
Abstract
Background:
Excessive force required to deliver a set dose of insulin as well as a localization of the push button and its upwards extension may result in significant difficulties to safely perform insulin injection, including bending/breakage of the injector's needle. The GensuPen2 (Copernicus/Bioton, Warsaw, Poland) pen has a unique spring-assisted delivery system and a lateral trigger device for injection of insulin to improve its ergonomics. We tested the force required to administer insulin using three pens: GensuPen2, NovoPen® 4 (Novo Nordisk, Bagsværd, Denmark), and HumaPen Ergo® (Eli Lilly, Indianapolis, IN).
Materials and Methods:
Using a certified dynamometer we tested injection force at three doses of insulin: 2, 30, and 60 U, using each of the three injectors (n=10) in triplicate. Area under the curve (AUC) and maximum force used were calculated for each series of injections.
Results:
When administering doses of 2, 30, and 60 units of insulin, the GensuPen2 (6.55±1.09, 6.52±1.92, and 6.89±1.15 N, respectively) required significantly lower maximum force than the NovoPen 4 (9.04±0.61, 12.96±1.45, and 15.42±0.99 N, respectively) and the HumaPen Ergo (17.66±1.88, 32.14±6.08, and 40.39±7.64 N, respectively) (all P<0.0001). The AUC of force used for insulin injection with GensuPen2 did not differ between doses (P=0.82). At all dose levels, GensuPen2 required significantly lower force than the other two injectors. Moreover, the mode of holding of GensuPen2 was more similar to the natural arrangement of the hand while gripping a cylindrical item in comparison with NovoPen 4 and HumaPen Ergo.
Conclusions:
Usage of the GensuPen2 injector with a lateral trigger location and spring-assisted delivery system reduces the force required for drug administration, especially at high doses of insulin.
Background
D
Approximately 0.5 million people with diabetes in Poland use insulin in their therapeutic regimen. Owing to the efforts of the National Health Fund, insulin pumps are refunded by the state for children and pregnant women who develop diabetes and require insulin, but no such support is granted to adults with type 2 diabetes requiring insulin injections on a daily basis. Insulin pens reduce fear of self-injection in contrast to needles and vials 2 and have been the dominant mode of insulin self-delivery in Poland for the last 20 years among adult patients with diabetes.
It is also known that diabetes can lead to reduced finger joint mobility and lower hand strength, impaired muscle function, and carpal tunnel syndrome. 3 –5 These ailments may hinder the patient's ability to operate small or complex devices, potentially limiting their ability to administer insulin. Use of easily operated insulin pen devices requiring less injection force would thus appear to be beneficial in such patients. On the other hand, excessive force exerted by the patient to deliver a set dose of insulin may result in increased pain during injection or possibly in bending/breakage of the pen injector's needle. 6
Most insulin pens available on the market follow the same general design, with the trigger for releasing insulin mounted on its distal end. This makes the patient press the button with the thumb of his or her dominant hand, while maintaining a firm grip on the pen, while the other hand forms the skinfold for injection. When administering large doses of insulin, however, the distance of the pen's trigger may shift farther away, necessitating the patient to extend his or her thumb and apply pressure to the trigger for a longer period of time, thus using more force. One solution to this problem would be to relocate the trigger closer to the pen's tip to reduce the strain placed on the thumb and improving stability of the device during injection (Supplementary Fig. S1; Supplementary Data are available online at
The GensuPen 2 device (Copernicus/Bioton, Warsaw, Poland) is an insulin pen with a spring-assisted insulin release mechanism and a laterally located trigger, constructed to facilitate insulin delivery. We analyzed the performance of this device and compared it with other insulin injectors in terms of force necessary to administer the intended dose of insulin.
Materials and Methods
The study was performed in laboratory settings without involvement of human subjects. The force required to administer insulin using three pen injectors—GensuPen 2, NovoPen® 4 (Novo Nordisk, Bagsværd, Denmark), and HumaPen Ergo® (Eli Lilly, Indianapolis, IN)—was measured and compared in three scenarios: administration of 2, 30, and 60 units of insulin.
Injection time was established by measuring the test injection times of GensuPen 2 for the three compared doses. The button speed was kept constant as in other studies that compared pen force requirements. 7,8 Because of the unique construction of the device it was impossible to assure identical flow rates, in contrast to the study by Friedrichs et al. 9 Injection time was thus preestablished to last between 1 and 1.5 s for 2 insulin units, 3.5 to 4 s for 30 units, and 5.5 to 6.5 s for 60 units, to mirror standard conditions of insulin injection. The end of insulin administration was determined by visual control of insulin outflow from the needle as in other similar studies on the subject. 10
Each injection cycle of 2, 30, and 60 units with each insulin pen was done manually by T.T. (who is right-handed), using a new needle and a new insulin cartridge filled with human insulin (Gensulin N [Bioton] for GensuPen 2; Humulin® N [Eli Lilly] for HumaPen Ergo; and Actrapid® [Novo Nordisk] for NovoPen 4). Ten devices of each type were used in the study. Injections of the same insulin doses were done three times with each of the pens selected in random order, producing a total of 30 measurements for each tested pen type.
Ergonomic analysis was performed by T.T. and D.R.-L. in a certified laboratory, dedicated to ergonomy analyses for medical product manufacturers. All force measurements were done under standard atmospheric conditions at room temperature using a certified tensile meter (DMP1 JBA; Zbigniew Staniak, Gdansk, Poland) approved for research use. The device's sensor was set up vertically to reduce the impact of the pen's weight on the strength required to administer insulin. The tensile meter collected data of the force used every 0.01 s. Afterward, areas under the curves (AUCs) were calculated, to account for variability of injection time, using the trapezoid approximation with the “sumproduct” formula in Microsoft (Redmond, WA) Excel®. AUCs and peak force used during each injection were compared between the groups. Distance between the trigger surface and the skin during injection was measured using a ruler.
Statistical analysis
Measurements were performed using analysis of variance at all three dose levels. Post-hoc comparisons were done with Tukey's test, if analysis of variance yielded significant results. P levels <0.05 were selected as the threshold for declaring significance. All statistical analyses were performed in Statistica version 10.0Pl software (Statsoft, Tulsa, OK).
Results
Lateral location of the trigger resulted in the shortening of the thumb–skin distance to 93 mm regardless of the preset insulin dose, in comparison with values of 139, 147, and 157 mm noted with the NovoPen 4 for doses of 2, 30, and 60 units, respectively, or 143, 158, and 173 mm, respectively, observed with the HumaPen Ergo. This would translate to lower torque with the use of GensuPen 2, potentially contributing to greater stability of the pen during the injection. All measurements of the cylindrical hold diameter of the GensuPen 2 were between the 5th and 95th percentile achievable by the Polish population (34–44 mm for women and 35–46 mm for men).
After completion of measurement and data analysis, we found that the GensuPen 2 device required significantly lower force expenditure to deliver insulin than the HumaPen Ergo when delivering 2 units of insulin. The force necessary to deliver this dose was 53% lower than when using the HumaPen Ergo (Table 1). At 2 units the difference in force used for injection between the GensuPen 2 and NovoPen 4 was 17.5% but did not reach statistical significance (P=0.1794). The maximum forces applied during the injection of 2 units were, however, significantly different among all three pens, with the HumaPen Ergo showing threefold and twofold higher maximum force registered than the GensuPen 2 and NovoPen 4, respectively.
Data are reported as mean±SD values.
P<0.001 versus HumaPen Ergo.
P<0.001 versus HumaPen Ergo and P<0.05 versus NovoPen 4.
P<0.001 versus HumaPen Ergo and NovoPen 4.
AUC, area under the curve.
When injecting 30 units, the differences were even more pronounced, as the spring-assisted trigger mechanism of GensuPen 2 reduced the force needing to be maintained during the later phases of insulin injection. AUCs of force expended throughout the injection with the GensuPen 2 was 84% lower than that applied with the HumaPen Ergo and 58% lower than that used with the NovoPen 4 (Table 1). Differences in maximum force used were similar in terms of direction and magnitude.
When the administered dose was set at 60 units, the GensuPen required 87% less force than the HumaPen Ergo and 66% less force than the NovoPen 4. Similarly, maximum force of injection with the GensuPen 2 was reduced by 83% with regard to the HumaPen Ergo and by 55% with regard to the NovoPen 4. All these dose- and pen-dependent differences are visualized in Figure 1.
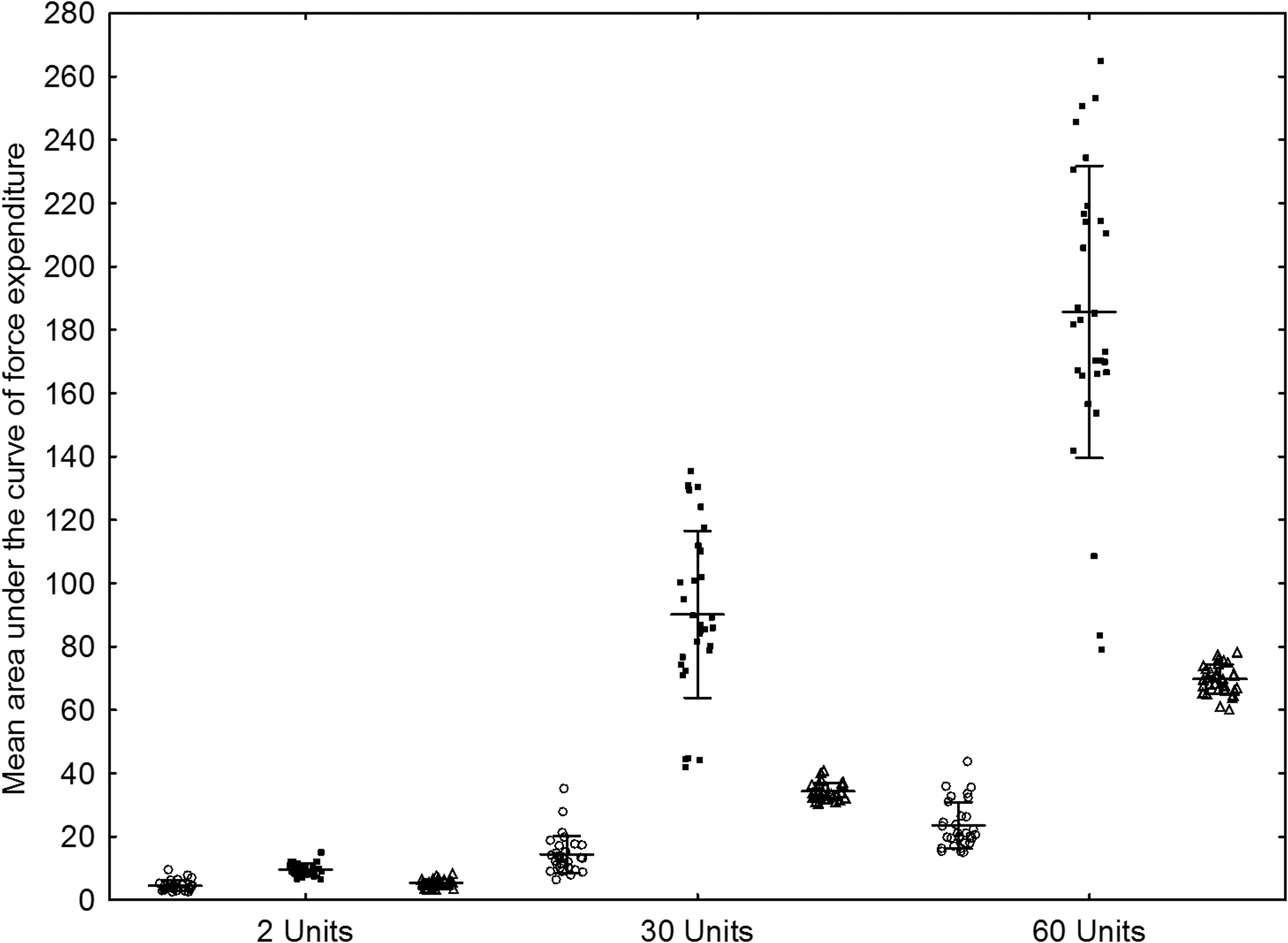
Mean areas under the curve of force required to administer the intended dose of insulin using the GensuPen 2 (circles), NovoPen 4 (triangles), and HumaPen Ergo (squares) devices. Whiskers denote 95% confidence intervals.
The differences of AUC between the insulin doses injected with the tested pens were significant (P<0.0001 in all three cases). However, the maximum force used during injection did not differ significantly among the 2-, 30-, and 60-unit doses in the GensuPen 2 (P=0.8170). After analyzing individual time–force curves it became clear that this mode of insulin release makes the applied force considerably lower than in a situation in which the patient has to actively push downward, overcoming the piston mechanism's friction and effectively shortening the pen. This produced a plateau of force upkeep at approximately 5 N for the duration of injection, regardless of the magnitude of the injected dose (Fig. 2). All these reductions were direct consequences of the spring-assisted trigger mechanism, which required only the initial push and maintenance of constant force thereafter with the GensuPen 2.

Applied force diagrams for
Discussion
The use of the GensuPen 2 pen injector allowed for a significant reduction in the force necessary to properly administer the intended dose of insulin.
At very small doses, the duration of injection using the GensuPen 2 may require marginally more time in order to allow for the trigger mechanism activation. For larger doses of insulin, this time difference is imperceptible.
The reduction of force applied by the patient, however, is considerable, with the difference between the GensuPen 2 and conventional pens increasing along with the administered dose. The common way of achieving reduced injection force was to shorten the push-button travel distance, which was done by limiting the stroke dial extension. 11 In the case of the SoloSTAR® (Sanofi, Paris, France) pen, this shortening of the push-button travel distance made pens perceivably easier to use by patients, 11 –13 even though the difference in button extension was only 22%. 14 It is clear that this was an attempt at solving the problem of thumb distension and the resultant increase of injection force. However, shortening the piston itself is only a partial solution. The modified construction of the GensuPen 2 resolves the issue by moving the trigger to the side, thus shortening the distance between the thumb-operated trigger and the skin. Moreover, the spring-assisted mechanism made the injector easier to operate for people with restricted joint movement or impaired fine motor skills. However, because surveys show that the most important feature for patient satisfaction is an easy push-button injection, 15 one can assume that the design of GensuPen 2 should meet with acceptance of the general population of diabetes patients as well.
The spring-assisted delivery system and a lateral trigger device for injection of insulin were introduced primarily to improve the ergonomics of the insulin administration. Another theoretical advantage of such layout is the reduced torque and resulting improved stability during injection. Although as far as we know no large studies have been performed to examine the frequency of needle damage or bending in insulin pens, the problem may be of clinical consequence. 16 Because the only factor that has been identified to contribute to needle bending is their size, it is logical to assume that the thinner the needle, the more susceptible it is to bending under pressure. If one considers that the hand's position during administration with the GensuPen is closer to the skin, it is very likely that this insulin pen allows for better stabilization during injection and potentially limits the extent of tissue and needle damage due to unintentional needle mobility. This field would, however, require further in vivo experiments.
The study does have some limitations due to its experimental nature. Injection time was calibrated for the NovoPen 4 and HumaPen Ergo to match that of the tested GensuPen 2. Because the injection cannot be accelerated using the GensuPen 2, we deemed this methodology to be the best comparative model. One could, however, inject insulin faster using the two other devices by applying greater force. To account for that possibility, our comparisons focused on the AUCs for the tested pens, regardless of the actual injection time. Should the patient deliberately press the button with more force, the maximum force would increase, and insulin would be administered faster but with a similar AUC. Second, the injections were made into the air. Should the injections be made into actual tissue, the force required could be greater, because of back pressure. It is unlikely, however, that there would be any specific difference in back-pressure characteristics among any of the three compared devices. Moreover, because the injection is driven by the spring mechanism, any additional back pressure would be transferred to the mechanism rather than to the patient's thumb. Finally, it is obvious that the reduction of injection force should translate to clinical applicability. Epidemiological studies on grip strength performed by Forrest et al. 17,18 showed that even after accounting for osteoporosis or older age, the patients are able to exert a force far exceeding that necessary for insulin administration. Therefore, we cannot assume that the general population may be unable to use standard insulin pens or be enabled to use the GensuPen 2 in contrast to the other devices. However, the reduced force, ease of holding, and the easy-to-operate trigger are appealing characteristics that may facilitate the daily routine of administering insulin.
Conclusions
Usage of the GensuPen2 pen injector with a lateral trigger location and the spring-assisted delivery system vastly reduces the force required for insulin injection, especially when administering high doses of insulin.
Footnotes
Acknowledgments
Costs of the insulin pens, measurements, and data analysis were covered by an unrestricted grant funded by Bioton Inc., Ozarow Mazowiecki, Poland.
Author Disclosure Statement
R.R. is an employee of Bioton Inc. and a Vice President at Copernicus Inc. W.F., D.R.-L., T.T., and W.M. declare no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.