. The photographs were coded using an identification number and assessed in a masked manner.
Photographs were assessed and assigned a retinopathy level, and the final diagnosis for each patient was determined from the grading of the worse eye according to the Early Treatment Diabetic Retinopathy Study criteria for severity of individual eye. Retinopathy was present if any of the following lesions was graded definite or probable: blot hemorrhages, flame-shaped hemorrhages, microaneurysms, soft exudates (cotton-wool spots), hard exudates, macular edema, new vessels, intraretinal microvascular abnormalities, and other less common lesions. In brief, level 10 represents no retinopathy (no DR), levels ≥20 through <60 represent nonproliferative DR (NPDR) (level ≥20, mild NPDR; levels ≥30 to <50, moderate NPDR; and levels ≥50 to <60, severe NPDR), and levels ≥60 represent proliferative DR (PDR). 17
Electrocardiogram
A resting 12-lead electrocardiogram (ECG) was carried out, and Minnesota coding 18 was used to grade the ECG by a single trained grader who was blinded to the clinical status of the patient.
Definitions
Diabetes was diagnosed if subjects were on drug treatment for diabetes (insulin or oral hypoglycemic agents) and/or fulfilled the criteria laid down by the World Health Organization Consulting Group report (i.e., a fasting venous blood glucose level of ≥126 mg/dL and/or a 2-h postglucose value of ≥200 mg/dL). 15
Hypertension was diagnosed if subjects were on drug treatment for hypertension or if systolic blood pressure was ≥140 mm Hg and/or diastolic blood pressure was ≥90 mm Hg. 19
Mean arterial blood pressure was defined as D+(S – D)/3, where S is systolic blood pressure and D is diastolic blood pressure.
CAD was diagnosed based on positive medical history (documented myocardial infarction, coronary artery bypass graft, or angioplasty) or angina pectoris confirmed by ischemic changes on a conventional 12-lead ECG that included ST-segment depression (Minnesota codes 1-1-1 to 1-1-7). 20
Individuals were classified as nonsmokers and current smokers.
Statistical analysis
Numbers were expressed as mean±standard deviation. One-way analysis of variance (with post hoc Tukey's analysis) was used to compare groups for continuous variables, and the χ2 test was used to compare proportions among groups. Logistic regression analysis was done using CAD as the dependent variable. Different models were constructed using multivariate regression analysis to determine the association of DR and CAD by adjusting for other risk variables that have been reported to have an association with both DR and CAD. To assess the risk of CAD in relation to severity of DR, severe NPDR and PDR were combined together as the numbers of subjects in each group were very small (n=9 and 15, respectively). P<0.05 was considered significant. All analysis was done using a Windows-based SPSS statistical package (version 10.0; SPSS, Inc., Chicago, IL).
Results
Of the 1,736 diabetes subjects recruited for the study, fundus photographs were not available in 21 subjects because of various reasons, which included opacities in the ocular media, inability to cooperate, or refusal. Of the subjects for whom retinal photographs were ungradable, retinal photography was repeated, and eight subjects were included. Thus, in total, 1,723 subjects with gradable photographs were included for analysis. Of these, the ECG could not be done in 121 subjects primarily because of refusal to undergo ECG. Hence, in total, 1,602 subjects (response rate, 83.4%) finally participated in this study, which included 1,275 KD and 327 NDD subjects. There were no significant differences between the 1,602 “participants” and the 134 “nonparticipants”: age, 51±11 versus 52±12 years (P=0.234); men, 44.6% versus 50.0% (P=0.240); fasting plasma glucose, 162±72 versus 162±54 mg/dL (P=0.513); systolic blood pressure, 129±21 versus 130±24 mm Hg (P=0.637); and diastolic blood pressure, 77±12 versus 77±12 mm Hg (P=0.872).
The overall prevalence of CAD among the diabetes subjects was 7.6% (11.6% of subjects were diagnosed with CAD on the basis of ECG abnormalities alone). The prevalence of CAD was higher among subjects with DR compared with those without DR (11.3% vs. 6.7%; P=0.007). The prevalence of CAD was 10.7% in those with mild NPDR, 11.8% in subjects with moderate NPDR, and 12.5% in those with severe DR (inclusive of severe NPDR and PDR). There was an increasing trend in prevalence of CAD with severity of DR (trend χ2=6.946; P=0.008) (Fig. 1). It was observed that none of the NDD subjects with CAD had DR in this study population.
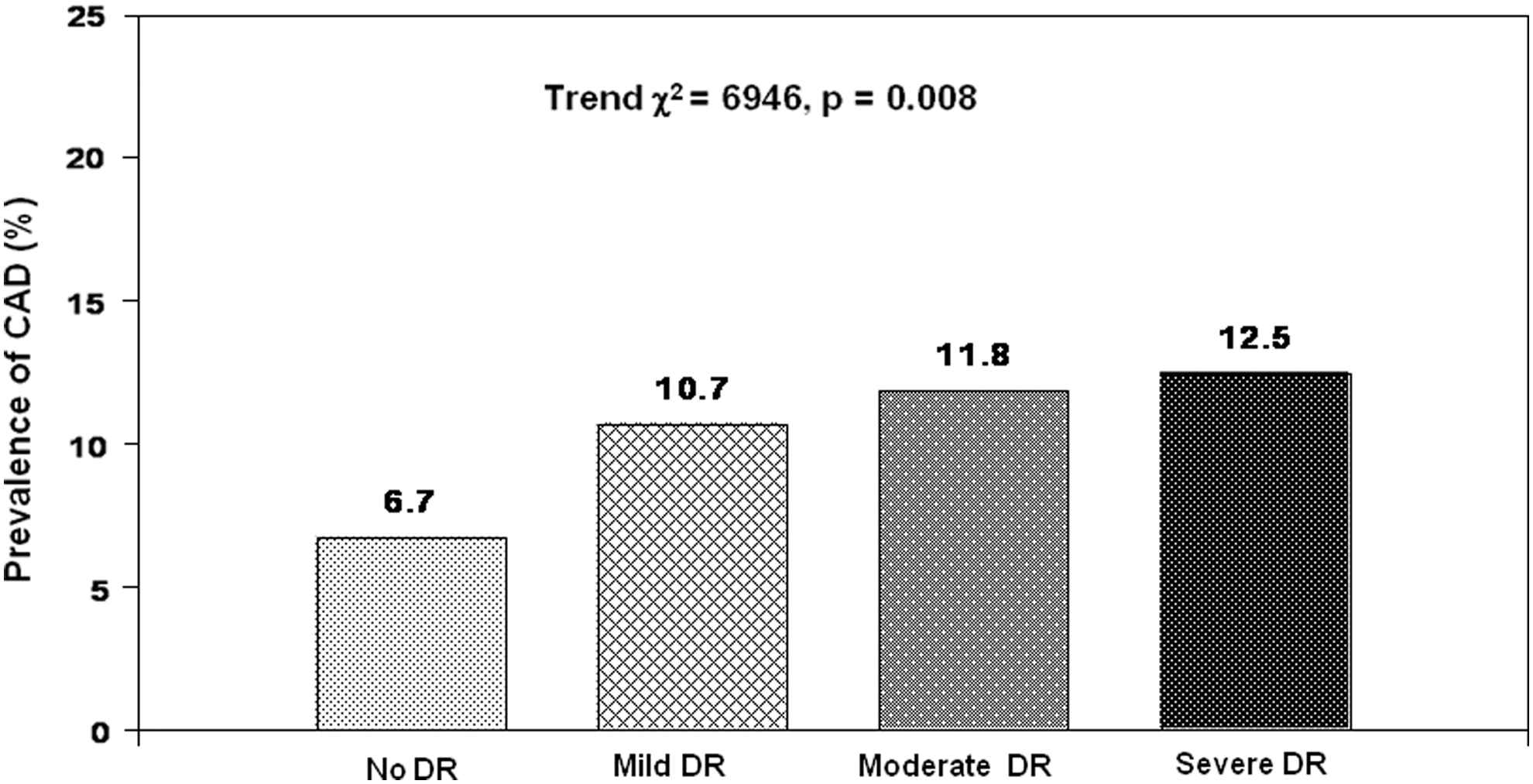
Prevalence of coronary artery disease (CAD) according to severity of diabetic retinopathy (DR).
Table 1 compares the clinical and biochemical characteristics of study subjects. Compared with the no DR group, DR subjects with CAD were older (P<0.001), had greater duration of diabetes (P<0.001), lower body mass index (P<0.05), and higher fasting blood sugar (P<0.05) and HbA1c (P<0.001), and included a higher proportion of subjects with hypertension (P<0.05) and on insulin therapy (P<0.001). Similarly, DR subjects without CAD were also older (P<0.05), had greater duration of diabetes (P<0.001), lower body mass index (P<0.001), higher fasting blood sugar (P<0.001) and HbA1c (P<0.001), and high triglycerides (P<0.001), and included a higher proportion of subjects on oral hyperglycemic agents and insulin therapy (P<0.001) compared with the no DR group.
Data are mean±SD values, unless otherwise indicated.
Analysis of variance P for continuous variables and P for trend for categorical variables.
P<0.001, c P<0.05 compared with the no diabetic retinopathy group.
P<0.001, e P<0.05 compared with the diabetic retinopathy without CAD group.
BMI, body mass index; BP, blood pressure; CAD, coronary artery disease; HDL, high-density lipoprotein; LDL, low-density lipoprotein; OHA, oral hyperglycemic agent.
Table 2 shows the prevalence and association of clinical characteristics with CAD and DR. The prevalence of CAD and DR was significantly higher among subjects >50 years of age, of male gender, who had hypertension, and who had HbA1c levels >7%. Logistic regression analysis revealed that, when stratified according to age, gender, hypertension status, and glycemic control, a significant association was observed between DR and CAD in those without hypertension (odds ratio [OR]=2.15; 95% confidence interval [CI], 1.03–4.47; P=0.04) and in subjects with an HbA1c level >7% (OR=1.77; CI, 1.13–2.76; P=0.002).
Dependent variable, coronary artery disease (CAD); independent variable, diabetic retinopathy (DR).
P value indicates a significant difference.
CI, confidence interval; HbA1c, glycated hemoglobin; OR, odds ratio.
Table 3 depicts the association of different lesions of diabetic retinopathy with CAD. Prevalence of CAD was significantly higher in those with microaneurysms/dot and blot hemorrhages (11.8% vs. 7.0%) and hard exudates (13.5% vs. 7.0%) compared with those without these lesions. In subjects with new vessels and fibrous proliferans, the prevalence of CAD was higher compared with those without these lesions (11.1% vs. 7.5%); however, the difference did not reach statistical significance. Among the different DR lesions, microaneurysms/dot and blot hemorrhages and hard exudates were independently associated with CAD. However, only hard exudates were significantly associated with CAD after controlling for age and gender (OR=1.85; 95% CI, 1.06–3.25; P=0.03).
Dependent variable, coronary artery disease (CAD).
P value indicates a significant difference.
Cl, confidence interval; OR, odds ratio.
To evaluate the association of DR with CAD, models were developed based on logistic regression using CAD as the dependent variable, and various factors associated with CAD on univariate regression analysis were included as independent variables. Table 4 shows that after adjustment for various risk factors, DR was associated with CAD (Model 1: OR=1.58; 95% CI, 1.002–2.490; P=0.049). When the association between DR and CAD was assessed among subjects with duration of diabetes ≤10 years and >10 years, it was observed that association of DR with CAD persisted only in subjects with diabetes duration >10 years (OR=4.06; 95% CI, 1.55–10.60; P=0.004) after adjustment for various risk factors.
Data are odds ratio (95% confidence interval); P value.
Dependent variable, coronary artery disease.
P value indicates a significant difference.
HbA1c, glycated hemoglobin; LDL, low-density lipoprotein.
Discussion
This cross-sectional study shows that there is an association between DR and CAD in urban South Indian type 2 diabetes subjects, which persisted even after adjusting for age, gender, HbA1c, mean arterial blood pressure, smoking status, and serum lipids. This association was stronger among subjects with duration of diabetes >10 years. In an earlier study we had shown that there was an association between DR and carotid intimal medial thickness in the same CURES population. 21 The association of DR with clinical CAD seen in this study as well as with early atherosclerosis as assessed by intimal medial thickness in our earlier study suggests that there could be common pathogenic mechanisms between DR and macrovascular complications like CAD. As the prevalence of retinopathy is lower in Indians 11 and the prevalence of CAD is high, 22 looking at the relationship between these two in an epidemiological setting is of great interest.
Previous epidemiological studies have reported that patients with DR have a higher proportion of CAD and have a high risk of mortality from CAD. 5,7,8 An increased rate of cardiac events in patients with DR was demonstrated in a prospective follow-up study. 6 In this cross-sectional study, the prevalence of CAD was lower (33/291, 11.3%) among subjects with DR than that reported in the Cardiovascular Health Study (25/60, 41.7%). 23 This could be due to the younger age cutoff used in our study (≥20 years) and the inclusion of both KD and NDD. Although our earlier studies have reported lower prevalence of DR in our population, 12 DR still remains the leading cause of blindness among those of working age and hence requires clinical intervention right from the earlier stages, including screening for CAD to prevent/reduce the consequent morbidity and mortality. 24
Many studies have looked at the association of severity of DR with cardiovascular disease in western populations. 6,8,23 It has been elegantly demonstrated in the EURODIAB prospective complications study that type 1 diabetes subjects with NPDR or PDR have an increased risk for cardiovascular disease. 4 The Wisconsin Epidemiologic Study of Diabetic Retinopathy showed that in type 1 diabetes subjects, the severity of DR was associated with increased heart disease mortality. 25 Miettinen et al. 26 in Finnish type 2 diabetes individuals have reported that PDR was significantly associated with coronary heart disease events even after controlling for other cardiovascular risk factors. However, in the Atherosclerosis Risk in Communities study, severity of DR was not cross-sectionally associated with CAD in type 2 diabetes subjects. 27 This is consistent with our findings where there was an increasing trend in the prevalence of CAD with the severity of DR in type 2 diabetes subjects; however, the association with CAD was not significant, likely because of insufficient events. A recent report in a Japanese population has shown a significant association of proliferative retinopathy with CAD after accounting for several confounders. 28 Further studies have also consistently established that retinopathy underlies and exaggerated risk of coronary heart disease. 29,30
There were significant associations between DR and CAD in those with an HbA1c level of ≥7% and without hypertension, when stratified according to age, gender, glycemic control, and hypertension status. It is surprising that among our type 2 diabetes population we found a significantly higher OR for association of DR with CAD in normotensive subjects (OR=2.15) than in those with hypertension (OR=1.6); however, this was not statistically significant. One of the reasons for lack of association of DR and CAD among hypertensive subjects in this study could be that systolic and mean arterial blood pressures were not major risk factors for DR in this relatively young population with diabetes.
To our knowledge there are no previous reports on the association of CAD and DR in Asian Indians who are at high risk for diabetes and CAD. 31 Lesions seen in DR (e.g., microaneurysms, retinal hemorrhages, soft and hard exudates) are structural evidence of microvascular damage from various processes. 32 Studies in western populations have shown that retinal lesions predict future cardiovascular events, independent of measured risk factors. 33,34 This is inconsistent with our study in which only hard exudates were found to be associated with CAD independent of age and gender.
Some studies have reported that DR had an independent association with CAD. 6,35 The fact that CAD was associated with DR even after adjusting for other well-known factors for CAD like age, male gender, HbA1c, mean arterial blood pressure, smoking status, serum cholesterol, triglyceride, and low-density lipoprotein cholesterol shows that DR seems to have an independent association with CAD, which is consistent with other reported studies. 6,35 In addition, DR was associated with CAD among those with longer duration of diabetes (>10 years) in this study after adjusting for various risk factors. It is well known that microangiopathy 36 and, to a lesser extent, macroangiopathy 37 are dependent on the duration of diabetes. Studies have also shown that duration of diabetes is a risk factor for both DR 38,39 and CAD. 40,41 These observations, in conjunction with ours, support the concept that DR and CAD are dependent on duration of diabetes beyond the shared risk factors adjusted for in our multivariate models. Any conclusions regarding these associations must be made with caution as this is a cross-sectional study.
The strengths of this study are that it is population-based and conducted on a large representative sample in urban South India. It is also the first study to look at the association between CAD and DR in Asian Indians, a population with high prevalence of the former and lower prevalence of the latter. The limitation of this study is that being a cross-sectional one, no conclusions can be drawn with respect to a cause and effect relationship between DR and CAD. Hence we cannot directly extrapolate our findings to an early detection of CAD in subjects with retinopathy until longitudinal data are available from this population. Another limitation in this study is the use of ECG to define CAD, as ECG changes are often not specific to CAD and ECG is also not sensitive enough to pick up subclinical CAD.
In conclusion, this cross-sectional study shows that DR is associated with CAD in this urban South Indian type 2 diabetes population despite lower prevalence of the former and higher prevalence of the latter in Asian Indians, compared with whites.
Footnotes
Acknowledgments
We gratefully acknowledge the late Dr. M. Rema, Managing Director and Chief Ophthalmologist, Dr. Mohans Diabetes Specialities Centre, for initiating the CURES EYE Study, our epidemiology team for their untiring efforts in the field work, and the eye technicians for retinal photographs. This is the 3rd publication from the CURES Eye Study and the 101st publication from CURES (CURES-101).
Author Disclosure Statement
No competing financial interests exist.