
Abstract
Background:
Diabetes self-management education is a cornerstone of successful diabetes management. Various methods have been used to reach the increasing numbers of patients with diabetes, including Internet-based education. The purpose of this article is to review various delivery methods of Internet diabetes education that have been evaluated, as well as their effectiveness in improving diabetes-related outcomes.
Materials and Methods:
Literature was identified in the Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, Medline, EBSCO, the Cochrane Library, and the Web of Science databases through searches using the following terms: “type 2 diabetes AND internet/web based AND education” and “type 2 diabetes AND diabetes self-management education (DSME) AND web-based/internet OR technology assisted education.” The search was limited to English language articles published in the last 10 years. The search yielded 111 articles; of these, 14 met criteria for inclusion in this review. Nine studies were randomized controlled trials, and study lengths varied from 2 weeks to 24 months, for a total of 2,802 participants.
Results:
DSME delivered via the Internet is effective at improving measures of glycemic control and diabetes knowledge compared with usual care. In addition, results demonstrate that improved eating habits and increased attendance at clinic appointments occur after the online DSME, although engagement and usage of Internet materials waned over time. Interventions that included an element of interaction with healthcare providers were seen as attractive to participants.
Conclusions:
Internet-delivered diabetes education has the added benefit of easier access for many individuals, and patients can self-pace themselves through materials. More research on the cost-benefits of Internet diabetes education and best methods to maintain patient engagement are needed, along with more studies assessing the long-term impact of Internet-delivered DSME.
Introduction
D
Diabetes management requires a complex combination of medication, nutritional, and lifestyle therapy to achieve glycemic control and reduce the risk for complications such as heart disease, stroke, vision loss, renal failure, and neuropathy. Diabetes self-management education (DSME) provides individuals with important information and problem-solving skills needed to self-manage their disease process and has been shown to improve glycemic control, nutritional behaviors, and self-blood glucose monitoring accuracy. 3 Those who have completed DSME are also more likely to follow recommended guidelines for diabetes care and display better adherence to medication regimens. 4 The American Diabetes Association recognizes DSME as a vital component of the care of patients with diabetes and recommends that DSME be provided for every patient at the time of diagnosis of diabetes and as needed thereafter. 1 Despite these recommendations and the proven effectiveness of DSME, many patients with diabetes never receive DSME. Only 23–66% of U.S. individuals referred to DSME receive recommended diabetes education services. 5 Factors preventing access to diabetes education are multifaceted and include travel to attend DSME, limited insurance reimbursement for DSME, difficulty attending classes due to work schedule or child care issues, or disabilities that make travel to DSME services challenging. 5,6
The increasing prevalence of diabetes is resulting in limited availability and access to diabetes care services, including access to certified diabetes educators. It is estimated that there is about one certified diabetes educator per 1,400 patients with diabetes in the United States. 7 Because of the many factors limiting access to diabetes education, innovative delivery methods for DSME will need to be developed. One potential avenue that has been studied over the last decade for addressing the reach and accessibility of DSME is the use of Internet-based interventions.
Internet-based DSME
Internet-based delivery of DSME is a potential way to overcome the barriers of distance, limited access, scheduling logistics, and the limited supply of certified diabetes educators. In the United States, there are over 245 million Internet users. 8 Internet use has increased among even middle-aged and older age groups. According to the U.S. Census Bureau in 2010, 80% of the 45–54-year-old age group had accessed the Internet, and 76% of the 55–64-year-old group had accessed the Internet in the past week.
The Internet has been used for many years to disseminate health information and provide health education. 9 Generally, this is done via sharing of information, automated question and answer sites, and downloadable brochures or written guidelines and instructions. The Internet allows for access to updated, appropriate diabetes information regarding disease processes, treatment, and complication prevention. However, assessing whether patient learning and behavior change have occurred can be difficult 10 and is challenging to measure. Patients must be engaged in order to improve knowledge and reinforce preventative strategies. 11
Haythornthwaite 12 described three essential communication components to address in Internet learning environments: content-related exchanges, planning of tasks related to the learning, and engaging in social support. Understanding and sharing content are essential to learning. Planning is imperative as a means of organizing and ensuring clarity of purpose. Social support creates relationships and enhances collaborative learning. Inclusion of these three components builds and sustains online communities.
Internet-based learning offers added flexibility and freedom from physically attending a session at a clinic or office. Learners are able to choose the time and location of their Internet learning and have access 24 h/day. Internet offerings can be provided asynchronously or synchronously, with benefits and drawbacks to both methods. An asynchronous environment is one that is not interactive in real time. Rather, an asynchronous environment or electronic or e-learning site supports working relationships among learners and with teachers, even when participants cannot be online at the same time. The benefits of asynchronous e-learning are numerous: the site is available 24 h/day, and it encourages autonomy and independence and allows for personal flexibility. In addition, asynchronous sites can be programmed to provide interactive programmed responses to participants' inquiries. In an asynchronous learning community, learners may organize their experiences around work, family, sleep, and other obligations. Asynchronous learning assures that consistent messages and information are provided and that all learners receive the same content. The flexibility that online learners experience in asynchronous settings allows for time to reflect and learn at an individualized pace, which is often demonstrated in e-mails and blogs. 13
Synchronous learning occurs in real time and can take place via online videoconferencing and Internet chat rooms. Learners feel less isolated as they can receive immediate feedback, and there is the feeling of shared experience and increased attention to the interaction. 13 In addition, synchronous learning often saves time and money in that content does not need to be designed or recorded for posting online.
Given the increased use of the Internet for health information and education, in general, and the need to reach increasing numbers of patients with diabetes for DSME, we conducted this review to synthesize the current literature regarding Internet-based DSME, examining the efficacy of Internet-based delivery modes, the synchronous and asynchronous features, and the overall advantages and disadvantages of Internet-based DSME.
Materials and Methods
We conducted a review of the allied health, nursing, and medical literature using the Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, Medline, EBSCO, the Cochrane Library, and the Web of Science. The search terms were as follows: “type 2 diabetes AND internet/web based AND education” and “type 2 diabetes AND diabetes self-management education (DSME) AND web-based/internet OR technology assisted education.” Publication dates were restricted from 2004 to 2013. This reflected a time frame during which the Internet was increasingly used to deliver DSME. Reference lists within articles were reviewed using snowballing in order to find other relevant DSME literature.
Study selection
Inclusion criteria were publications in English, type 2 diabetes education interventions (including those focused on health maintenance and prevention of complications), adult participants (age 18 years or older), and specifically programs offered via the Internet. Randomized trials, exploratory studies, and comparative effectiveness designs were included. Exclusion criteria were healthcare provider education programs, face-to-face or non–Internet-based diabetes education interventions, studies focused on multiple diseases or other types of diabetes, pediatric samples (age <18 years), and studies focused on primary outcomes related to emotional well-being and healthcare costs.
In total, 111 articles resulted from the searches outlined above. Of the 111 articles, 14 met the criteria and were reviewed. Figure 1 gives a summary flowchart of literature search and selection. No additional articles were retrieved through reference list searches.
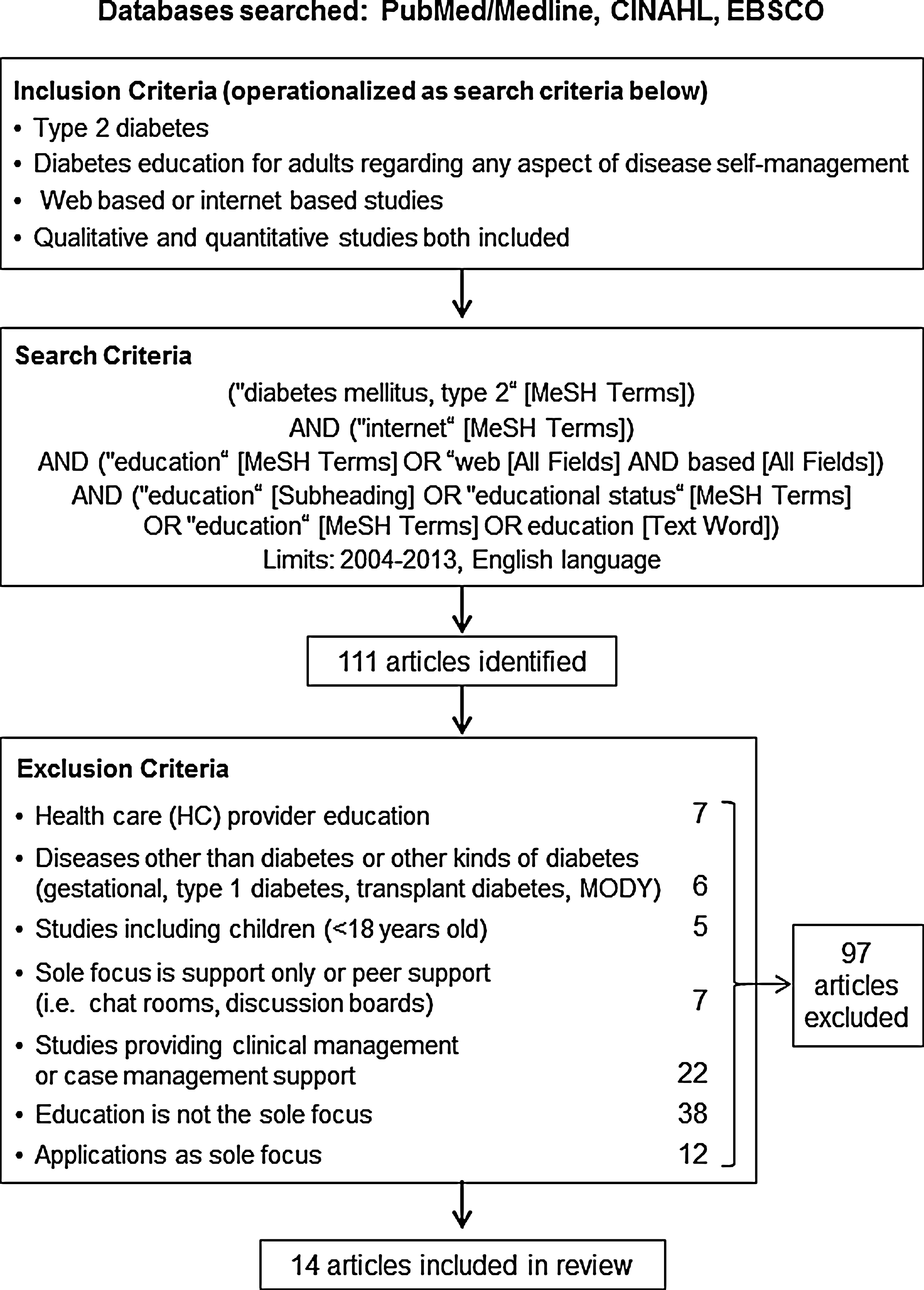
Flowchart of literature search and study selection. MeSH, medical subject heading; MODY, maturity-onset diabetes of the young.
Data extraction
The following data from each article were examined: study design, sample size and characteristics, length of intervention and follow-up, intervention description, outcome variables, results, and pertinent discussion of limitations and findings. Two authors independently reviewed the search results according to the inclusion/exclusion criteria. They then discussed any differences in their recommendations to come to a conclusion as to the appropriateness of the studies based on the criteria.
Matrices of the data are summarized in Table 1. 10,14 –26
AI/AN, American Indian/Alaskan Native; BMI, body mass index; BP, blood pressure; CASM, computer-assisted self-management; CASM+, computer-assisted self-management plus additional social support; DM, diabetes mellitus; DSME, diabetes self-management education; EUC, enhanced usual care; HbA1c, hemoglobin A1c; HL, hyperlipidemia; HTN, hypertension; NA, not available; PM, printed materials; QoL, quality of life; RCT, randomized controlled trial; SE, self-efficacy; T2DM, type 2 diabetes mellitus.
Results
Among the studies reviewed, eight studies were randomized control trials, 10,14,17 –20,22,25 whereas one was a randomized comparative effectiveness trial. 15 There was one pre/post evaluation study, 22 two pilot/feasibility studies, 23,24 and two studies that explored participant usage patterns for Internet-based materials. 25,26 In total, 2,802 subjects were enrolled among the studies reviewed.
Nine of the 14 studies included physiologic outcome variables to assess efficacy of the DSME intervention, measuring hemoglobin A1c (HbA1c), 14,15,17 –20,22,27 blood pressure, and body mass index. 10,15 Related psychosocial and behavioral variables were assessed in some studies: diabetes self-efficacy was measured in four trials, 15,18,19,21 diabetes knowledge was assessed in four studies, 16,22,24,25 and self-reported eating and exercise behaviors were assessed in three trials. 15,17,18 Web site usage patterns were assessed in several trials, some to explore participant interest or ease of accessing materials, 10,15,19,23,25 whereas other trials assessed correlations between Web site usage and study outcomes. 10,16,20,21,24 Two studies compared very short-term outcomes (after only 2 weeks), 16,25 whereas four studies compared outcomes at baseline and again 4, 6, or 12 weeks later. 17,21,22,23 Several studies compared outcomes 6–18 months from baseline, 10,14,15,18 –20 whereas the longest follow-up period was 2 years. 26
Only two studies 14,22 compared Internet education with face-to-face diabetes education typically delivered in clinic settings. Noh et al. 20 compared the same materials between two groups receiving them in different formats: the control group received written materials, whereas the intervention group received cell phone and Web-based information. Glasgow et al. 10 compared engagement of participants between a control group that had Web site access alone, whereas the intervention group also received phone calls and group meetings. McIlhenny et al. 19 compared individualized face-to-face orientation with an educational Web site versus written instructions on how to access the Web site alone. The remaining randomized trials compared Internet-based diabetes education with usual clinic care 15,17,18,25 ; therefore the control group did not receive an educational intervention.
Some interventions provided a component of social support through message boards, discussion groups, or peer support, and these were viewed positively by participants. 15,22,23 Other interventions included interaction through individualized e-mail and phone contact. 10,18,19,22,26 These studies showed a high participant satisfaction rate with the level of contact. Social support was seen as being very important when face-to-face interactions took place. 23
Synchronous versus asynchronous features
All of the studies provided components of asynchronous interaction for participants, through interactive Web sites, short message services, e-mail communication, or text messaging. Participants could pace themselves through materials and access materials whenever convenient for them. The ability for participants to interact or message with an educator/healthcare provider in some trials was seen as a very worthwhile feature by participants. 14,19,20,22,23,26 None of the studies included synchronous online interactions as part of the intervention, although two studies 14,22 incorporated live, face-to-face group meetings as control groups.
Effectiveness of interventions
Internet education generally resulted in significantly improved glycemic control compared with usual care. 14,17 –20,22 Web-based education was not comparatively better at improving glycemic control outcomes than printed education materials when both were compared with usual care in one study. 17 The authors noted that both the Web-based and printed education groups received more attention that the usual care groups; thus the increased attention may have been one explanation for these results. A Web-based automated cell phone/e-mail system resulted in greater improvement in HbA1c compared with usual written DSME materials (−1.53% vs. −0.49% in control; P=0.031). 20
Glasgow et al. 10 examined an enhanced usual care model versus computer-assisted self-management (CASM) program versus CASM program plus additional support (which included face-to-face interaction). No differences in outcomes such as HbA1c, body mass index, or lipid levels were reported between groups. Attrition rates were higher in the CASM plus support group compared with the usual care and CASM groups.
Yet, in a study comparing two levels of Web-based interventions—an online DSME program versus online DSME program with additional e-mail reminder messages along with comparison with usual care—both of the online DSME groups had a significant improvement in HbA1c compared with usual care with no differences in outcomes between the two different Web-based interventions. 18 Lorig et al. 18 found that patients with higher HbA1c at study beginning seemed to benefit most from these interventions, whereas those with good glycemic control at baseline had less impressive (although significant) glycemic improvements. 23
In one relatively large study (n=98) comparing Internet-based educational materials plus face-to-face diabetes nurse educator contact with access to the Web site alone, the added interaction with an educator resulted in improved glycemic control and diabetes knowledge, 19 whereas another smaller trial (n=31) noted improved diabetes care behavior in both a face-to-face and Internet-based group, but HbA1c only improved in the Internet-based education group. 22
Web-based DSME also resulted in improved clinic attendance (P≤0.0001) 14 compared with face-to-face DSME. Some studies also demonstrated improvements in self-efficacy, 18 diabetes knowledge, 16,19,22,24 exercise behaviors, 15,17 and self-care behaviors 15,21 after receiving Web-based DSME.
In a majority of studies that analyzed participant engagement with the Internet interventions, greater participant usage of Web-based materials resulted in improved knowledge and/or glycemic control. 10,20,24 However, Heinrich et al. 25 did not find a relationship between amount of time spent using their Web educational program and improved knowledge. Participant interest and time spent logged into programs waned as the studies progressed, although the significance of this is unclear. The lack of prompts for participants to log-in, lack of regularly updated materials available on the site, and technical difficulties were all cited as reasons for declining participation. 19 –21,26
In terms of addressing culturally diverse needs, Porter et al. 24 provided a Web site tailored to Hispanic individuals that provided all information in Spanish, and this small pilot study (n=9) demonstrated an increase in self-reported nutrition and diabetes-related skills. Lorig et al. 18 provided an intervention with materials, discussion boards, and peer facilitators in both Spanish and English and culturally appropriate materials for those of American Indian/Alaskan Native descent. They were successful in significantly improving HbA1c (short-term), patient activation, and self-efficacy (long-term) compared with usual care.
Limitations of studies
Our review did not include unpublished manuscripts, which could introduce publication bias into our conclusions. Study follow-up time periods were relatively short, with a few studies lasting 2–12 weeks and a majority following participants for 6 months. Three studies followed patients for longer intervals, 10,15,18,26 with one 24-month-long study. 26 Attrition rates varied, from 18% to 62%, 10,19,22 although attrition did not seem to be related to study length or whether the patient had been randomized into an intervention versus control group. Study outcomes are also limited by the fact that there were no data captured regarding what additional educational materials may have been accessed by the patient during the study interval, either printed or Web based.
Participant training and support to assure appropriate usage of the Internet materials were provided for involved providers and participants. 14 Participants had difficulties with more sophisticated programs such as smartphone applications 20 in one study that resulted in some subject dropout. Nearly all studies enrolled middle-aged adults, with average ages of 40–63 years, 10,14,18 –22,26,28 but none specifically examined how older adults may use or benefit from Web-based education. Likewise, only one trial enrolled a significant proportion of young adult participants, 15 who may be more Web-savvy and thus navigate these types of programs with greater ease. One study provided computers and/or Internet access 19 for participants, which eliminates access barriers and examines only how the participant responds to the intervention. However, generalizability of results may be limited in certain socioeconomic and rural settings, and this may reduce the feasibility of the intervention across socioeconomic groups. Likewise, participant self-selection for studies (i.e., those with well-controlled diabetes) brings up the question as to whether those who may benefit the most are likely to receive the Web-based education.
Intervention groups commonly involved more access to and interaction with healthcare providers and facilitated patients' goal setting and monitoring of these goals. Thus it seems that any increased interaction between the patient and provider may prove beneficial, regardless of the form of interaction. The “usual care” groups received little in the way of education, feedback, or modification of plan of care between clinic visits. Thus it is difficult to ascertain if indeed the education and increased attention received via the Internet resulted in improved outcomes (the “Hawthorne effect”), or whether the same education and attention given in the traditional clinical setting would also result in improved outcomes.
Conclusions
From this review we can conclude that education above and beyond usual care for patients improves knowledge and glycemic control. However, the benefits of providing education in an online format seem to be the ability to reach more patients at any time and at convenient times for both the patient and the provider. In addition, online programs can provide education and information more efficiently (e.g., patients can access materials whenever they want and from home) and economically than if done on a one-on-one or face-to-face basis, although there is little research information on the extent of cost savings possible using Internet-based DSME.
All Internet-based interventions were more effective when compared with usual care (which many times did not include standard educational content) or printed written interventions alone. Printed materials can vary in “interest factor” to attract readers when compared with more interactive materials delivered via the Web. Patients adapted relatively easily to the Web-based delivery platform, and attrition rates related to technical issues seemed to be low. The asynchronous format seems to lend itself well to diabetes-related information. Learners can process complicated concepts such as medication use and nutrition information at their own pace. Asynchronous communication also works well for information exchange such as glucose logs and medication adjustment instructions, and this feature is seen as beneficial for patients.
Waning interest in accessing online DSME materials over time may mean that the patient has learned all he or she needs to know; thus returning to the site may not be seen as helpful. Diabetes is a progressive disease, and self-management needs also tend to increase in complexity as the time with disease goes on; this factor may decrease relevance and interest in online educational materials that are more self-directed. Simultaneously this could prompt a need for more individualized education (where there is the ability to discretely clarify and individualize the education needs of the patient), and this may not be suited for online delivery. Determining the amount and type of education appropriate for patient needs may be a subject for further research, or whether providing rotating, dynamic content may maintain patient interest in learning about new topics. A necessary level of engagement in online interventions to improve outcomes remains unclear and may be dependent on multiple personal factors or characteristics. Combining interaction with healthcare providers/educators and peer support with elements of education could be a way to maintain patient interest and engagement in DSME activities and provide ongoing social support. When participants can actually feel a part of the experience, they can build supportive relationships with educators and social relationships with fellow participants. If this synchronous communication or networking does not occur in the online format, the benefits of the face-to-face teaching environment for support will continue to outweigh that of Web-based delivery.
Future Directions for Research
Developing an online method to provide DMSE would be enhanced with the use of both asynchronous and synchronous aspects. Learners can benefit from group learning and social support, while increasing their knowledge and understanding by reflecting and processing knowledge at their own pace. Patients can learn from one another in diabetes self-management groups designed for social support, and this has proven to be effective in maintaining and improving glycemic control. 29 Learners are also able to participate in the educational offerings both at their own pace and as part of a group.
Longitudinal research is important in order to determine relationships between Internet intervention use and health outcomes. 30 In addition, retention of knowledge over time will be imperative to examine, as well as linking knowledge attainment to sustainable symptom management and disease control. More studies comparing various methods of delivery would be helpful, especially as related to the complexity and cost of delivery methods to determine efficacy, cost-effectiveness, and sustainability.
It is important to note that the ability of the participant to interact with a healthcare provider via the Internet was seen as valuable by participants. Studies exploring programs that include education along with other features such as interdisciplinary care coordination and active medication management in-between face-to-face visits (which were excluded in this review) may be more successful in helping patients negotiate their self-care needs, along with maintaining patient engagement. Because diabetes is a chronic illness and social support is key in successful management 31 in addition to education, future research could be directed at determining if relationships and support could be strengthened through Web-based DSME.
Other delivery platforms that allow for synchronous communication such as video teleconferencing, Web conferencing, or virtual environments might allow for increased sense of community- and relationship-building. The preliminary data suggest that virtual environments provide a feasible and useful platform of diabetes education and support for patients and educators. Easy access to both synchronous and asynchronous diabetes education, skill-building activities, and support from a home computer help to remove barriers to attending clinic-based meetings. 32
Footnotes
Author Disclosure Statement
No competing financial interests exist.