
Abstract
Aim:
This study assessed whether Helicobacter pylori infection could influence metformin tolerance in patients with type 2 diabetes mellitus.
Subjects and Methods:
Demographic, anthropometric, ultrasound, and laboratory data were obtained from 415 metformin-naive patients with diabetes. H. pylori infection was assessed based on the 13C-labeled urea breath test (13C-UBT). The study duration was 4 weeks, and all subjects started metformin from 500 mg/day to 1,500 mg/day progressively. Gastrointestinal side effects were assessed each week, and the metformin doses were adjusted by the compliance. Gastrointestinal side effects were compared between H. pylori–positive and –negative groups.
Results:
According to the 13C-UBT results, 220 patients were categorized as H. pylori negative versus 195 as H. pylori positive. At baseline, the scoring of gastrointestinal symptoms showed no statistical difference between the two groups. After 4 weeks, for gastrointestinal symptoms such as abdominal pain, nausea, bloating, and anorexia, the respective percentages in H. pylori–positive and –negative subjects were 44.6% versus 21.8% (P<0.01), 20.0% versus 9.6% (P<0.01), 47.7% versus 23.2% (P<0.01), and 32.8% versus 12.3% (P<0.01). The final metformin dose was 951.28±661.1 mg in H. pylori–positive subjects, significantly less than that in H. pylori–negative subjects (1,209.09±522.91 mg) (P<0.01). On multivariate analysis, female gender, H. pylori infection, body mass index, triglycerides, age, and low-density lipoprotein-cholesterol were the independent parameters associated with any gastrointestinal symptoms.
Conclusions:
Patients with diabetes having H. pylori infection demonstrated more gastrointestinal side effects than those without H. pylori infection after taking metformin. Furthermore, female gender, H. pylori infection, body mass index, triglycerides, age, and low-density lipoprotein-cholesterol are independent determinants of metformin's side effects.
Introduction
T
Currently, metformin is recommended as a first-line antihyperglycemic agent by most of the T2DM management guidelines from different countries. 3,4 It does not stimulate insulin secretion and therefore does not cause hypoglycemia. The United Kingdom Prospective Diabetes Study had provided evidence of beneficial effects, including cardiovascular protection and safety of metformin, in the treatment of T2DM. 5 Furthermore, a cost-effectiveness analysis by the United Kingdom Prospective Diabetes Study Group declared that metformin was both cost-saving and extends life expectancy when used as first-line pharmacological therapy in overweight patients with T2DM. 6 So if not contraindicated and if well tolerated, metformin is the preferred initial pharmacological agent for T2DM. 3
On the other hand, digestive disorders (such as abdominal pain, diarrhea, vomiting, and, very rarely, lactic acidosis) represent the most common side effects of metformin for T2DM. 7 Although metformin is recommended as a first-line drug in elderly T2DM patients, 8 there is an increasing safety concern that the elderly may be more vulnerable to gastrointestinal side effects. Thus the maximal dosage allowed for clinical use in many Chinese hospitals is 1,500 mg/day, especially in the elderly.
In 2012, a prospective cohort study demonstrated that Helicobacter pylori infection is associated with an increased rate of incident diabetes. 9 Another retrospective study suggested a trend toward more frequent H. pylori infections in patients with diabetes, especially in patients with T2DM. 10 As has been well documented, H. pylori infection can cause gastrointestinal complications in the normal population and patients with T2DM. 11 It seems to be intriguing to explore potential associations between metformin and H. pylori infection because both exhibit similar gastrointestinal complications. Currently, to the best of our knowledge, there has been no systematic study to address this issue. Thus, we felt imperative to conduct this study, which enrolled metformin-naive T2DM patients and assessed whether there is an association between H. pylori infection and metformin tolerance.
Subjects and Methods
All patients were recruited from Huadong Hospital, Shanghai, Fudan University School of Medicine, Shanghai, People's Republic of China. There were, in total, 419 T2DM subjects enrolled in the study according to the protocol. The study protocol was approved by the Ethics Committee of Huadong Hospital (ethics protocol number [2012]056). Written informed consent was obtained from all participants before the study.
Inclusion criteria
All patients were diagnosed with T2DM according to the 2012 American Diabetes Association criteria. 12 All patients were over 40 years old. The patient could have used no drugs or any other antihyperglycemic drugs except metformin, α-glucosidase inhibitors, or glucagon-like peptide-1 receptor agonists.
Exclusion criteria
The exclusion criteria included the following: (1) a history of known peptic ulcer, H. pylori infection, or gastrointestinal discomfort (including motility disorders and small intestinal bacterial overgrowth); (2) currently (in the 4 weeks prior to initiation of the study) using aspirins, proton pump inhibitors, or antibiotics; (3) currently with diabetic ketoacidosis or hyperosmolar coma; (4) currently with cardiovascular disease or other serious disease; (5) currently with hypoglycemia; (6) creatinine clearance rate of <45 mL/min 8 ; (7) impaired liver function (liver enzymes more than twice the upper limit of normal); (8) receiving unknown combination drugs; or (9) poor drug compliance.
Protocol
This was a 4-week, double-blind study.
Following a 10-h overnight fast, anthropometric, serum, plasma, and urine samples were collected. A questionnaire was used to collect information on medical history, including initial date of diagnosis of diabetes, use of medications and tobacco, history of organ disease, and family history. Biochemical measurements of plasma glucose, serum lipids, liver enzymes, high-sensitivity C-reactive protein, glycosylated hemoglobin (HbA1c), and urine albumin were performed in a central laboratory, and the urine albumin:creatinine ratio was calculated. Fat liver and gallstones were measured by B-mode ultrasound by the same researcher. H. pylori infection was identified by the 13C-labeled urea breath test (13C-UBT). 13 To maintain blinding, the results of 13C-UBT and blood samples were not released to both researchers and patients during the protocol.
All patients were instructed to maintain their recommended dietary, medication, and exercise programs. Metformin (Glucophage™; Bristol-Myers Squibb, Princeton, NJ) was supplied as 500-mg tablets. All patients received 500 mg of metformin with breakfast for the first week. Metformin was increased to one tablet with breakfast and one with dinner for the second week. Then it was increased to one tablet with breakfast, one with lunch, and one with dinner for the third week. Considering the potential serious side effects in elderly patients, the final daily metformin dosages were 1,500 mg. Compliance was assessed by tablet count at each visit.
Patients were scheduled for clinic visits once a week. Adverse events and concomitant medications were assessed at each visit. All the patients were questioned weekly by a same research nurse for gastrointestinal symptoms. The questionnaire covered the following six digestive disturbances: (1) abdominal pain; (2) diarrhea; (3) nausea; (4) vomiting; (5) bloating; and (6) anorexia. A scoring system of 0–4 was used to grade the severity of the symptoms, 14 where 4=severe (gastrointestinal problem inducing ill health such as malnutrition, hospitalization), 3=significant (gastrointestinal symptoms present to the extent that daily activity is disturbed), 2=moderate (gastrointestinal symptom present with some disturbance to daily activity), 1=mild (daily activity not affected), and 0=no symptoms. If a patient had a symptom with a score above 1, the dose of metformin could be considered not to increase for the next week. If a patient had a symptom with more than a score of 2 or found it hard to tolerate the side effects, the patient should be considered to end the study by researchers.
Statistical analyses
Statistical analyses were performed with SPSS version 13.0 software (SPSS Inc., Chicago, IL). Baseline characteristics were expressed as mean±SD values or number (percentage). HbA1c measurements are reported in International Federation of Clinical Chemistry and Laboratory Medicine units (mmol/mol), followed by derived National Glycohemoglobin Standardization Program units (%). 15 A logarithmic transformation because of skewed distribution was performed as needed. The t test and χ2 test were used for between-group comparisons where appropriate, after adjustment for age and gender. The Pearson correlation coefficient (r) and t test were conducted to evaluate the relationship between gastrointestinal symptoms and anthropometric indices and metabolic variables where appropriate. The generalized linear model was used to examine the independent relationship between scoring of any gastrointestinal symptoms and the following variables: age, gender, body mass index (BMI), blood pressure, HbA1c, duration of diagnosed diabetes, H. pylori infection, lipid profile, liver enzymes, fat liver, gallstone, high-sensitivity C-reactive protein, and albumin:creatinine ratio. A P value of <0.05 was considered statistically significant.
Results
There were, in total, 419 subjects with T2DM enrolled in the study. One patient failed to complete the 13C-UBT, three patients lost contact during the protocol, and the rest (n=415) completed the whole study.
The clinical characteristics of the 415 patients under the baseline are summarized in Table 1. According to the 13C-UBT, 220 patients were H. pylori–negative, and 195 were H. pylori–positive. Gender, BMI, duration of diabetes, blood pressure, fasting glucose, HbA1c, liver enzymes, B-mode ultrasound, and lipid profile showed no statistical difference between the two groups. H. pylori–positive patients had a higher albumin:creatinine ratio level and a lower age than –negative subjects (P<0.05). At baseline, the scoring of gastrointestinal symptoms showed no statistical difference between the two groups (Table 2). No one presented a score above 1 or complained of vomiting at baseline.
Data are mean±SD values or number (percentage), as indicated.
P<0.05, significant difference for H. pylori positive versus negative.
ACR, urine albumin:creatinine ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BP, blood pressure; F, female; GGT, γ-glutamyl transferase; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; M, male.
Data are number (percentage).
NS, not significant.
After 4 weeks, both groups showed a better glucose control by measuring fasting glucose, but the difference between the two groups was not significant (Table 3). Of the 195 H. pylori–positive subjects, in total, 122 (62.6%) had digestive disturbances (irrespective of severity) compared with 80 (40.0%) of the 220 control subjects (P<0.01). For gastrointestinal symptoms such as abdominal pain, nausea, bloating, and anorexia, the respective percentages in H. pylori–positive and –negative subjects were 44.6% versus 21.8% (P<0.01), 20.0% versus 9.6% (P<0.01), 47.7% versus 23.2% (P<0.01), and 32.8% versus 12.3% (P<0.01). When focused on the scoring of digestive symptoms, we found similar results: abdominal pain, 0.6±0.74 versus 0.3±0.61 (P<0.01); nausea, 0.24±0.52 versus 0.13±0.42 (P<0.05); bloating, 0.54±0.62 versus 0.26±0.51 (P<0.01); and anorexia, 0.39±0.61 versus 0.14±0.38 (P<0.01). All differences remained statistically significant after adjusting for age and sex status. However, compared with the H. pylori–negative subjects, H. pylori–positive subjects presented similar rates of vomiting and diarrhea (Table 3).
Data for percentages are number (percentage). Data for gastrointestinal scoring, fasting glucose, and metformin dose are mean±SD values.
P<0.05, b P<0.01 for H. pylori–positive versus –negative.
Table 3 also shows the number of subjects who failed to complete the study. Of the 195 H. pylori–positive subjects, in total, 57 (29.2%) failed to complete the study (54 were digestive disturbances related) compared with 28 (12.7%; all of them were digestive disturbances related) of the 220 control subjects (P<0.01). Actually, all gastrointestinal symptoms were either mild (score=1) or moderate (score=2) in severity. No subject in either group had a score of more than 2. However, several patients refused to increase the dose of metformin or to continue to take metformin even if the digestive disturbances were mild. For Good Clinical Practice and security reasons, we respected patients' decision. The final metformin dose was 951.28±661.1 mg in H. pylori–positive subjects, significantly less than that in H. pylori–negative subjects (1,209.09±522.91 mg) (P<0.01).
Figure 1 shows that elderly patients were treated with lower doses of metformin compared with younger patients, regardless of H. pylori infection. However, in the subgroup 40–49 years of age, H. pylori–positive and –negative patients have similar metformin tolerance. Figure 2 also shows similar gastrointestinal symptoms between H. pylori–positive and –negative patients in the subgroup 40–49 years of age.
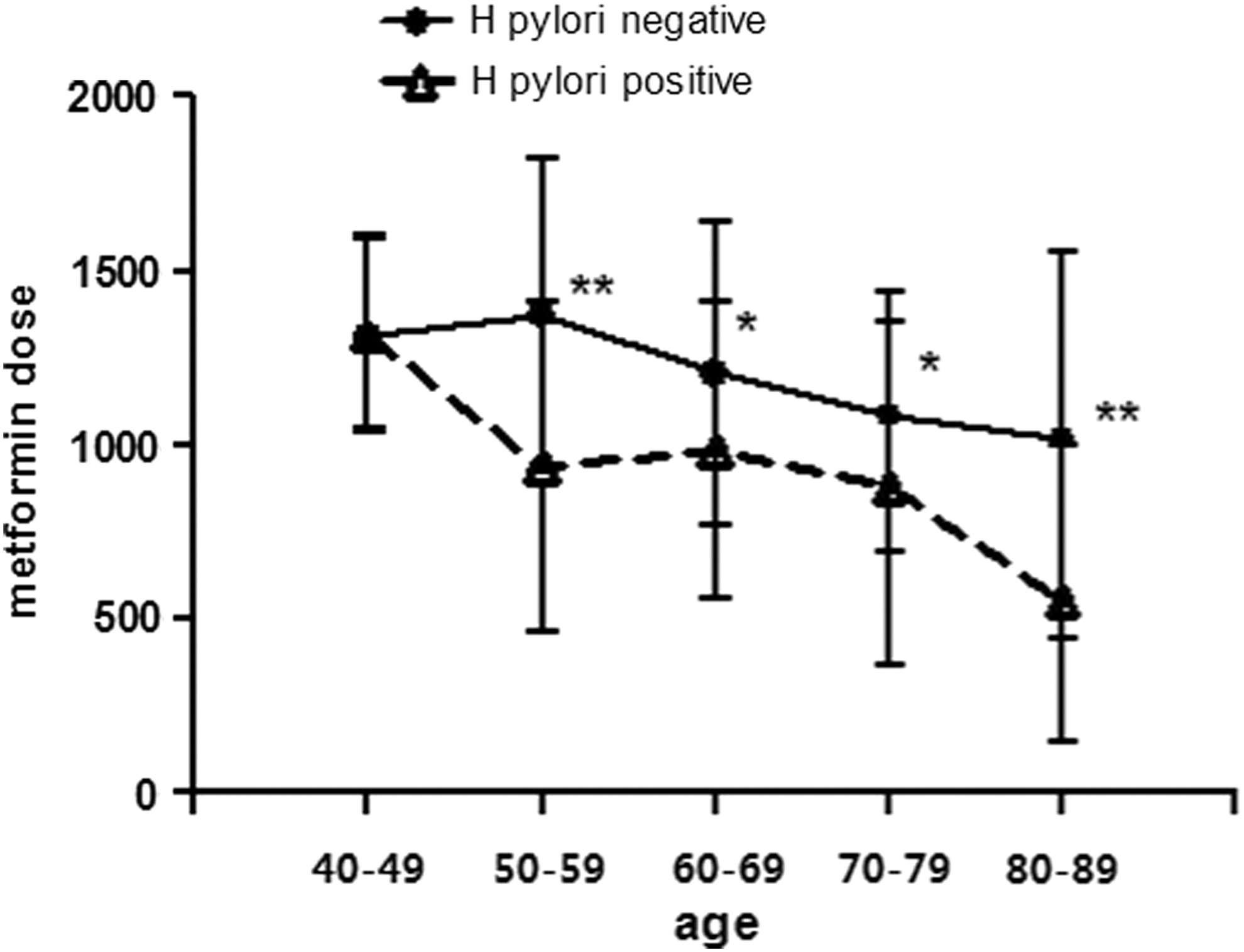
Distributions of the different age brackets associated with metformin dose. Data are mean±SD values. *P<0.05, **P<0.01 for H. pylori–positive versus –negative.
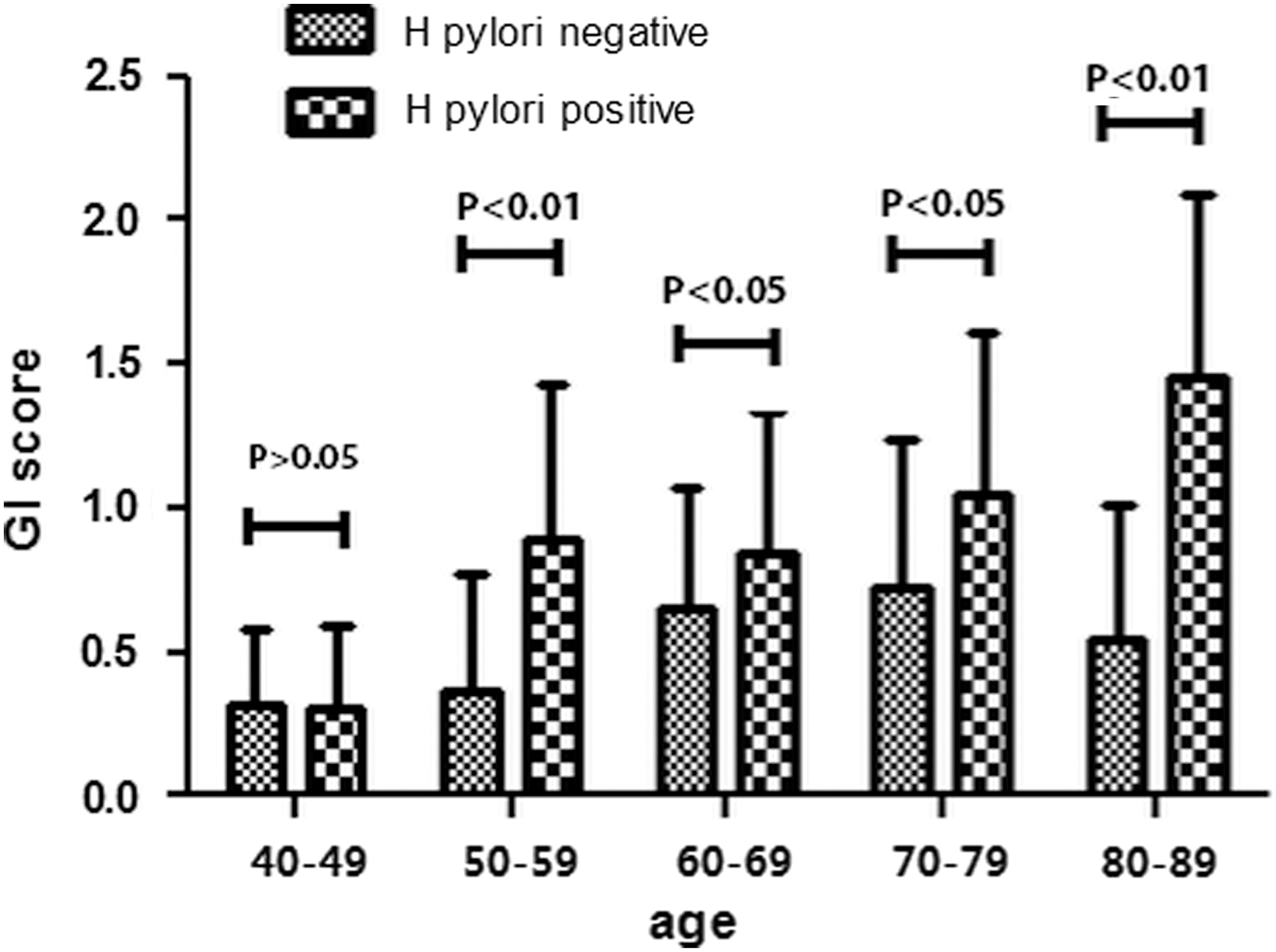
Distributions of the different age brackets associated with gastrointestinal (GI) score. Data are mean±SD values.
Bivariate correlation analyses showed that age (r=0.20668, P<0.01), duration of diabetes (r=0.13430, P<0.01), BMI (r=–0.15532, P<0.01), HbA1c (r=–0.11843, P<0.05), γ-glutamyl transferase (r=–0.10796, P<0.05), and total triglycerides (r=–0.15450, P<0.01) were significantly correlated with scoring of any gastrointestinal symptoms. The t test showed that female gender (t value=2.54, P<0.05), fat liver (t value=2.93, P<0.01), gallstones (t value=1.98, P<0.05), and H. pylori infection (t value=4.42, P<0.01) were correlated with scoring of any gastrointestinal symptoms.
On multivariate analyses (using gender, age, BMI, duration, systolic blood pressure, diastolic blood pressure, fasting glucose, HbA1c, alanine aminotransferase, aspartate aminotransferase, γ-glutamyl transferase, triglyceride, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, high-sensitivity C-reactive protein, albumin:creatinine ratio, fat liver, gallstones, and H. pylori as independent variables), female gender (β=0.20160, P=0.0069), H. pylori infection (β=0.379, P=0.0001), BMI (β=–0.02276, P=0.0205), triglycerides (β=–0.06858, P=0.0125), age (β=0.01187, P=0.0002), and low-density lipoprotein cholesterol (β=–0.09721, P=0.0271) were independent parameters associated with the total score of any gastrointestinal symptoms (Table 4).
The generalized linear model was used to examine the independent determinants of scoring for any gastrointestinal symptoms. The full model contained gender, age, body mass index (BMI), duration, systolic blood pressure, diastolic blood pressure, fasting glucose, glycosylated hemoglobin, alanine aminotransferase, aspartate aminotransferase, γ-glutamyl transferase, triglycerides, total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol (LDL-C), high-sensitivity C-reactive protein, albumin:creatinine ratio, fat liver, gallstones, and H. pylori. Variables were entered in the model if the significance of the F value was <0.05 and removed if it was >0.10.
Discussion
In this study, we compared gastrointestinal intolerance of metformin between H. pylori–infected patients and H. pylori–negative ones in patients with T2DM for the first time. We found significantly worsened gastrointestinal side effect (such as abdominal pain, nausea, bloating, and anorexia) in patients with H. pylori infection after taking metformin than in H. pylori–negative patients. We further confirmed that female gender, H. pylori infection, BMI, triglycerides, age, and low-density lipoprotein cholesterol are independent determinants of gastrointestinal symptoms while taking metformin.
As has been well documented before, the most common side effects that limit metformin dosage were gastrointestinal symptoms, particularly abdominal pain, nausea, bloating, and diarrhea. In previous studies, patients using metformin suffered significantly more gastrointestinal side effects than those using placebo. 16 But, the adverse effects were generally tolerable and self-limiting. In a population with previous use of oral antidiabetes drugs or insulin, patients using metformin also suffered more gastrointestinal side effects than those using placebo. 17,18 In our study, most of the patients suffered from metformin's side effects whether or not they exhibited H. pylori infection (Table 3).
In 1997, a study demonstrated that metformin's therapeutic benefit was dose dependent. Benefits were observed with as little as 500 mg of metformin; maximal benefits were observed at the 2,000-mg and 2,500-mg daily dosage. 17 Generally speaking, gastrointestinal side effects of metformin occurred in the early term of treatment, commonly in less than 10 weeks. 19,20 According to the dose–response study of 451 patients, all dose of metformin were well tolerated, and patients exhibited similar gastrointestinal symptoms from the 1,000 mg to 2,500 mg daily dosage. 17 Therefore, a small initial dose and increasing the dose slowly can minimize gastrointestinal symptoms of metformin. 21
According to the general understanding and clinical experience, the elderly seem to be more vulnerable to gastrointestinal side effects while using metformin. However, in another study of T2DM in Japanese patients, no significant difference was observed in the frequencies of self-reported symptoms between the elderly and nonelderly patients; furthermore, no significant difference was observed in elevated lactic acid levels between elderly and nonelderly patients. 22 In our study, most of the subjects were more than 60 years old. Most of the patients tolerated metformin well, and all gastrointestinal symptoms were either mild or moderate in severity. However, in multivariate analysis, we found that age was an independent parameter associated with the score of any gastrointestinal symptoms.
As we all know, H. pylori is a Gram-negative spiral bacterium that colonizes the gastric mucosa in humans. A study in 2011 showed that there was a high prevalence of H. pylori infection (54.5%) in Northern China. Furthermore, diabetes and age played important roles in H. pylori prevalence. 23 H. pylori is the major cause of chronic gastritis, gastric ulcer, and gastric cancer. Besides, infection of adults with H. pylori is associated with gastrointestinal symptoms such as bloating, vomiting, anorexia, nonulcer dyspepsia, and flatulence. 24 In our study, we also saw a high prevalence of H. pylori infection (46.9%) in patients with T2DM, and we found a significantly increased rate of gastrointestinal side effects in patients with H. pylori infection while they were taking metformin.
Because of lack of evidence, the reason why H. pylori infection could influence metformin tolerance remains unclear. However, existing evidence and our data warrant discussion as a part of the initial effort to address this issue. First of all, H. pylori infection shares similar gastrointestinal side effects with metformin, such as abdominal pain, vomiting, anorexia, and dyspepsia. 17,24 While a patient with H. pylori infection is taking metformin, the gastrointestinal symptoms of metformin and H. pylori infection could overlap and be enhanced. The different gastrointestinal symptom between H. pylori infection and metformin is “diarrhea.” It is interesting that patients with diabetes suffered the same prevalence of diarrhea between the two groups while taking metformin in our study (Table 3). Second, metformin accumulates in the small intestine and stomach after oral administration. 25 H. pylori also colonizes the gastric mucosa in humans. The mucosal damage by H. pylori may enhance the gastrointestinal symptoms by metformin.
Our study also found a positive correlation between female gender and side effects of metformin and a negative correlation between obesity (or hyperlipidemia) and side effects of metformin for the first time. Previous data showed that postmenopausal women exhibited a lower level of sex hormone such as progesterone and estradiol, and administration of progesterone to postmenopausal women contributes to gastric emptying, small bowel transit, and colonic transit. 26 Most female subjects in our study are more than 50 years old. The lack of sex hormone may influence the gastric emptying and enhance the gastrointestinal symptoms by metformin. Another study found that a postprandial increase in plasma glucagon-like peptide-1 and peptide YY was reduced in obese subjects. 27 These outcomes may help to explain why obese patients exhibited fewer side effects after taking metformin.
In any event, our data for the first time, to the best of our knowledge, demonstrated a possible correlation between metformin gastrointestinal side effects and H. pylori infection. However, we should point out that the mechanism of metformin-induced gastrointestinal symptoms is very complicated, and the above-mentioned unaddressed issues call for further translational and clinical studies.
Conclusions
We found that patients with diabetes with H. pylori infection demonstrated more gastrointestinal side effects than those without H. pylori infection while taking metformin. Furthermore, female gender, H. pylori infection, BMI, triglycerides, age, and low-density lipoprotein cholesterol are independent determinants of gastrointestinal symptoms. We therefore speculate that elderly patients with T2DM are more vulnerable to gastrointestinal side effects while using metformin. We shall increase the dosage of metformin more carefully in this population. H. pylori eradication in elderly patients with diabetes may enhance metformin tolerance. H. pylori screening and eradication should be considered in this target population.
Future Research
Future research will be directed to further translational study to dissect the underlying mechanism of how H. pylori is involved in metformin-induced gastrointestinal discomforts. In addition, a similar study with a longer duration (greater than 4 weeks) should be considered. Meanwhile, it would be interesting to see how H. pylori eradication affects symptoms in patients taking metformin. Furthermore, various other antidiabetes medications such as dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists, and α-glucosidase inhibitors will be explored for potential interaction or association with species of gastrointestinal microflora bacteria.
Footnotes
Acknowledgments
We thank Zhao Bin, MD, PhD, and Zhu Xiaolin, MD, PhD, for scientific and editing support to this work.
Author Disclosure Statement
No competing financial interests exist.