
Abstract
We recently developed new electrochemiluminescence (ECL) insulin autoantibody (IAA) and glutamic acid decarboxylase 65 autoantibody (GADA) assays that discriminate high-affinity, high-risk diabetes-specific autoantibodies from low-affinity, low-risk islet autoantibodies (iAbs) detected by radioassay (RAD). Here, we report a further validation of the ECL-IAA and -GADA assays in 3,484 TrialNet study participants. The ECL assay and RAD were congruent in those with prediabetes and in subjects with multiple autoantibodies, but only 24% (P<0.0001) of single RAD-IAA-positive and 46% (P<0.0001) of single RAD-GADA-positive were confirmed by the ECL-IAA and -GADA assays, respectively. During a follow-up (mean, 2.4 years), 51% of RAD-IAA-positive and 63% of RAD-GADA-positive subjects not confirmed by ECL became iAb negative, compared with only 17% of RAD-IAA-positive (P<0.0001) and 15% of RAD-GADA-positive (P<0.0001) subjects confirmed by ECL assays. Among subjects with multiple iAbs, diabetes-free survival was significantly shorter if IAA or GADA was positive by ECL and negative by RAD than if IAA or GADA was negative by ECL and positive by RAD (P<0.019 and P<0.0001, respectively). Both positive and negative predictive values in terms of progression to type 1 diabetes mellitus were superior for ECL-IAA and ECL-GADA, compared with RADs. The prevalence of the high-risk human leukocyte antigen-DR3/4, DQB1*0302 genotype was significantly higher in subjects with RAD-IAA or RAD-GADA confirmed by ECL. In conclusion, both ECL-IAA and -GADA are more disease-specific and better able to predict the risk of progression to type 1 diabetes mellitus than the current standard RADs.
Introduction
I
At the initial screening, insulin autoantibodies (IAAs) or glutamic acid decarboxylase (GAD) 65 autoantibodies (GADAs) are often detected in isolation and at a low level. 2 –5 None of the 407 DPT-1 participants expressing only IAA progressed to diabetes during the initial observation period, 6 casting doubt whether these IAA signals were diabetes-related. Exclusion of these “low-risk autoantibodies” by using a more specific assay would greatly enhance the efficiency of risk staging for clinical trials.
Previous efforts to improve specificity of iAbs have included determination of their affinity, 2 –5 immunoglobulin G subtyping, 7 –9 and a truncated GAD65 molecule. 10 These methods have improved assay specificity, but most are too costly and cumbersome for a large-scale screening or associated with some loss of sensitivity. Recently, we developed new electrochemiluminescence (ECL) IAA 11,12 and GADA 13 assays that discriminated high-affinity, diabetes-specific iAbs from low-affinity, “low-risk” iAbs detected by radioassay (RAD).
In the present study, we measured ECL-IAA and -GADA in a large cohort of relatives being followed in the TrialNet Pathway to Prevention Study of Type 1 Diabetes (PPS). The ECL assays were performed in a blinded manner; all demographic information of the samples studied was received after the results were submitted to the TrialNet Coordinator Center. The ECL assay sensitivity, specificity, and predictive value were compared with those for the RAD-IAA and RAD-GADA.
Research Design and Methods
Subjects
The study included 3,484 subjects enrolled in the TrialNet PPS between 2005 and 2012 with 384 pre-T1DM who were followed to clinical T1DM later and 3,100 without T1DM. The TrialNet PPS is an ongoing national cohort study that aims to assess the natural history of progression to T1D and to identify high-risk subjects eligible for T1DM prevention trials. The participants are first-degree relatives (1–45 years of age) or second/third-degree relatives (1–20 years of age) without diabetes of patients with T1DM. All subjects are screened for IAA, GADA, and IA-2A. Subjects who are positive for any of the iAbs are tested for islet cell autoantibodies (ICAs), ZnT8 autoantibodies (ZnT8A), and human leukocyte antigen (HLA)-DQ genotypes. Subjects with two or more confirmed iAbs are followed every 6 months with hemoglobin A1c and oral glucose tolerance tests. All subjects selected for this study were tested for IAA, GADA, IA-2A, and ZnT8A by TrialNet RADs; 2,682 of those were positive for at least one iAb, including those 384 pre-T1DM and 2,298 without diabetes. Follow-up iAb data (range, 0.1–8.1 years; mean, 2.4 years; median, 1.5 years) were available for 2,170 of the study participants.
ECL-IAA assay
The ECL-IAA assay method has been previously published. 11 In brief, serum samples were treated with 0.5 M acetic acid, followed by neutralization with Tris buffer (pH 9.0), and then mixed with both sulfo-tag and biotin-labeled proinsulin for overnight incubation at 4°C. The antigen–antibody complexes with biotin were captured by a streptavidin-coated plate and counted on an Imager 2400 (MSD, Gaithersburg, MD). The results were expressed as an index against our internal standard positive control of insulin monoclonal antibody. The assay cutoff index of 0.006 was set at the 99th percentile of 100 healthy controls, and the interassay coefficient of variation was 4.8% (n=20). In the recent IASP Workshop at the 2013 Immunology of Diabetes Society meeting (Lorne, Australia), among patients with newly diagnosed T1DM, the sensitivity for ECL-IAA was 68%, and the specificity was 99%.
ECL-GADA assay
The ECL-GADA assay method has also been previously published. 13 In brief, 20 μL of fivefold diluted serum was mixed with 20 μL of antigen buffer containing both sulfo-tag and biotin-labeled GAD65 and incubated at 4°C for overnight. The antigen–antibody complexes containing biotin were captured by a streptavidin-coated plate and counted on an Imager 2400. The results were expressed as an index against our internal standard positive control of GAD65 monoclonal antibody. The assay cutoff index of 0.023 was set at the 99.5th percentile of 181 healthy controls, and the interassay coefficient of variation was 8.8% (n=10). In the recent IASP Workshop at the 2013 Immunology of Diabetes Society meeting, among patients with newly diagnosed T1DM, the sensitivity for ECL-GADA was 76%, and the specificity was 99%.
Other laboratory measurements
The RADs for IAA, GADA, IA-2, and ZnT8A used in the present study were all performed in our laboratory and have been previously published. 14 HLA-DQ and DR polymorphisms were determined by allele-specific oligonucleotide genotyping. 15 The haplotypes of interest were DQA1*0501-DQB1*0201 (DQ2), DQA1*0301-DQB1*0302 (DQ8), and DQA1*0102-DQB1*0602 (DQ6).
Statistical analysis
Statistical analyses were performed using correlation analysis, rank sum, or Fisher's exact test in PRISM version 4.0 software (GraphPad Software Inc., San Diego, CA). Survival analyses used the log rank test in SAS version 9.3 software (SAS Institute, Cary, NC). Statistical significance was determined by an α level of 0.05.
Results
ECL-IAA and -GADA assays improve assessment of T1DM risk
Among 384 pre-T1DM subjects who were followed to T1DM, the sensitivity of the ECL-IAA assay (54.7%, 210/384) was similar to that for the RAD-IAA assay (48.4%, 186/384). The sensitivity of the ECL-GADA (79.2%, 304/384) and RAD-GADA (76.8%, 295/384) assays was also similar. Figure 1 compares positivity and levels of ECL-IAA and RAD-IAA (Fig. 1A) as well as ECL-GADA and RAD-GADA (Fig. 1B) among 384 prediabetes samples with specificity set at the 99th percentile for each assay. The levels were strongly correlated between ECL-IAA and RAD-IAA (R 2=0.55; P<0.0001) and between ECL-GADA and RAD-GADA (R 2=0.70; P<0.0001). Only nine RAD-IAA-positive and 16 RAD-GADA-positive samples at low levels were found to be negative in ECL assays.
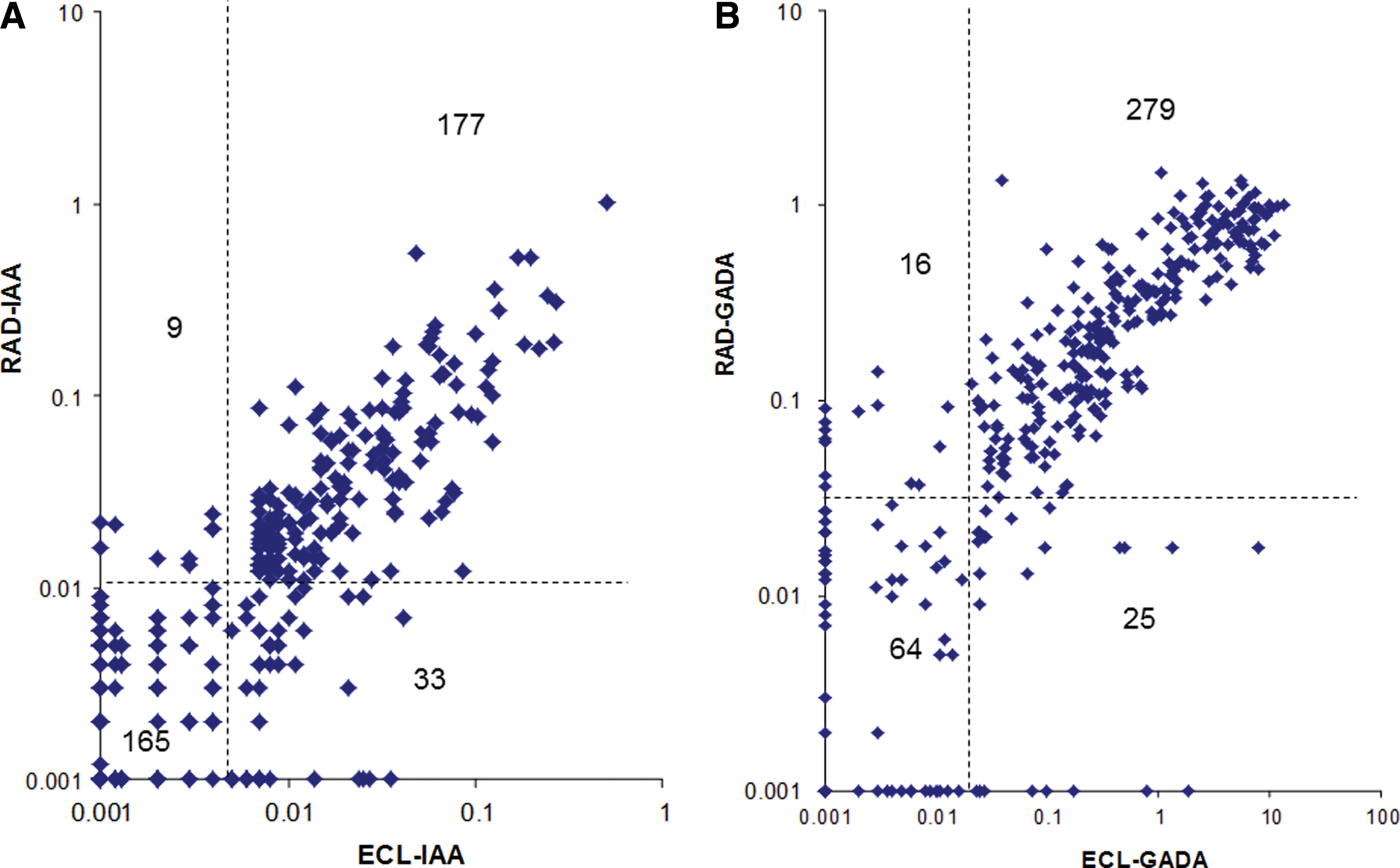
Comparison of islet autoantibody levels between electrochemiluminescence (ECL) and radioassay (RAD) among 384 TrialNet prediabetes subjects who were prospectively followed up to clinical type 1 diabetes mellitus. The dotted lines represent the assay cutoffs. All assays were set at 99% specificity.
Of 3,100 subjects who had not developed T1DM, 2,298 were positive for at least one iAb, and 802 were negative for all iAbs. Among iAb-positive subjects, 75.2% (1,727/2,298) were positive for a single iAb; most were positive for IAA (n=421) or GADA (n=1,169) only. It is remarkable that both ECL-IAA and ECL-GADA assays discriminated high-risk subjects with multiple iAbs or those followed to T1DM from low-risk subjects with a single iAb. The results of the ECL-IAA assay in all subjects participating in the present study are summarized in Figure 2. Only 1.0% (8/802) of subjects negative for all iAb by radioassays were ECL-IAA positive. The iAb-positive subjects who had not progressed to T1D were subdivided into RAD-IAA negative (n=1,581) or RAD-IAA positive (n=717). Among the former, 4.1% (54/1,306) of subjects with a single iAb were ECL-IAA positive versus 19.0% (52/275) of subjects with multiple iAbs (P<0.0001); among the latter, 21.1% (89/421) of subjects with a single iAb (RAD-IAA) were ECL-IAA positive versus 88.5% (262/296) of subjects with multiple iAbs (P<0.0001). ECL-IAA positivity was found in 54.7% (210/384) of subjects who later developed diabetes (pre-T1DM), compared with 48.4% (186/384) for RAD-IAA positivity (P=0.097).

Electrochemiluminescence-insulin autoantibody (IAA) results for all 3,484 TrialNet subjects: all four islet autoantibodies negative (Ab–) (n=802); islet autoantibodies positive with radioassay (RAD)-IAA negative (n=1,581), subdivided into single islet autoantibody (1Ab) positive (n=1,306) and multiple islet autoantibodies (2Ab) positive (n=275); islet autoantibodies positive with RAD-IAA-positive (n=717), subdivided into 1Ab positive (IAA+ only; n=421) and 2Ab positive (n=296); and pre-diabetes mellitus (DM) (n=384). (Color graphics available online at
Similar comparisons for the ECL-GADA assay are summarized in Figure 3. Only 1.2% (10/802) of subjects negative for all iAbs by radioassay were ECL-GADA positive. The iAb-positive subjects who had not progressed to T1DM were subdivided into RAD-GADA negative (n=627) or positive (n=1,671). Among the former, 2.9% (16/558) of subjects with a single iAb were ECL-GADA positive versus 23.2% (16/69) of subjects with multiple iAbs (P<0.0001); among the latter, 44.3% (518/1,169) of subjects with a single iAb (RAD-GADA) were ECL-GADA positive versus 92.6% (465/502) of subjects with multiple iAbs (P<0.0001). ECL-GADA positivity was found in 79.1% (304/384) of those who developed diabetes (pre-T1DM), compared with 76.8% (295/384) for RAD-GADA (P=0.486).

Electrochemiluminescence-glutamic acid decarboxylase 65 autoantibody (GADA) results for all 3,484 TrialNet subjects: all four islet autoantibodies negative (Ab–) (n=802); islet autoantibodies positive with radioassay (RAD)-GADA negative (n=627), subdivided into single islet autoantibody positive (1Ab) (n=558) and multiple islet autoantibodies positive (2Ab) (n=69); islet autoantibodies positive with RAD-GADA positive (n=1,671), subdivided into 1Ab positive (GADA+ only; n=1,169) and 2Ab positive (n=502); and pre-diabetes mellitus (DM) (n=384). (Color graphics available online at
“Single” RAD-IAA or RAD-GADA not confirmed by the ECL assay is often transient and less predictive of T1DM
Most of the subjects with single RAD-IAA or -GADA tested negative for the corresponding ECL-IAA or -GADA. Among 2,170 subjects who had follow-up data available, 1,276 were those with a single iAb, including 338 “single” RAD-IAA and 938 “single” RAD-GADA subjects. The follow-up data are summarized in Figure 4 for the “single” RAD-IAA group (Fig. 4A) and the “single” RAD-GADA group (Fig. 4B). Half (51.1%, 129/252) of the subjects with “single” RAD-IAA, not confirmed by ECL-IAA, lost their IAA positivity during the follow-up (median, 1.5 years), compared with only 17.4% (15/86) (P<0.0001) of those confirmed by ECL-IAA. Moreover, only 2.8% (7/252) of those with RAD-IAA not confirmed by ECL-IAA have progressed to multiple iAbs or T1DM, compared with 34.9% (30/86) (P<0.0001) of the subjects with “single” RAD-IAA confirmed by ECL-IAA. As for GADA (Fig. 4B), 62.9% (316/502) of the subjects with “single” RAD-GADA not confirmed by ECL-GADA lost their GADA positivity during the follow-up, compared with only 14.9% (65/436) (P<0.0001) of those confirmed by ECL-GADA. Similarly to IAA, only 3.6% (18/502) of the subjects with “single” RAD-GADA not confirmed by ECL-GADA have progressed to multiple iAbs or T1DM, compared with 19.7% (86/436) (P<0.0001) of those confirmed by ECL-GADA.
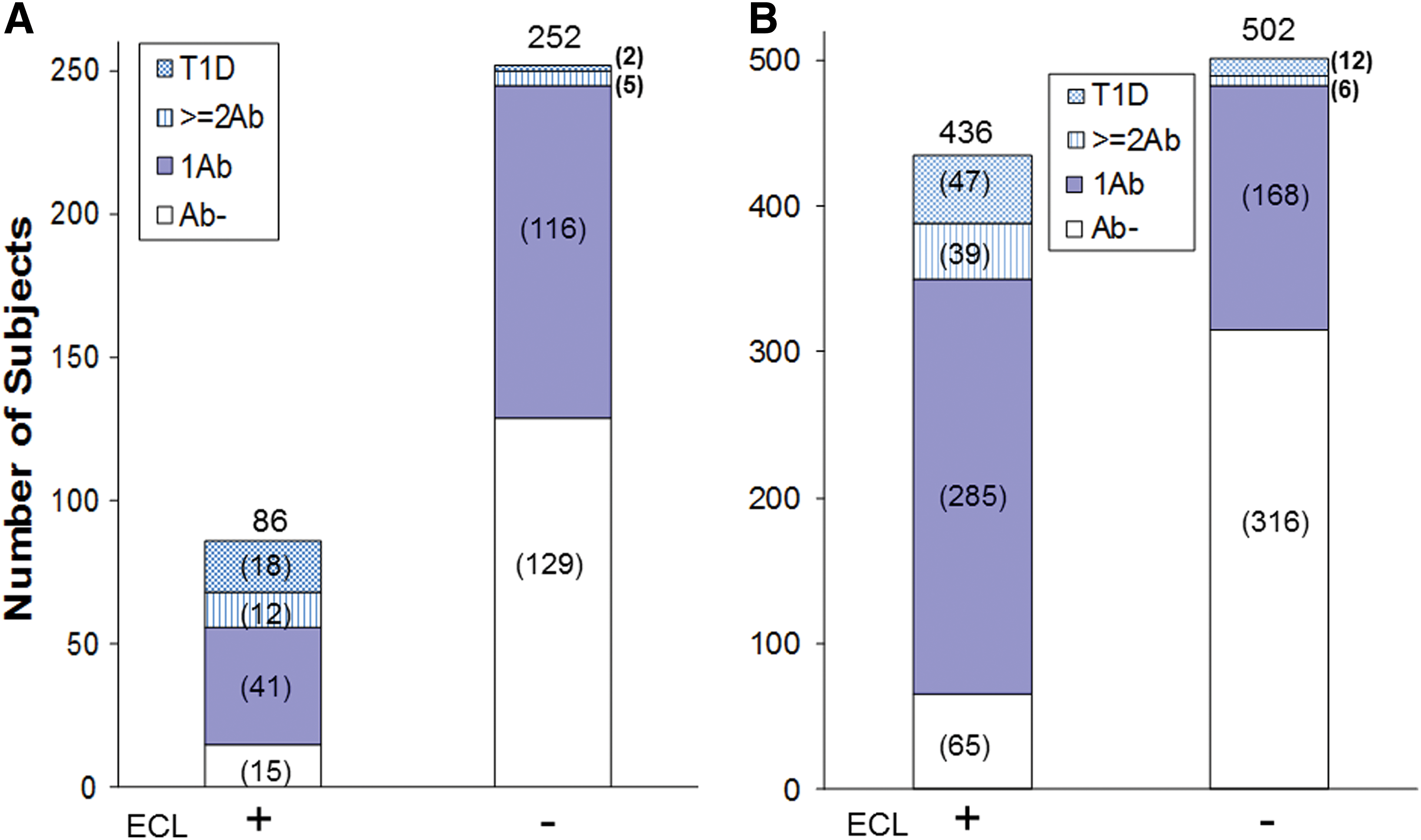
Prospective clinical follow-up on the subjects who were single islet antbody positive for their most recent status of development of islet authoantibodies and progression to type 1 diabetes mellitus (T1D).
ECL-IAA and ECL-GADA improve risk prediction even among subjects with multiple iAbs
Diabetes-free survival was significantly shorter among subjects with multiple iAbs who were ECL-IAA positive, but negative for RAD-IAA, compared with those who were RAD-IAA positive but negative for ECL-IAA (P<0.019) (Fig. 5A). By 6 years of follow-up, over 40% of subjects in the former group, compared with 10% in the latter, had progressed to clinical T1DM. This difference was age dependent and limited to children under 10 years of age (P=0.004) (data not shown).
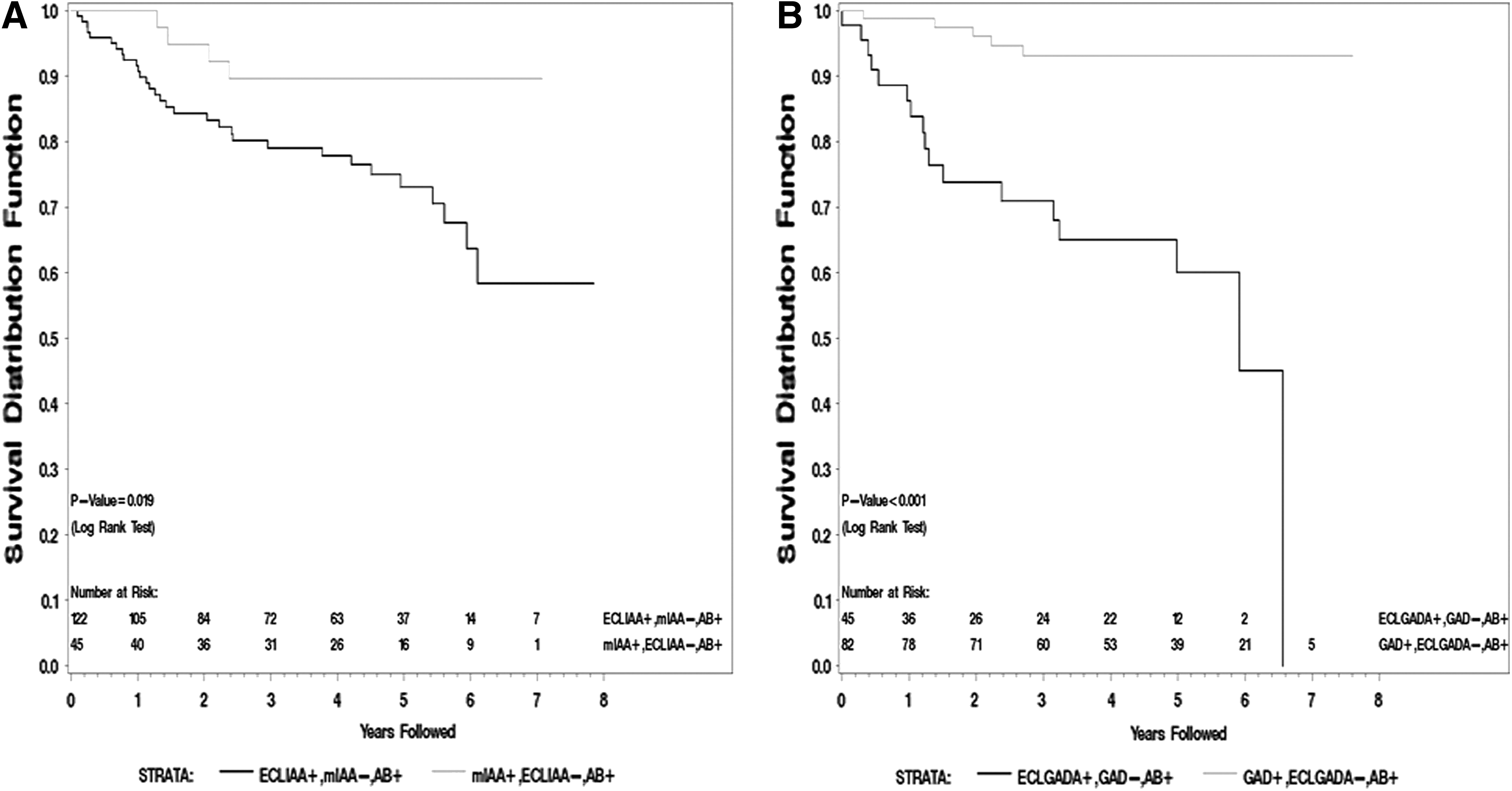
Type 1 diabetes mellitus survival distribution analysis for the subjects with multiple (m) islet autoantibodies (AB):
Diabetes-free survival was also significantly shorter among subjects with multiple iAbs who were ECL-GADA positive, but negative for RAD-GADA, compared with those who were RAD-GADA positive but not confirmed by ECL-GADA (P<0.001) (Fig. 5B). By 6 years of follow-up, approximately 40% of subjects in the former group, compared with 7% in the latter, had progressed to clinical T1DM. This difference appeared to present at all ages and was a bit stronger in children 10–19 years of age (data not shown).
Both ECL-IAA and -GADA have higher predictive values
Among a total of 3,484 TrialNet samples in this study, the 2,944 belong to the very first initial TrialNet screening samples, and 340 have developed T1DM after up to an 8-year prospective follow-up. The positive and negative predictive values of the ECL and RADs are summarized in Figure 6. The positive predictive values for both ECL-IAA (32%, 186/575) and ECL-GADA (24%, 273/1,146) were significantly higher than those RAD-IAA (21%, 164/765; P<0.0001) and RAD-GADA (16%, 267/1,702; P<0.0001), respectively (Fig. 6A). The negative predictive values for both ECL-IAA (94%) and ECL-GADA (96%) were significantly higher than those for RAD-IAA (92%; P<0.05) and RAD-GADA (94%; P=0.007), respectively (Fig. 6B). The positive and negative predictive values of ECL-IAA and -GADA combined together were also significantly higher than the two RADs combined (P<0.0001 and P=0.01, respectively).
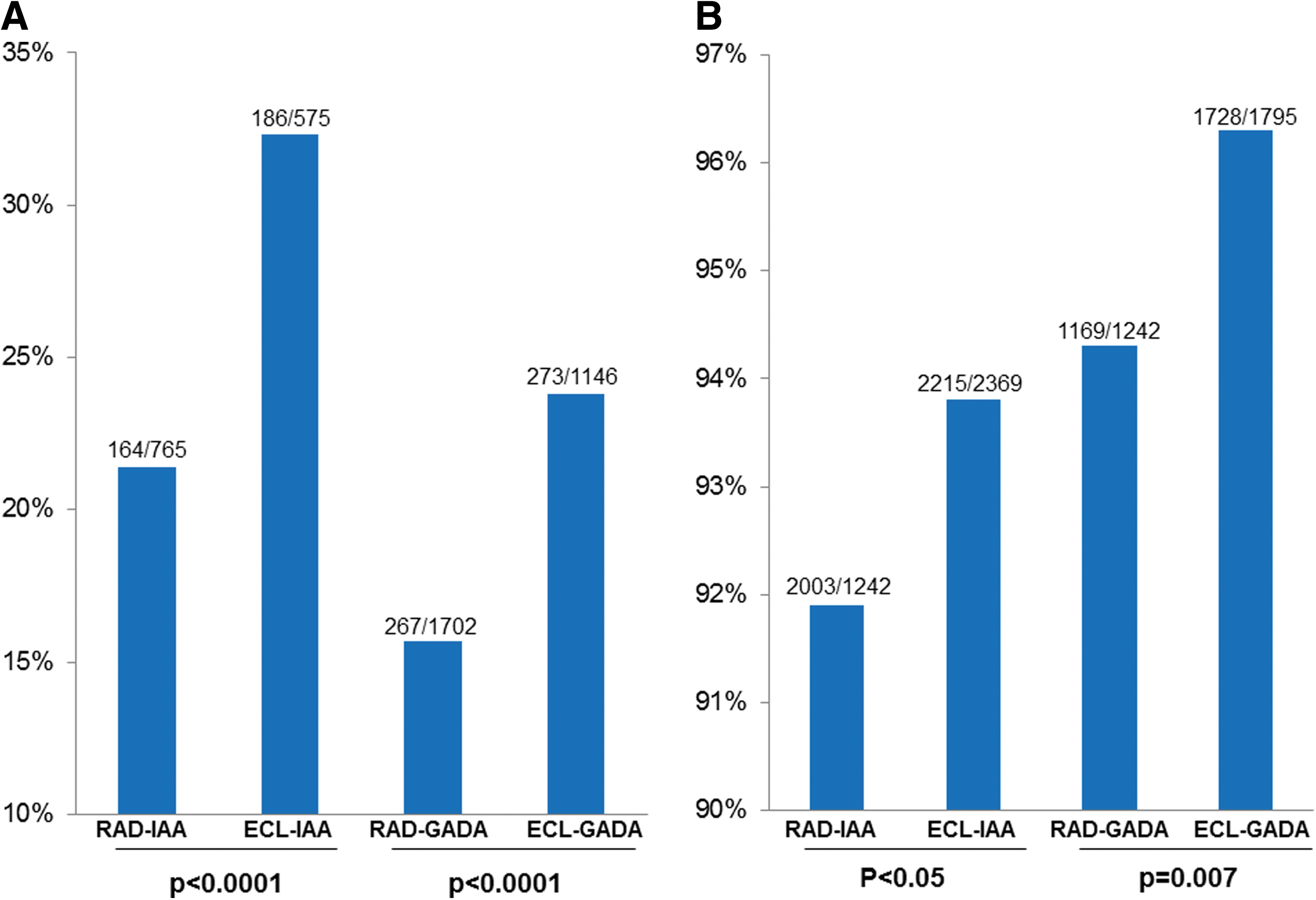
Comparison of predictive values between electrochemiluminescence (ECL) and radioassay (RAD) on 2,944 subjects for their very first initial screening samples in TrialNet Pathway to Prevention Study: comparison of
ECL-IAA and ECL-GADA are more strongly associated with the high-risk genotype HLA DR3/4 than the RAD-IAA and RAD-GADA
Of all subjects participating in this study, 1,107 were genotyped for HLA-DR and DQ. The prevalence of the highest-risk genotype, DR3/4, DQB1*0302, by study group is summarized in Figure 7. In this study population, the prevalence of the DR3/4, DQB1*0302 genotype was similar among subjects who had diabetes (28.2%) or were positive for multiple iAbs (26.5%) at the end of their follow-up. In contrast, the DR3/4, DQB1*0302 genotype was present in only 12.8% of subjects with a “single” iAb and in 12.7% of those negative for all four iAbs (P<0.0001, compared with those positive for multiple iAbs). In line with their high risk of diabetes, subjects with RAD-IAA confirmed by ECL-IAA more often had the DR3/4, DQB1*0302 genotype than those negative for ECL-IAA (24.5% vs. 11.3%; P<0.0017). Similarly, subjects with RAD-GADA confirmed by ECL-GADA had the highest-risk HLA more often than those negative for ECL-GADA (23.1% vs. 9.6%; P<0.0001).

A subanalysis of subjects with “single” iAbs by radioassay showed higher prevalence of the DR3/4, DQB1*0302 genotype in those confirmed by ECL, although the difference has not reached statistical significance among subjects with “single” IAA.
The association with younger age is stronger for ECL-IAA than RAD-IAA
In this study population, the mean age at the initial detection of iAb positivity was similar among subjects who had diabetes (15.0 years) or were positive for multiple iAbs (14.0 years) at the end of their follow-up (Fig. 8). In contrast, subjects with a “single” iAb (23.0 years) or those negative for all four iAbs (26.7 years) were, on average, significantly older. In line with their high risk of diabetes, the subjects with RAD-IAA confirmed by ECL-IAA were younger (12.0 years) than those negative for ECL-IAA (21.7 years) (P<0.0001). Similarly, the subjects with RAD-GADA confirmed by ECL-GADA were younger (19.3 years) than those negative for ECL-GADA (22.0 years) (P<0.0001).
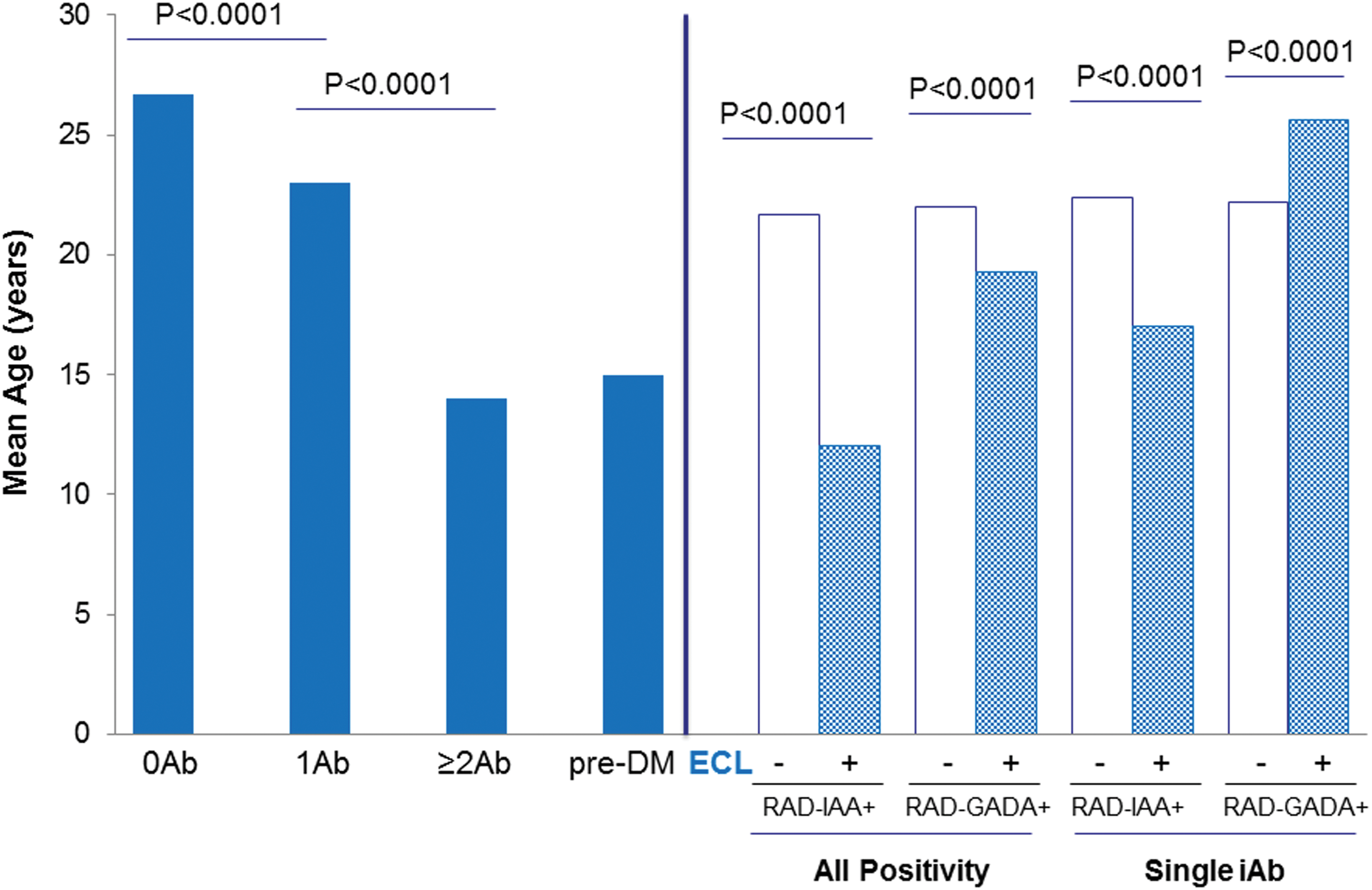
A subanalysis of the subjects with “single” RAD-IAA showed a younger age of those confirmed by ECL-IAA (17.0 years) than those not confirmed (22.4 years) (P<0.0001). Subjects with “single” RAD-GADA confirmed by ECL-GADA were older (25.6 years) than those negative for ECL-GADA (22.2 years) (P<0.0001).
Discussion
These results from the large study in well-characterized TrialNet participants provide strong evidence for an added value of ECL-IAA and ECL-GADA assays, compared with the currently used “gold standard” RAD-IAA and RAD-GADA. The ECL-based assays demonstrate better predictive ability in assessing the risk of progression to T1DM in subjects with iAbs. These results are remarkably consistent with those previously published using samples from the DASP, the Diabetes Autoimmunity Study in the Young (DAISY), and the clinic population at the Barbara Davis Center. Both ECL-IAA and -GADA assays were able to discriminate high-risk iAbs in pre-T1DM children and in children with multiple iAbs from low-risk iAbs often detected as a “single” iAb by RADs. 11,13
The large sample size and up to 8-year follow-up of this TrialNet cohort made it possible to analyze discordance between ECL and RAD, especially among “single” iAb-positive subjects who were not confirmed by ECL assays. This was not possible in the previous, smaller studies. One of the major findings of this study is the loss of iAb positivity in most of these “single” iAb-positive subjects not confirmed by ECL, in contrast to only approximately 15% loss in those confirmed by ECL. It comes with a caveat that the follow-up time was limited for most of these subjects (median, 1.5 years). However, despite the short follow-up, 20–35% of the ECL-confirmed “single” iAb subjects progressed to multiple iAbs or T1DM; the progression rate in the absence of ECL confirmation was only 3%. These results support our hypothesis 11 that most of the “single” IAA or GADA detected only by radioassay are low-affinity antibodies, perhaps resulting from immunization with a cross-reactive molecule. This is consistent with previous reports from other laboratories 2 –5 that both IAA and GADA in children who remained single autoantibody positive or became iAb negative had a significantly lower affinity than IAA and GADA in multiple antibody-positive children. No affinity maturation was observed for IAA from seroconversion to T1DM diagnosis. 5 ECL-IAA and especially ECL-GADA may help to distinguish autoimmune T1DM from other forms of diabetes among subjects with a single iAb.
It is well known that people with multiple iAbs are at high risk of progression to T1DM. A recent international collaborative study demonstrated that young children with two or more iAbs had 70% risk of progression to clinical T1DM in 10 years of follow-up. 1 However, in the present study, we unexpectedly found that the risk was much lower, perhaps only 10%, if RAD-IAA and RAD-GADA could not be confirmed by ECL in multiple iAb-positive subjects. It could be partially explained by the higher prevalence of subjects positive for three or more iAbs (IAA, GADA, IA-2A, and ZnT8A) among subjects with ECL-confirmed IAA (57%) or GADA (60%) than among those not confirmed by ECL (37% [P=0.03] and 20% [P=0.0001], respectively). Accordingly, previous studies showed that T1DM risk increases with greater number of iAbs even among subjects with multiple iAbs. 6,14 The higher risk of T1DM with increasing number of iAbs may also reflect faster progression to T1D or that subjects with more iAbs are closer to clinical T1DM.
Our findings of higher prevalence of the high-risk HLA-DR3/4, DQB1*0302 genotype and younger age in subjects with iAbs confirmed by ECL provide additional evidence for disease specificity of the new ECL assays. IAA is the only iAb found to be significantly associated with age 16 –18 : inversely correlated with age for both level and prevalence. IAA is usually the first iAb to appear in early life 2,12 to mark the initiation of islet autoimmunity. Our previous study found that ECL-IAA antedated the onset of islet autoimmunity by a mean of 2.3 years (range, 0.3–7.2 years) in high-risk young children followed to clinical diabetes. 12 Consistent with this finding, 15% of subjects in the present study who were initially ECL-IAA-positive and RAD-IAA-negative later become RAD-IAA-positive (data not shown), but we lack ECL-IAA data on these follow-up samples. The number of young children in the present study was limited, and this issue will be better addressed in the TEDDY study. 19
In conclusion, both ECL-IAA and -GADA assays are more diabetes-specific, compared with their corresponding RADs, with higher positive predictive values and the ability to exclude “single” transient iAbs that are not associated with T1DM in most cases.
Footnotes
Acknowledgments
The sponsor of the trial was the Type 1 Diabetes TrialNet Study Group, a clinical trials network funded by the National Institutes of Health through the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institute of Allergy and Infectious Diseases, and The Eunice Kennedy Shriver National Institute of Child Health and Human Development, through the cooperative agreements U01 DK061010, U01 DK061016, U01 DK061034, U01 DK061036, U01 DK061040, U01 DK061041, U01 DK061042, U01 DK061055, U01 DK061058, U01 DK084565, U01 DK085453, U01 DK085461, U01 DK085463, U01 DK085466, U01 DK085499, U01 DK085505, and U01 DK085509 and contract HHSN267200800019C; by the National Center for Research Resources, through Clinical Translational Science Awards UL1 RR024131, UL1 RR024139, UL1 RR024153, UL1 RR024975, UL1 RR024982, UL1 RR025744, UL1 RR025761, UL1 RR025780, UL1 RR029890, UL1 RR031986, and P30 DK017047 and General Clinical Research Center Award M01 RR00400; by the JDRF; and by the American Diabetes Association. This study was also supported by grant DK32083 from the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
D.M., K.M.G., L.J., T.A., and S.M.M. researched data and reviewed the manuscript. A.K.S., L.Z., and M.R. reviewed/edited the manuscript. J.K. analyzed data and reviewed the manuscript. L.Y. researched data and wrote the manuscript. L.Y. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.