
Abstract
Background:
Insulin is an essential therapy for patients with type 1 diabetes mellitus (T1DM). With the progression of the disease, many patients with T1DM may have an increased prevalence of insulin resistance; thus the common standard insulin therapy requires a high insulin dosage (>1 unit/kg/day) and is usually associated with many side effects. Studies have shown that metformin may benefit those insulin-resistant individuals with T1DM. This meta-analysis was performed to provide the evidence of clinical efficacy and safety of metformin in T1DM.
Materials and Methods:
We conducted a search on Medline, EMBASE, and the Cochrane Library for relevant studies published before May 2014 based on “metformin” and “diabetes mellitus, type 1.” The following outcomes were evaluated: hemoglobin A1c (HbA1c), fasting plasma glucose (FPG), lipid metabolism, weight, insulin dosage, hypoglycemia, diabetic ketoacidosis, or gastrointestinal adverse events (AEs). The meta-analysis was performed using Review Manager version 5.2 software (The Nordic Cochrane Centre, Copenhagen, Denmark).
Results:
In total, eight randomized controlled trials were included. Metformin was associated with a reduction in daily insulin dosage, body weight, total cholesterol level, low-density lipoprotein level, and high-density lipoprotein level but an increase in risk of gastrointestinal AEs compared with placebo treatment in T1DM patients. No significant difference was found between the metformin group and the placebo group in HbA1c level, FPG level, or triglycerides level. No significant difference was found between the metformin group and the placebo group in the risk of severe hypoglycemia or diabetic ketoacidosis.
Conclusions:
Metformin may decrease the daily insulin dosage, body weight, and lipid levels in T1DM. However, metformin does not increase the incidence of hypoglycemia and ketoacidosis. High-quality, large-sample, and long-term follow-up clinical trials are needed to confirm these conclusions.
Introduction
T
The Diabetes Control and Complications Trial 1 and its follow-up observations 2 have shown that intensive glucose control was associated with significant long-term reduction in both microvascular and macrovascular complications in T1DM patients. However, many patients could not reach the recommended target in hemoglobin A1c (HbA1c) levels during the insulin therapy. The reason was that achieving and maintaining such a target by the common standard insulin therapy strategy required high daily insulin dosage (>1 unit/kg/day). 3 The literature revealed that a high insulin dosage was often associated with increased risk of hypoglycemia, weight gain, and, in some cases, the aggravation of cardiovascular risk factors, including dyslipidemia. 4
Metformin is the first-line oral hypoglycemic agent commonly used in the treatment of type 2 diabetes mellitus (T2DM). 5 It decreases the glucose level primarily by suppressing hepatic glucose production (hepatic gluconeogenesis). Metformin improve glycemic control with modest weight loss, which could be beneficial to the reduction of diabetes-related complications. 6 –8 Based on the positive effects of metformin from the studies in T2DM, we therefore propose that metformin may benefit those insulin-resistant T1DM patients whose daily insulin requirement was more than 1 unit/kg of body weight. 3 We also propose that metformin may produce a better control of glucose and lipids with less weight gain and a reduced daily insulin dosage.
To investigate and provide an up-to-date and comprehensive picture of the clinical efficacy and safety of metformin in T1DM, we conducted this meta-analysis to provide the evidence that metformin might be prescribed for some patients with T1DM.
Materials and Methods
We captured all relevant studies published before May 2014 in Medline, EMBASE, and the Cochrane Library based on the following search terms as medical subject headings: (1) “metformin” and (2) “diabetes mellitus, type 1” or “type 1 diabetes” or “insulin dependent diabetes.”
We included the studies in this meta-analysis if (1) they were randomized controlled trials, (2) the duration of treatment was ≥12 weeks, (3) they used a parallel design or crossover design of metformin versus placebo treatment, and (4) they reported data on HbA1c change, fasting plasma glucose (FPG) change, lipid metabolism, weight change, insulin dosage, hypoglycemia, or diabetic ketoacidosis, or gastrointestinal adverse events (AEs) were investigated.
Abstracts of cited articles were reviewed by two independent investigators (X.Z. and P.L.) to determine the relevance. Disagreements were resolved through discussion and consensus or, as needed, with a third investigator (L.L.) and confirmed by consensus. When there were multiple articles from the same trial, the most complete and recently reported data were used. The quality of included articles was further assessed using the criteria of Jadad et al. 9 The score range was from 0 to 5 (a high score indicating high quality).
The statistical analysis was performed with Review Manager version 5.2 (The Nordic Cochrane Centre, Copenhagen, Denmark) from the Cochrane Collaboration (2013). Continuous variables were analyzed using the weighted mean differences (MD) under general circumstances but standardized MD for different units of measurement, whereas categorical dichotomous variables were assessed using relative risks (RR). A P value of<0.05 was considered to be statically significant, and 95% confidence intervals (CI) were reported. Homogeneity was tested by the Q statistic (significance level at P<0.10) and the I 2 statistic (significance level at I 2>50%). 10 A random-effects model was used if the Q or I 2 statistic was significant. Otherwise, a fixed-effects model was used.
Results
The initial literature search retrieved 340 relevant articles. Two hundred and one articles were excluded after the titles were scanned. One hundred and twenty-one articles were excluded after the abstracts were carefully read. Then, 10 articles were excluded for various reasons (duplicate, review, case report, no required data), and finally eight randomized controlled trials were retained for meta-analysis (Fig. 1). 3,11 –17 Pooled analysis included 300 patients. Overall, included studies were of adequate methodologic quality (mean Jadad score of 3.5 for included studies; all of the eight studies had a score of ≥3). Included studies, basic characteristics of enrolled patients, and details on drug therapy are presented in Table 1.

Flowchart demonstrating process of study selection.
F, female; M, male; MET, metformin; PL, placebo.
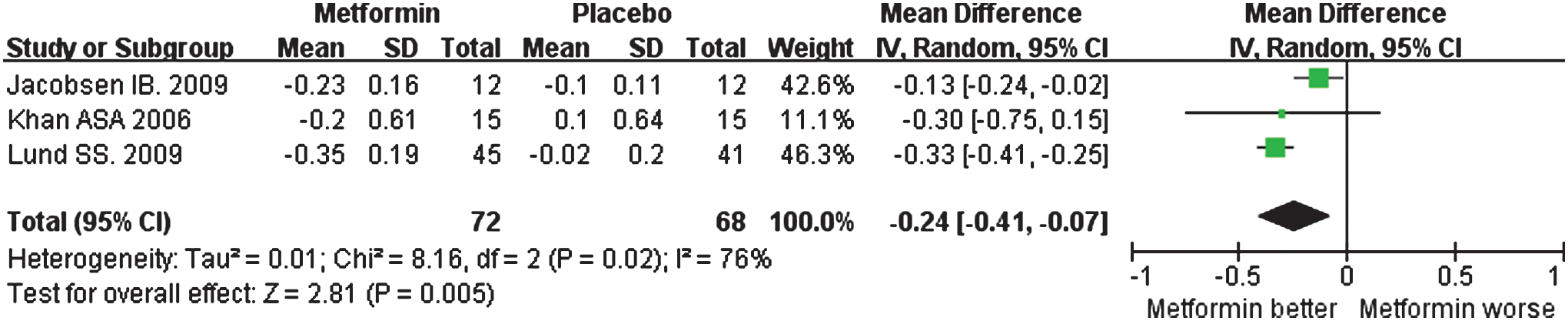
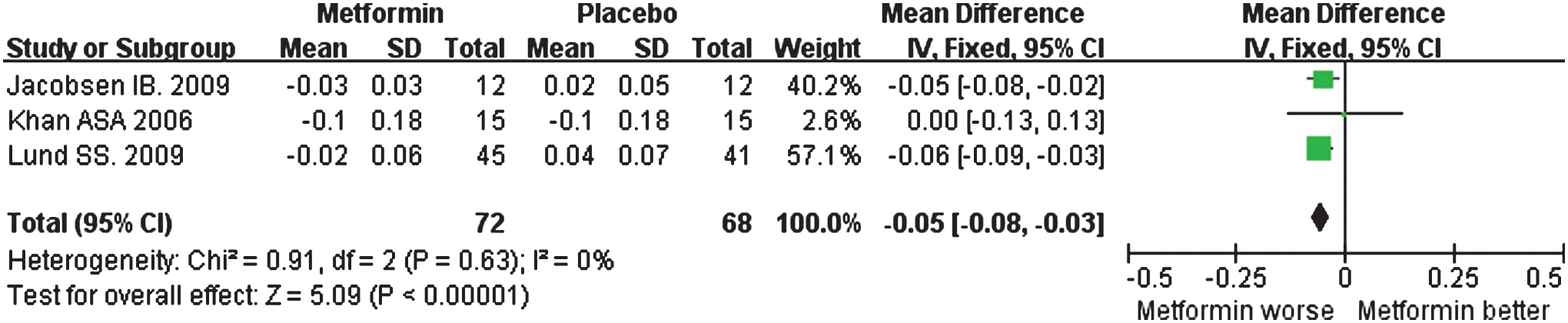
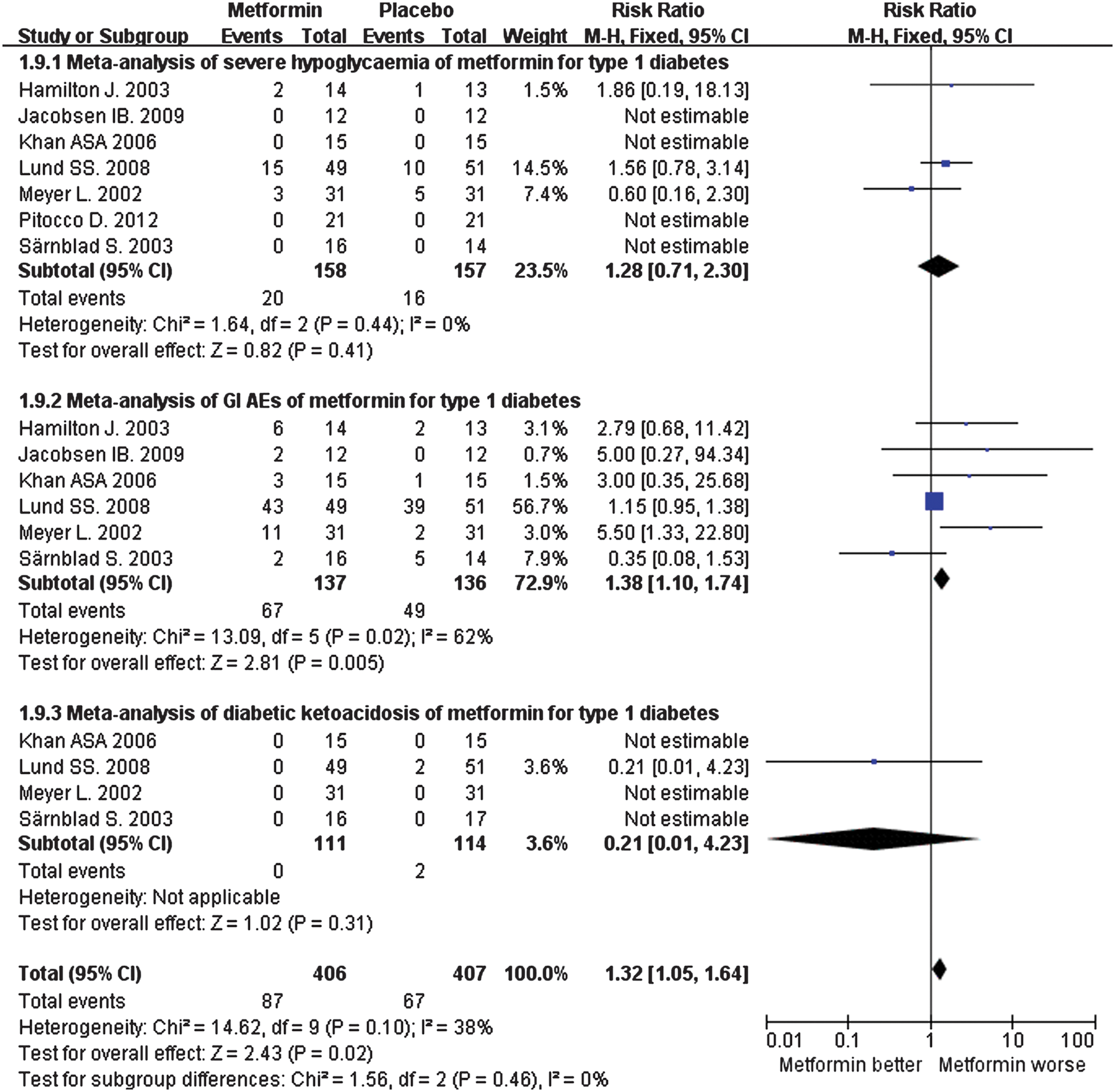
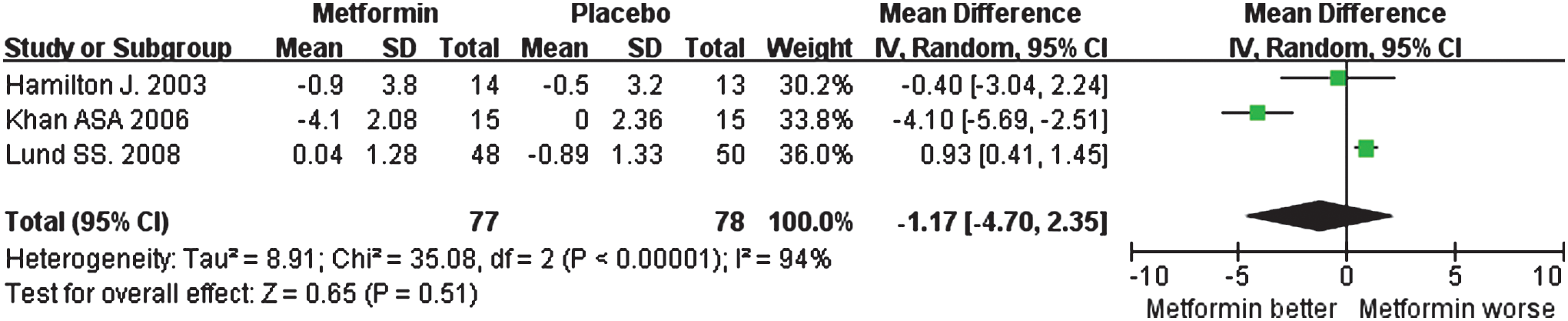
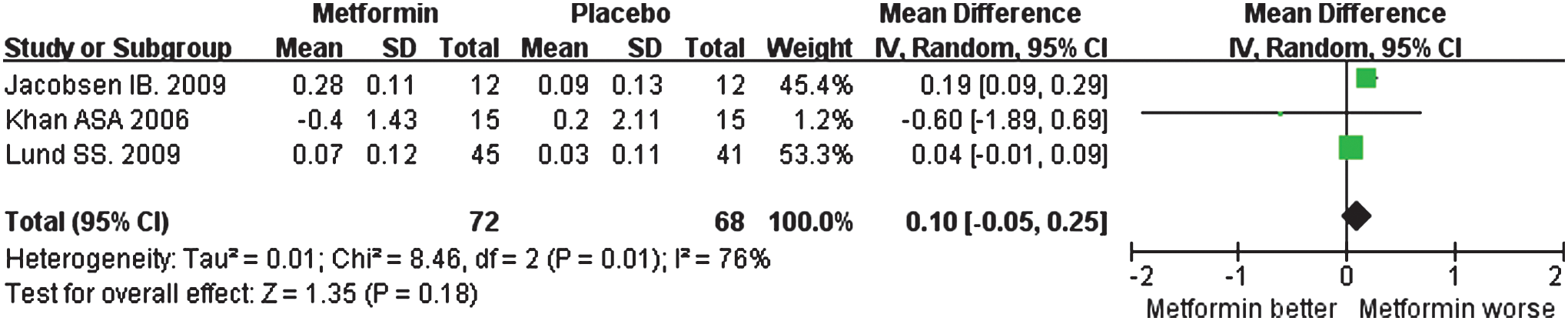
The results of meta-analysis showed that metformin was associated with a reduction in daily insulin dosage (in units/day) (MD=−1.36; 95% CI, −2.28 to −0.45; P=0.004) (Fig. 2), lower body weight (in kg) (MD=−2.41; 95% CI, −4.17 to −0.65; P=0.007) (Fig. 3), lower total cholesterol level (in mmol/L) (MD=−0.25; 95% CI, −0.46 to −0.05; P=0.02) (Fig. 4), lower low-density lipoprotein level (in mmol/L) (MD=−0.24; 95% CI, −0.41 to −0.07; P=0.005) (Fig. 5), and lower high-density lipoprotein level (mmol/L) (MD=−0.05; 95% CI, −0.08 to −0.03; P<0.00001) (Fig. 6) but an increase in the risk of gastrointestinal AEs (RR=1.38; 95% CI, 1.10–1.74; P=0.005) (Fig. 7) compared with placebo treatment in T1DM patients. No significant difference was found between the metformin group and the placebo group for the HbA1c level (%) (MD=−0.20; 95% CI, −0.45 to −0.05; P=0.11) (Fig. 8), FPG level (in mmol/L) (MD=−1.17; 95% CI, −4.70 to 2.35; P=0.51) (Fig. 9), and triglycerides level (in mmol/L) (MD=0.10; 95% CI, −0.05 to 0.25; P=0.18) (Fig. 10). No significant difference was found between the metformin group and the placebo group in the risk of severe hypoglycemia (RR=1.28; 95% CI, 0.71–2.30; P=0.41) (Fig. 7) or diabetic ketoacidosis (RR=0.21; 95% CI, 0.01–4.23; P=0.31) (Fig. 7).




Discussion
We found only eight randomized studies of metformin therapy in T1DM, which were small samples. Nonetheless, the meta-analysis results showed that metformin produced greater reduction in daily insulin dosage, body weight, total cholesterol, and low-density lipoprotein than placebo. However, metformin showed lower high-density lipoprotein and higher risk of gastrointestinal AEs compared with placebo. No significant difference was found between metformin and placebo for HbA1c, FPG, and triglycerides levels or the risk of severe hypoglycemia and diabetic ketoacidosis. Another meta-analysis has obtained similar results. 18
Metformin was thought to improve the reduced insulin sensitivity in overweight subjects, 19 prediabetes, 20 patients with T2DM, 21 and patients with T1DM. 22 In our meta-analysis, metformin administration significantly decreased the daily insulin dose requirement, indicating that metformin might improve the insulin sensitivity in T1DM. There was no significant effect on HbA1c and FPG, which might be expected as patients would tend to adjust their insulin dosage toward their usual HbA1c and FPG levels. Although several potential benefits on glycemic control have been reported in different studies, 10,12,17,23 there is little evidence that metformin has any significant effect on HbA1c or FPG in T1DM.
Patients with T1DM and T2DM showed a significant prior risk of cardiovascular disease compared with the group without diabetes. 24 In the group without diabetes as well as in patients with diabetes, dyslipidemia is an important cardiovascular disease risk factor. 25 In our meta-analysis, we found metformin has been associated with a reduction in total cholesterol and low-density lipoprotein levels, and we speculate that metformin may reduce the risk of cardiovascular disease. Only one 17 of our included studies reported cardiovascular AEs: two patients with two events in the metformin group versus four patients with five events in the placebo group (not a significant difference). Metformin has been definitively found to reduce cardiovascular events in T2DM, 26,27 whereas in T1DM, metformin has been proposed to have beneficial effects on cardiovascular risks, but this needs to be further proven. 28 Another double-blind, randomized, placebo-controlled trial will provide important information on a potential intervention of metformin to improve cardiovascular morbidity and mortality in children with T1DM at high risk from cardiovascular disease. 29
In order to reduce gastrointestinal AEs, medication (metformin or placebo) in all studies was taken during or at the end of meals. Although a higher gastrointestinal AE risk was shown in the metformin treatment group in patients with T1DM, only four patients in the metformin group in all eight studies were withdrawn because of digestive symptoms. 3,15 We therefore concluded that the gastrointestinal AEs of metformin can be tolerated in most patients with T1DM. The differences were not statistically significant in severe hypoglycemia and diabetic ketoacidosis. Based on the results in our analysis, we concluded that metformin administration was safe in combination with insulin therapy in patients with T1DM.
Eight included studies met the inclusion criteria, with a mean Jadad score of 3.5. Therefore the conclusions of this systematic analysis are reliable.
In summary, metformin, which may possibly decrease the risk of cardiovascular events, was safe and effective in patients with T1DM. It could be a credible alternative for T1DM patients who are on high daily insulin dosage and with a high risk of hypoglycemia, obvious body weight gain, and possibly high risk of cardiovascular exposure during the monoinsulin therapy. More high-quality, large-sample, further long-term follow-up, randomized, multicenter clinical trials are needed to confirm our results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.