
Abstract
Intensive insulin therapy (IIT) has been shown to reduce micro- and macrovascular complications in patients with type 1 diabetes mellitus (T1DM). However, IIT is associated with a significant increase in severe hypoglycemic events, resulting in increased morbidity and mortality. Optimization of glycemic control without hypoglycemia (especially nocturnal) should be the next major goal for subjects on insulin treatment. The use of insulin pumps along with continuous glucose monitors (CGMs) has made it easier but requires significant resources and patient education. Research is ongoing to close the loop by integrating the pump and the CGM using different algorithms. The currently available closed-loop system is the threshold suspend. Steps needed to achieve a near-perfect closed-loop are (1) a control-to-range system that will reduce the incidence and/or severity of hyper- and/or hypoglycemia by adjusting the insulin dose and (2) a control-to-target system, a fully automated or hybrid system that sets target glucose levels to individual needs and maintains glucose levels throughout the day using insulin (unihormonal) alone or with other hormones such as glucagon or possibly pramlintide (bihormonal). Future research is also focusing on better insulin delivery devices (pumps), more accurate CGMs, better predictive algorithms, and ultra-rapid-acting insulin analogs to make the closed-loop system as physiological as possible.
Introduction
A
Intensive insulin therapy (IIT) (using multiple daily injections [MDI] or continuous subcutaneous insulin infusion [CSII]) has been shown to reduce the long-term micro- and macrovascular complications in patients with T1DM and T2DM. 3,4 However, IIT increases the risk for severe hypoglycemia by threefold. 5
Incidence rates of hypoglycemia as a result of IIT range from 115 to 320 events per 100 patients with T1DM. 6 In a study in patients with T1DM, hypoglycemic events occurred for 8.5% at night, and hypoglycemia lasting for at least 2 h was present in 23% at night. 7 More recently, it was realized that not only is hypoglycemia a problem in children and adolescents, it is more common in older patients with diabetes receiving insulin treatment. In a recent study, 97,648 emergency visits per year were attributed to insulin-induced hypoglycemia, and the occurrence of hypoglycemic events was two times higher in individuals more than 80 years of age, 8 resulting in an estimated $640 million cost in healthcare expenditures. Hypoglycemia in adults also increases the risk of cardiovascular events and may pose a higher risk of cognitive deficits in children. 9,10 Approximately 4–6% of deaths among patients with T1DM are attributed to severe hypoglycemia. 11 Contrary to the Diabetes Control and Complication Trial (DCCT) findings, recent studies have revealed that hypoglycemia occurs with similar frequency across all A1C values in all age groups 12 and is the major limiting factor in implementing IIT.
With the introduction of newer long-acting insulin analogs such as insulin glargine, insulin detemir, and insulin degludec (not approved in the United States), hypoglycemic events have been significantly reduced compared with previous generations of intermediate-acting insulins such as neutral protamine Hagedorn (NPH) and ultralente (now discontinued worldwide). 13 However, severe hypoglycemia, especially nocturnal, continues to be a risk with IIT. Despite advances in technology and the availability of insulin pumps and continuous glucose monitors (CGMs), most youths with T1DM do not meet American Diabetes Association or International Society for Pediatric and Adolescent Diabetes glycemic goals. 14 The open-loop insulin delivery system is subject to human error and can result in unexpected hypo- and/or hyperglycemic events. Hence, closing the loop by integrating insulin pumps and sensors by using appropriate algorithms provides a promising approach to reduce nocturnal hypoglycemia, meal-related hyperglycemia, and wide glucose excursions (glycemic variability). This review discusses progress towards closed-loop (CL) therapies and highlights the future steps needed to imitate the human pancreas (artificial pancreas/bionic pancreas).
History of the Artificial Pancreas (CL System)
The discovery of insulin in 1921 is one of the great advances of the 20th century, and its availability has reduced morbidity and mortality in patients with T1DM significantly. Self-injections of multiple doses of short- or rapid-acting insulin along with one or two injections of long-acting insulin are usually referred to as MDI. Because the early short-acting insulins were derived from bovine and porcine pancreata, they were limited by requiring multiple daily injections, immunological reactions, lipodystrophy, and unpredictable hypoglycemic and hyperglycemic events. 15 Early developments focused on insulin purification, different formulations, and prolonging the duration of action. With the introduction of long-acting insulins in the 1930–1940s (protamine zinc insulin and NPH), patients were able to take one or two injections of long-acting insulin and three or more injections of short-acting insulin a day for optimal glycemic control. 15 The DCCT established the usefulness of IIT (MDI or CSII) in the management of diabetes. 3 However, early insulins used in the DCCT were limited by marked inter-and intra-individual variability and nocturnal hypoglycemia as a result of peak action at 4–6 h, which made it difficult to achieve desired glucose control. The currently available rapid-acting (insulin lispro, insulin glulisine, insulin aspart) and long-acting (insulin glargine, insulin detemir) insulin analogs have better pharmacokinetics and pharmacodynamics properties than earlier insulins and have been shown to reduce the occurrence of hypoglycemic events while maintaining or improving glycemic control. 15
The first insulin pump developed by Kadish 16 in 1964 was large in size and included an autoanalyzer to measure blood glucose. However, it was impractical to use this device and did not receive much attention. In early 1980, the first computerized insulin delivery device was made (Biostator; Miles Laboratories, Elkhart, IN). It was also impractical to use this large device on a daily basis. 17 Most of the Biostators are now used for early pharmacokinetics/pharmacodynamics studies of developing insulin analogs. Between 1965 and1980, several companies made different devices for insulin delivery and blood glucose measurements. The timeline development of various insulin delivery and glucose monitoring systems is provided in Figure 1.
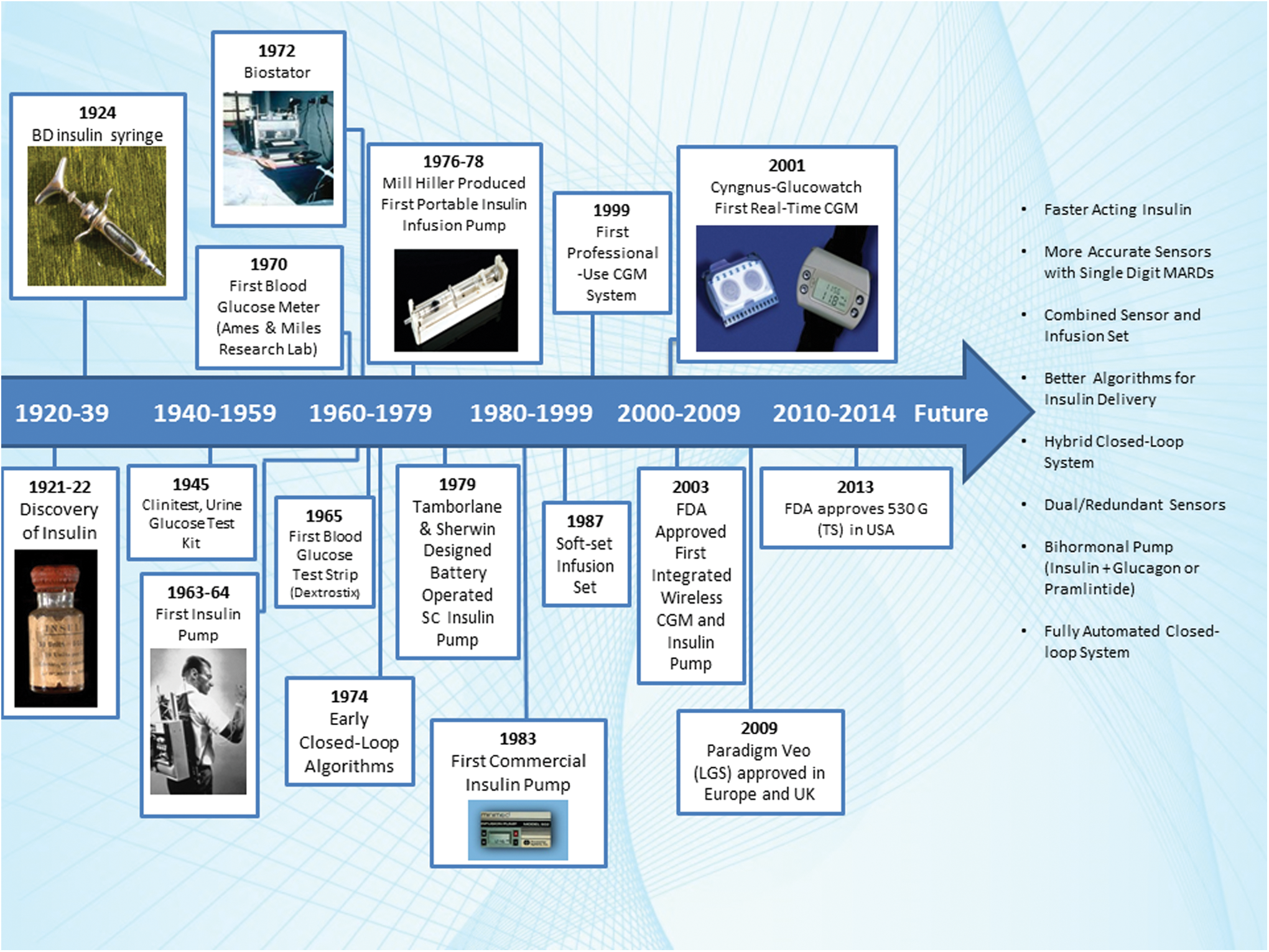
Roadmap of the discovery of insulin delivery and glucose monitoring devices leading to the closed-loop system. CGM, continuous glucose monitor; FDA, Food and Drug Administration; LGS, low glucose suspend; MARD, mean absolute relative difference; SC, subcutaneous; TS, threshold suspend. Color images available online at
Earlier insulin pumps were large in size, imprecise, and limited by technical issues. Since the first commercial pump (1983), there have been constant modifications in size, shape, functionality, delivery cannula, and smart basal and bolus features. The current generation of pumps with their small size and smart features, such as built-in dose bolus calculators and alarms, has increased the adoption of pump therapy by both patients and providers. 18
In 1970 it was shown for the first time that self-monitoring of blood glucose (SMBG) improved glycemic control in patients with diabetes, and since then SMBG has become the standard of care. 19 With advances in technologies, newer glucose meters are smaller in size, require less blood for glucose measurement, and are more accurate. Finger-stick glucose measurements are single-point blood glucose estimations, and patients have to prick their fingers multiple times a day in order to obtain glucose values at different points of the day. This limitation led to the development of CGMs in the late 1990s. 19 Like SMBG, the new-generation CGMs are more accurate and smaller in size and have been shown to improve glycemic control while decreasing hypoglycemia in patients with T1DM. 20 The CGM use in patients using an insulin pump or MDI has been shown to improve glycemic control, provided that the CGM is used frequently (more than 5 days/week). 21 –23
Since the availability of CGMs, there have been efforts to connect the insulin pump and CGM wirelessly, and by using various algorithms, insulin delivery can be optimized without human interference. The first semiautomatic CL system (the MiniMed Paradigm® Veo™ insulin pump; Medtronic MiniMed, Inc., Northridge, CA) has been approved for use in Europe since 2009. The Paradigm Veo, also known as the 530G in the United States, was recently approved by the U.S. Food and Drug Administration; it suspends the insulin delivery for up to 2 h if the user does not acknowledge hypoglycemia. A detailed description of the threshold suspended (TS) pump is provided later.
The Components of a CL System
The CL system has four components: the insulin pump delivering insulin, the CGM providing interstitial glucose values, a finger-stick glucose meter for the calibration of the CGM, and the controller regulating insulin delivery by using algorithms.
CSII (insulin pump)
The development of a portable CSII device was one of the first steps towards the creation of an artificial pancreas (CL system). The insulin pump is a small electromechanical device that continuously delivers basal insulin (at preprogrammed rates based on patient needs) subcutaneously while patients deliver prandial and corrective boluses of insulin. 24 Although initially reserved for patients who required more aggressive glycemic management, CSII use has increased dramatically in recent years because of convenience of use and its smart patient-friendly features. 24 CSII has many advantages over MDI, such as fewer injections, less pain, and increased portability. Furthermore, CSII has been shown to reduce A1C levels and incidences of hypoglycemia and diabetic ketoacidosis and to provide a modest reduction in insulin requirement and higher patient satisfaction compared with MDI. 25 –29 Currently available insulin pumps include the Paradigm 522/722 (Medtronic MiniMed, Inc., Northridge, CA), the 530G, the Accu-Chek® combo (Roche Diagnostics, Indianapolis, IN), the OneTouch® Ping® (Animas Corp., West Chester, PA), the DANA Diabecare IISG (SOOIL Development Co. Ltd., San Diego, CA), the Amigo® (Nipro Diagnostics, Inc., Fort Lauderdale, FL), the OmniPod® (Insulet Corp., Bedford, MA), and the T-Slim (Tandem Diabetes Care, Inc., San Diego, CA), with several more in development.
CGMs
The CGMs include a sensor, transmitter, and receiver. The sensor inserted subcutaneously measures the glucose level in the interstitial fluid. The transmitter relays glucose readings wirelessly to the receiver, which displays the data in real time. The CGM provides significantly more information than SMBG, such as glucose values every 5 min, glucose trends, and alarms. 30 Currently available CGM devices include the Dexcom G4 (Dexcom, Inc., San Diego), the Guardian® REAL-Time (Medtronic), the FreeStyle Navigator® (Abbott Diabetes Care, Alameda, CA) (not marketed in the United States), and the Enlite™ (Medtronic). CGM use has been shown to reduce A1C levels, glycemic variability, and the incidence of hypoglycemia in patients with T1DM using either MDI or CSII. 21,29 –32 Although the first generation CGMs lacked accuracy, new generations of CGMs are more accurate. 33 Despite all the advances in CGM technology, the usage of CGM in T1D patients is less than 9% in the United States, 34 partly due to issues in accuracy, false alarms, and annoyance in wearing two devices.
Blood glucose meters
Currently available CGMs require calibrations using a traditional blood glucose meter (BGM); therefore, a BGM is a fourth component of the CL. However, it is anticipated that improved CGM functionality will not require calibration and that BGMs will no longer be a part of the CL. The currently available BGMs, although accurate, may be influenced by many factors, including improper insertion of the test strip, test strip storage, humidity and temperature, hydration status of patients, unclean hands, and the need for calibration. 35 The error in glucose values from BGMs affects the sensor glucose data. 35
Algorithms
The success of the CL system is dependent on the control algorithms. The algorithms use CGM data to deliver insulin from the insulin pump while accounting for measurement errors, inherent lag times, and kinetic delays. Many algorithms are currently in development. The three main algorithms in use are model predictive control (MPC), proportional-integral-derivative (PID) control, and fuzzy logic.
The MPC uses mathematical models for glucose regulation to control insulin delivery with glucose excursions. These algorithms calculate insulin infusion rates by minimizing the difference between ideal glucose concentrations and the model's forecasted blood glucose levels over a prediction window ranging from 1 to 4 h. 36,37 In this manner, MPC algorithms can be viewed as proactive as they anticipate future glucose trends and administer insulin rather than reacting solely to current data. The MPC algorithms also accommodate for the delay associated with insulin absorption and can account, to some extent, for meal intake and prandial insulin boluses. The MPC algorithms are more commonly used in CL. 37
The PID algorithm continuously adjusts insulin infusion rates by considering three weighted elements of glucose excursion: deviations of the patient's blood glucose level from ideal levels (the proportional component), the area under the curve between ambient and target blood glucose (the integral component), and the rate of change of the patient's blood glucose (the derivative component). 38,39 This algorithm may be considered to be reactive, as it responds to glucose levels, although recent modifications to the PID algorithm incorporating adjustments to insulin delivery based on previously delivered insulin (insulin feedback) make this approach at least partially proactive as well.
The fuzzy logic algorithm, in addition to the model-predicting characteristics of the MPC algorithm, includes the patient's physical characteristics and basal and bolus factors. One such model, the MD-Logic artificial pancreas system (developed at the Institute for Endocrinology and Diabetes, Schneider Children's Medical Center, Tel Aviv, Israel), takes into account an individual patient's treatment characteristics and imitates medical decision-making with respect to glucose control. 40
Besides these three main algorithms, there are additional algorithms being investigated for the CL. All these algorithms are for the unihormonal CL and will need to be adapted when dual-hormonal therapy (insulin and glucagon or insulin and pramlintide) is considered in the CL system.
Further Steps for the Artificial Pancreas
The Food and Drug Administration has recently issued guidelines to carry out the investigations for the development of the artificial pancreas (CL system).
41
The necessary steps are as follows: 1. TS device system. This device suspends the insulin delivery for up to 2 h when the glucose sensor value approaches a predetermined lower threshold (unless the patient overrides the alarm). This device is intended to reduce the incidence and severity of hypoglycemic events.
41
Another system, predictive low glucose suspend (PLGS), suspends insulin delivery before the sensor glucose level reaches the hypoglycemic threshold. 2. Control-to-range system. This system would be designed to reduce the incidence and severity of hypoglycemic and hyperglycemic events by adjusting the insulin dose based on predetermined higher and lower CGM glucose thresholds. This system will still need a patient's involvement to set appropriate basal rates for his or her insulin pump and give a premeal bolus of insulin for glycemic control. 3. Control-to-target system. This system will be automated and/or a hybrid that would set target glucose levels and try to maintain these levels at all times. This system would be fully automated; however, there will always be an option for patients to override the pump and to make changes in the settings. This system will be divided into two subtypes: (a) unihormonal (insulin only) and (b) bihormonal (insulin and either glucagon or pramlintide).
The evidence and rationale for the TS system are discussed below. The other two systems are under investigation, and many clinical studies have been conducted to analyze their feasibility and usefulness in the management of T1DM. The details of the clinical trials are summarized in Table 1.
An up arrow (↑) indicates an increase; a down arrow (↓) indicates a decrease.
AUC, area under curve; BG, blood glucose; CGM, continuous glucose monitor; CL, closed-loop; CSII, continuous subcutaneous insulin infusion; CTR, control to range; DKA, diabetic ketoacidosis; FCL, fully closed-loop; HCL, hybrid closed-loop; Hypo, hypoglycemia; Hyper, hyperglycemia; LGS, low glucose suspend; MD-LAP, MD-Logic artificial pancreas; MPC, model predictive control; NA, not available; NH, nocturnal hypoglycemia; PD, proportional derivative; PID, proportional-integral-derivative; PLGS, predictive low glucose suspend; PPG, postprandial glucose; TS, threshold suspended.
The Current Clinical Evidence for the CL System
Evidence for the use of the TS system
More than half of hypoglycemic events occur at night. 11,42 More than 75% of hypoglycemic seizures in children and 6% of deaths can be attributed to nocturnal hypoglycemia in younger individuals with T1DM. 11 Furthermore, hypoglycemia begets hypoglycemia and makes the situation difficult for the patients and providers. 42 Fear of hypoglycemia is also associated with poor quality of life in both children with T1DM and their parents. Therefore, a reduction of hypoglycemia should be the first objective of the CL system by suspending the insulin delivery at a predetermined low glucose level.
The critical question in creating a TS pump was the duration of insulin suspension that would reduce the severity of hypoglycemia without causing serious hyperglycemia or ketoacidosis. In a study by Pickup et al., 43 basal infusion of regular insulin was deliberately stopped for up to 9 h in a group of pump-treated patients. The investigators noticed a rise in plasma glucose level after 2 h of insulin suspension, and blood ketones started appearing 3 h after insulin suspension. 43 Their observation was followed by several studies that suspended insulin pumps using rapid-acting insulin for 2–3 h with similar results. 44,45 The MiniMed Paradigm Veo insulin pump, commercially available in the Europe since 2009, receives sensor glucose values from the MiniLink™ REAL-time transmitter (Medtronic), and if the CGM glucose level is less than the desired glucose value (adjustable between 60 and 100 mg/dL), the pump suspends insulin delivery for up to 2 h if a hypoglycemia alarm is not acknowledged.
The first clinical trial using a TS pump in 31 patients with T1DM showed that use of a TS pump reduced the duration of severe nocturnal hypoglycemia (defined as ≤40 mg/dL) from 46.2 to 1.8 min/day in those within the highest quartile at baseline with good patient acceptance. 46 In a study by Danne et al., 47 use of the TS pump was found to reduce average hypoglycemic excursions (1.27±0.75 vs. 0.95±0.49 per day) and time spent in hypoglycemia (101±68 vs. 58±33 min/day) compared with the sensor-augmented pump alone. Several other studies have also shown the safety and efficacy of TS for reduction of hypoglycemia, severe nocturnal hypoglycemia, and time spent in hypoglycemia. 48 –50
The Automation to Simulate Pancreatic Insulin Response (ASPIRE-in-Clinic) study established the safety and efficacy of TS in patients with T1DM, 51 which was followed by a large, multicenter, randomized trial (ASPIRE-in-home) in patients with T1DM and showed that the use of the TS pump (also known as 530G) reduced nocturnal hypoglycemic events by 31.8% and decreased the mean area under the curve for nocturnal hypoglycemic events by 37.5% (efficacy) without increasing A1C values (safety). 52 Similarly, another randomized control trial by Ly et al. 53 also demonstrated reduction in the incidence rate of hypoglycemia (9.5 vs. 34.2) with the use of TS compared with an insulin pump alone in patients with T1DM. These studies have established the safety and efficacy of TS in reduction of hypoglycemia, which led to the approval of the 530G in the United States by the U.S. Food and Drug Administration in November 2013.
The PGLS system uses the predictive algorithm to suspend the insulin delivery before the hypoglycemic threshold is reached. In a safety and feasibility study by Buckingham et al. 54 (which used a combination of five different algorithms and a 35-min prediction horizon to discontinue insulin delivery before the glucose threshold of 80 mg/dL was reached) found that the use of PGLS prevented hypoglycemia in 75% of nights. The same group tested the usefulness of PLGS in the home setting and demonstrated a 50% reduction in the frequency of nocturnal hypoglycemia. 55 Similar findings were noted by other studies demonstrating that PGLS was useful in reduction of hypoglycemia in patients with T1DM. 56,57
A multicenter, multinational, randomized, crossover trial evaluated the efficacy of the CL using the fuzzy logic algorithm and changes in insulin delivery based on PLGS in 56 patients with T1DM at a diabetes camp; it was found that PLGS reduced the occurrence of hypoglycemic episodes during the night compared with sensor-augmented pump therapy without any serious adverse events. 58
In summary, clinical trials have shown that both TS and PLGS are safe and effective in reducing nocturnal hypoglycemia and time spent in hypoglycemia. However, there is no clinical trial that compared TS and PLGS to demonstrate superiority of one over the other (Table 1).
Evidence for the control-to-range or control-to-target CL system
The earliest study by Steil et al. 59 carried out 30 h of CL control in 10 patients with T1DM; they reported the time spent in target range had increased to 75% in CL patients compared with 60% in control patients. However, they noticed that the CL system failed to control postprandial glucose excursions. 59 Weinzimer et al. 60 noted similar findings, and they suggested that the hybrid CL with premeal boluses helped to control postprandial glucose excursions. In three randomized crossover studies of 19 patients 5–18 years of age with T1DM using the overnight CL, Hovorka et al. 61 reported increased time spent in target range (70–145 mg/dL; 60% vs. 40%) and reduced time for which glucose concentrations were 70 mg/dL or lower (2.1% vs. 4.1%) in patients using the overnight CL. The same investigators also replicated the CL trial in 24 adult patients with T1DM with similar results. 62 A recent meta-analysis of a Cambridge, United Kingdom cohort of patients with T1DM in overnight CL randomized studies demonstrated that overnight CL increased the time spent in target plasma glucose level and reduced both the time spent below 70 mg/dL and the glycemic variability in both youth and adults compared with conventional CSII. 63 Similar results have been observed by other studies. 64 –66
The AP@home Consortium carried out the first wearable artificial pancreas outpatient study in six subjects with T1DM who underwent a 14-h open-loop followed by 28-h CL experiment. The CL group had more time spent in target range (94.8% vs. 68.2%) and less time spent in hypoglycemia (1.25 vs. 11.9%) during the day with satisfactory overnight control. 67
Exercise-induced hypoglycemia is a challenge in control-to-range CL. Breton et al. 68 conducted a feasibility study where information on heart rate was added in the MPC algorithm; in a randomized crossover trial in 12 subjects with T1DM, heart rate information to control-to-range reduced the significant decline in blood glucose level and yielded fewer hypoglycemic events during exercise. Sherr et al. 69 demonstrated a significant reduction in nocturnal hypoglycemia following daytime exercise in 12 subjects undergoing CL control, compared with an open-loop crossover. The semiautomated CL also had been investigated in pregnant patients with T1DM and patients with T2DM with promising results. 70,71
Dassau et al. 72 carried out a fully automated CL study in subjects with T1DM and found that fully automated CL is feasible and able to keep near-normal blood glucose levels for an average of 70% of the time.
In brief, the semiautomated or hybrid CL is feasible and has been shown to increase time spent with the glucose levels in target ranges without significant hypoglycemia. Large randomized studies on Control-To-Range and Control-To-Target are necessary to document the potential of the CL (Table 1).
Evidence for bihormonal CL system
The bihormonal CL attempts to mimic the glucose-regulating function of the pancreas and is more physiological than unihormonal CL. Kadish 16 first used glucagon in the CL. During the early development of insulin pumps and CL, there was less interest in the use of glucagon because of the instability of the product and the technically challenge of using two hormones in the same system. In addition, the currently available glucagon preparation is not approved for pump use. However, there is renewed interest in making a dual-hormonal CL using glucagon and/or pramlintide.
CL studies have shown that glucagon use is feasible in the CL and can reduce the time spent in hypoglycemia. 73 –75 However, studies also reported that in 20–30% of cases, glucagon was not effective in preventing hypoglycemia. 76 The subanalysis of these studies found that glucagon may not be effective if insulin is on board or if it is delivered incorrectly because of CGM error. 76 Weinzimer et al. 77 used pramlintide in CL. The use of pramlintide in CL was associated with overall delayed time to peak blood glucose level (2.5±0.9 vs.1.5±0.5 h; P<0.0001) and reduced magnitude of glycemic excursion (88±42 vs. 113±32 mg/dL; P=0.006) compared with CL without pramlintide.
Recently, two randomized crossover studies were carried out to establish the safety and efficacy of an automated bihormonal CL system (bionic pancreas) in an unrestricted outpatient condition. 78 The study included 20 adults and 32 adolescents with T1DM. In adults, after 1 day of automatic adaptation by the bionic pancreas, the mean CGM glucose level (133±13 vs. 159±30 mg/dL; P<0.001) and the percentage of time with a hypoglycemia episode (4.1% vs.7.3%; P=0.01) were lower in bionic pancreas periods compared with control periods. Among the adolescents, the mean plasma glucose level was also lower during the bionic pancreas period than during the control period (138±18 vs. 157±27 mg/dL; P=0.004), but the percentage of time with a low plasma glucose reading was similar during the two periods. 78 This is the largest study so far demonstrating the effectiveness of a bihormonal CL system in controlling the blood glucose level within a narrow range with minimal hypoglycemia. The studies with bihormonal CL are summarized in Table 1.
The Limitations of the CL System
Limitations of the CL may be related to all the components of the system and are as follows: 1. The most common problem encountered by patients with diabetes using CSII is infusion set failure.
79
In theory, patients using CSII are at a higher risk of diabetic ketoacidosis because of the use of rapid-acting insulin analogs and unrecognized kinking or blockage and infection at the infusion site of the catheter.
24,80
However, real-life studies have shown that the incidence of diabetic ketoacidosis is lower with CSII than with MDI.
80,81
Patient education on infusion site care, pump troubleshooting, and insulin dose adjustments for exercise and sickness are important in reducing hypoglycemia and diabetic ketoacidosis.
35,82
2. The bolus calculators used in CSII use the insulin:carbohydrate ratio and other factors for insulin dose calculation. Studies have shown that taking fat and protein into account for insulin dose results in significant A1C reduction compared with only carbohydrate counting.
83
Thus, future algorithms may need to incorporate complete meal constituents for better glycemic outcomes with CL. 3. Another obstacle in closing the loop is the accuracy of the CGMs. Although the current generations of commercially available CGMs have improved significantly, there is still room for improving the accuracy.
84
The current-generation CGMs are invasive, and therefore approximately 5–20% of patients experience erythema, edema, or skin irritation from the sensor adhesive.
35
One of the disadvantages of CGM is the 5–15-min lag time between blood and interstitial glucose values,
85,86
which may be higher if the rate of change of glucose level is higher (>3 mg/min). Additionally, the enzyme-based CGM devices have a variety of drug interactions, such as acetaminophen, ascorbic acid, and dopamine, depending on the enzyme (glucose oxidase or glucose-1-hydrogenase) used in the sensor.
87
Further inaccuracies can result from changes in blood pH, hematocrit, blood oxygenation, and the environmental temperature.
87,88
Sensor attenuation over time may be difficult to detect: Castle and Ward
88
suggested the use of multiple sensors, which can reduce this problem. In addition, the currently available CGMs need frequent calibration from the BGM. Therefore, any BGM limitations or errors make CGM data less accurate. The BGM readings are influenced by many other factors, such as site, contamination of the site with sugar, and temperature and humidity of test strips, and thus influence the accuracy of the CGM.
35
4. There are several limitations with the algorithms used to modulate insulin administration in a CL (e.g., adjustment for exercise and/or food consumption).
89
The algorithms do not predict when a patient eats meals, and this results in postprandial spikes in blood glucose levels due to a lag in onset of insulin's action.
89
Until this limitation is overcome, the CL will likely be hybrid systems where users announce the meal or exercise, and necessary actions for premeal bolus or adjusting insulin delivery, respectively, are taken. 5. Lastly, the lack of availability of ultra-rapid (faster-acting) insulin analogs makes it harder to imitate normal human physiology where the onset of action of insulin is immediate. Even with a rapid-acting insulin analog, peak action does not occur until about 90 min after subcutaneous delivery, in addition to the inter- and intra-individual variability.
90
The limitations of the current CL and its possible solution to make a fully automated artificial pancreas possible are summarized in Table 2.
An up arrow (↑) indicates an increase; a down arrow (↓) indicates a decrease.
CGM, continuous glucose monitor; DKA, diabetic ketoacidosis; PID, proportional-integral-derivative model; SMBG, self-monitoring blood glucose; YSI, Yellow Spring Instrument blood glucose analyzer.
Future Directions in the CL System
Most of the currently available insulin pumps deliver insulin through a tube that may kink or detach. To avoid these tube/catheter-related complications, there has been growing interest in the development of patch pumps. Several patch pumps are currently available or are under development, including the OmniPod, the Solo™ MicroPump (Medingo US, Inc., Tampa, FL), the Finesse™ (Calibra Medical Inc., Redwood City, CA), the Cellnovo pump (Cellnovo Ltd., London, United Kingdom), the Freehand™ system (MedSolve Technologies, Inc., Manhattan Beach, CA), the Nanopump™ (Debiotech SA, Lausanne, Switzerland), the NiliPatch disposable insulin pump system (NiliMEDIX Ltd., Tirat-Carmel, Israel), the PassPort® system (Altea Therapeutics Corp., Atlanta, GA), the V-Go™ (Valeritas, Inc., Bridgewater, NJ), and the CeQur™ (Montreux, Switzerland) device. 91
Incorporating sensors with the infusion set is also under investigation, which may make CL more patient-friendly. 92 Many companies are investigating the incorporated sensor with infusion sets such as the Pod-Talk (Insulet Corp.) and the Medtronic integrated sensor and set. 93 A specifically designed hydrogel (zinc oxide poly[N-isopropylacrylamide–acrylamide–2-aminomethyl-5-fluorophenylboronic acid]) has been shown to measure glucose levels with high sensitivity and selectivity while simultaneously regulating insulin release in response to glucose values, which may be helpful in making a miniaturized CL. 94 Future studies on overnight CL and predictive low glucose management systems are ongoing.
The currently available CGMs are invasive and thus result in an inflammatory response at the insertion site and biofouling, which may result in inaccurate CGM data. Additional research is occurring to reduce this biofouling by use of special membrane or sensor materials that limit inflammation or using a sensor membrane coated with anti-inflammatory drugs to reduce inflammation at the site of sensor insertion. 95 Also, the invasiveness of the sensors results in skin-related adverse events, and hence research is continuing for a noninvasive CGM using different techniques such as iontophoresis, bioimpedance spectroscopy, near-infrared spectroscopy, reverse iontophoresis, and sonophoresis. 96 Another problem with the current CGMs is that the sensors last up to 7 days. The recently developed Abbott-FLASH by Abbott Diabetes Care can be used for 14 days and does not need external calibration, but the patient needs to bring the receiver to the transmitter for receiving glucose data. 97 This device is approved only in Europe.
To improve postprandial glucose control, development of ultra-rapid-acting insulins is important. These insulins are expected to overcome the limitation of rapid-acting insulin analogs. 80 There are many ongoing studies to improve the absorption of insulin, namely, fast-acting insulin aspart (FIAsp), VIAject™ insulin (Biodel, Danbury, CT), Hylenex® recombinant (rHuPH20; Halozyme Therapeutics, San Diego), local heating at the site of insulin delivery, and intradermal insulin delivery. 98,99
The main problem in making a dual-hormonal CL is unstable glucagon after reconstitution. 100 Available glucagon is effective for 8 h only, whereas the pump cannula lasts for 3 days. Glucagon analogs or novel preparations of glucagon without stability issues are under development. 101,102 In addition, glucagon administration is limited by nausea and possibly the depletion of hepatic glycogen and cognitive decline during long-term use. 103
Conclusions
The first step in closing the loop is suspending the insulin administration as hypoglycemia is detected. The TS pump has been shown to reduce the severity and duration of hypoglycemia while maintaining A1C values. Further steps such as control-to-range and control-to-target will make a near-perfect artificial pancreas in the future. The limitations of the CL are the infusion set, cannula, BGM, CGM, algorithms, and insulin analogs. Although fully automated CL is still a few years away, the data are promising, and numbers of studies are underway in making the artificial pancreas successful.
Footnotes
Author Disclosure Statement
No competing financial interests exist.