
Abstract
Noncommunicable diseases, including type 2 diabetes mellitus and cardiovascular diseases (CVDs), cause 7.9 million deaths every year in South Asia. India has nearly 65.1 million cases of diabetes, and Pakistan and Bangladesh are at the 12th and 13th positions in the global list of high prevalence countries, respectively. The prevalence in India is continuously increasing and is recently reported to be nearly 14% and 8% in urban areas and rural areas, respectively. Diabetes in South Asians is, in some manner, different from that in other races; it occurs nearly a decade earlier, at lower body mass index and waist circumference levels, and with more postprandial hyperglycemia, dyslipidemia, nephropathy, and CVD than in whites. Decision regarding prevention and management of diabetes should be taken in the background of heterogeneity of diet, attitudes, and cultural milieu in South Asia. A need for a low-cost, integrated, yet individualized approach specific for South Asian countries has been increasingly felt since escalating research has uncovered characteristic phenotype, dietary and socioeconomic patterns. Although most such guidelines formulated in developed countries such as the United States or the United Kingdom could be generally applied to developing South Asian countries, there are fundamental differences in applicability of lifestyle and diets (heterogeneous, different from western diets), availability and cost of drugs and insulins, monitoring methods and devices, and insulin pump. Moreover, the monitoring, education, care, and rehabilitation will differ according to different socioeconomic strata and levels of health care (primary, secondary, or tertiary). Some of the potential ethnic-specific modifications have been suggested in this review.
Introduction
T
The prevalence rates of NCDs in the South Asian region differ, but the risk factors are similar. They include rapidly changing and imbalanced nutrition, increasing physical inactivity, and increased stress due to urbanized lifestyle. The phenotype of South Asians contributes significantly to insulin resistance, T2DM, and CVDs. This phenotype includes excess body fat at any given level of body mass index, high prevalence of abdominal obesity, excess intraabdominal and truncal subcutaneous adiposity, and fat deposition at ectopic sites like liver and skeletal muscles. Furthermore, a combination of hypertriglyceridemia and low high-density lipoprotein cholesterol (“atherogenic dyslipidemia”), increased levels of pro-coagulant markers, and subclinical inflammation are also seen in them. 3
Let us discuss T2DM as a case study in the background of this scenario. India occupies the second position in the global list of high prevalence countries, with nearly 65.1 million cases of diabetes, and Pakistan and Bangladesh are in 12th and 13th positions, respectively. 4 The prevalence in India is continuously increasing and has recently been reported to be nearly 14% and 8% in urban and rural areas, respectively. 5 The ICMR-INDIAB study conducted in four centers in India showed the prevalence of T2DM to be as high as 13.6% in Chandigarh and 10.4% in Tamilnadu. 6 Diabetes in South Asians is, in some aspects manner, different from that in whites; it occurs nearly a decade earlier, at lower body mass index and waist circumference levels, and manifests with higher postprandial hyperglycemia, dyslipidemia, nephropathy, and CVD. Such high burden and poor management of diabetes result in an enormous load of early and severe complications and premature mortality. Other specific problems in South Asians include unawareness of diabetes, delay in treatment, intake of ineffective and often harmful alternative medicines, and frequent noncompliance with lifestyle and drugs. 2,7 Low levels of literacy, long travel distance for medical assistance, and inadequately trained human resources further add to suboptimal management. 6,8
Treatment of T2DM is often complex, involves expensive polydrug therapy, and needs to be individualized according to ethnic lifestyle, social, and economic considerations. The approach should be flexible and should take into consideration health-seeking behavior of the population. Decision(s) regarding prevention and management should be modulated according to socioeconomic strata, literacy, dietary preferences, and health-seeking behavior of people residing in different regions of India and those of migrant South Asians. Therefore, there is an undeniable need for a low-cost, integrated, yet individualized approach specific for South Asian countries.
Guidelines are available regarding prevention, diagnosis, and management of diabetes by several organizations and national associations, including the International Diabetes Federation, World Health Organization, American Diabetes Association, Canadian Diabetes Association, and Australian Diabetes Association. In particular, American Diabetes Association guidelines are popular and are revised every year based on research and inputs from a team of experts. These guidelines are published in January each year in the journal Diabetes Care and can be easily accessed by all medical practitioners. 9
Should there be such guidelines for diabetes in South Asians? A need for such guidelines has been increasingly felt in South Asian countries since escalating research has uncovered characteristic phenotype, dietary, and social patterns as stated previously. There are several specific questions that should be addressed while formulating South Asia–specific prevention and management guidelines: • Should we intervene with lifestyle measures at a lower range of body mass index and waist circumference as has been cited in guidelines for Asian Indians
3,10,11
(Table 1)? • Should nutrient-based prevention and management be attempted based on some recently generated evidence
15
? • Is any conventional antihyperglycemic drug more effective in South Asians than in other races
16
? • Are recently introduced antihyperglycemic drugs (dipeptidyl peptidase-IV inhibitors and glucagon-like protein-1 analogs)
16,17
more effective in South Asians?
Data are from Misra and Shrivastava. 3
From consensus guidelines for Asian Indians. 11
According to World Health Organization guidelines. 12
According to both consensus guidelines for Asian Indians 11 and the International Diabetes Federation. 13
According to the Modified National Cholesterol Education Program, Adult Treatment Panel III guidelines. 14
BMI, body mass index.
Although ethnic-specific responses to drug treatment are not conclusive, an important example of an ethnic-specific drug is hydralazine, which shows better response for treatment of hypertension in blacks than in other ethnic groups. 18 Furthermore, a good response to acarbose/voglibose in Japanese patients with T2DM who consume high carbohydrate diets has been clearly recorded, 19 making it a drug of choice after metformin in this ethnic group. This situation may be applicable in Asian Indians who, similar to Japanese, consume high carbohydrate meals. In addition, specifically, in a comparative study between South Asians and whites in the United States, response to pioglitazone was shown to be more in the former: significant improvement in insulin sensitivity (glucose disposal was improved by 32%) and a >50% decrease in levels of high-sensitivity C-reactive protein and plasminogen activator inhibitor-1. 16 Some of these important points are listed in Table 2. Unfortunately, only some of these questions can be answered because of a paucity of research data.
Most of these suggestions have been taken from reviews, consensus guidelines, and research articles. Robust research regarding many suggestions is needed.
BMI, body mass index; HDL, high-density lipoprotein.
Despite overall inadequate research and debate on these important questions, some progress has been made. For example, consensus guidelines for diagnosis of obesity, healthy diets, and physical activity have been formulated for Asian Indians. Consensus obesity guidelines for Asian Indians have included lower cutoffs for overweight (23.0–24.9 kg/m2), obesity (≥25 kg/m2), and waist circumference (≥90 cm for men and ≥80 cm for women) compared with international guidelines (Table 1). 11 Consensus dietary guidelines for India include reduction in the intake of carbohydrates, preferential intake of complex carbohydrates and low-glycemic index foods, higher intake of fiber, lower intake of saturated fats, optimal ratio of essential fatty acids, reduction in consumption of trans fatty acids, slightly higher protein intake, lower intake of salt, and restricted intake of sugar, all taking into consideration the dietary profile and imbalances in Asian Indians in the background of rising obesity and diabetes. 23 It is interesting that recent intervention studies on Asian Indians suggest that specific changes in nutrition quality result in multiple benefits in metabolic, glycemic, and cardiovascular risk profiles, for example, the benefits of pistachio nuts (Fig. 1) in persons with metabolic syndrome 15 and inclusion of high monounsaturated cooking oils in persons with nonalcoholic fatty liver and adverse metabolic features. 30
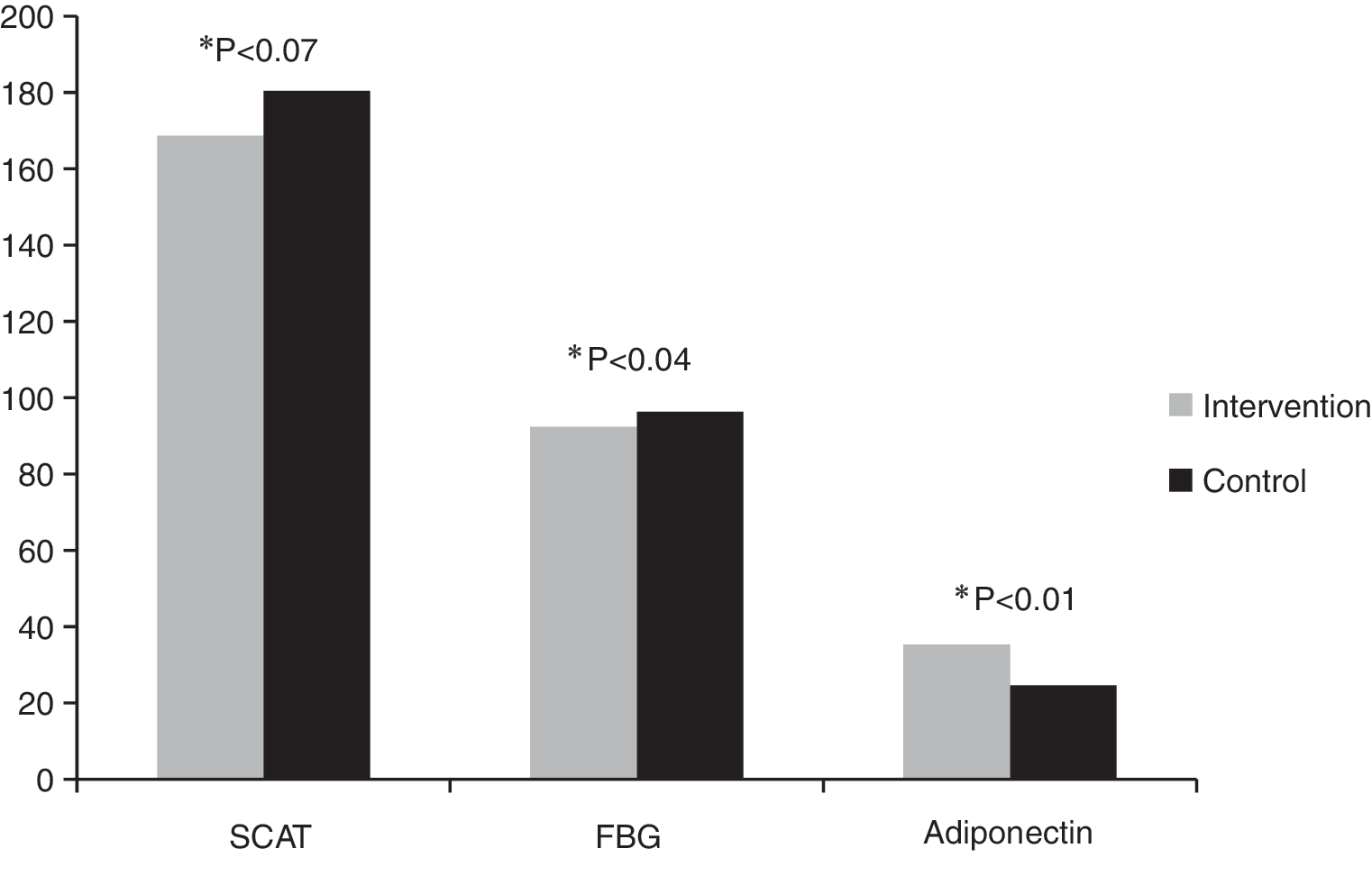
Levels following a 6-month intervention with pistachio nuts (20% of total energy intake) in Asian Indians with metabolic syndrome. Adiponectin levels are in ng/mL. FBG, fasting blood glucose (in mg/dL); SCAT, subcutaneous adipose tissue (in cm3). Adapted from data from Gulati et al. 15
Consensus physical activity guidelines for healthy Asian Indians include a total of 60 min of physical activity (30 min of moderate-intensity aerobic activity, 15 min of work-related activity, and 15 min of muscle-strengthening exercises) daily. Specifically, it also includes resistance training exercises for skeletal muscle, which has shown to be beneficial in Asian Indians with T2DM. 25 It is important that the physical activity instructions are more intensive for Asian Indians than the guidelines for other populations, given their tendency to have low muscle mass, excess adiposity, and a generally metabolically unhealthy profile.
Finally, these already available guidelines could be applied to other South Asian populations because these populations share most phenotypic and metabolic characteristics with Asian Indians. 3 It is interesting that, although many of these other issues are often discussed in various conferences and associations in which South Asian and Middle Eastern countries play prominent parts, no useful discussion on these issues has taken place.
Overall, although some progress has been made in the above areas, no firm guidelines for diagnosis and management of diabetes are yet available for South Asians. For the management of diabetes, the Indian Council of Medical Research released a guideline for Asian Indians in 2005, 31 but they have not been updated since then. Because of a paucity of such specific guidelines, other international guidelines (most popularly that of the American Diabetes Association) have been followed by most physicians in South Asia. Although most such guidelines formulated in developed countries such as the United States or the United Kingdom could be generally applied to developing South Asian countries, there are fundamental differences in applicability of lifestyle and diets (heterogeneous, different from western diets), availability and cost of drugs and insulin, monitoring methods and devices, and insulin pumps. Moreover, the monitoring, education, care, and rehabilitation will differ according to different socioeconomic strata and levels of health care (primary, secondary, or tertiary). In this context, an elaborate document stating all aspects of diabetes in migrant Asian Indians in the United Kingdom is a commendable effort. 32
The lack of proper guidelines for prevention and management of T2DM in Asian Indians is a noticeable gap, which is proving to be a hindrance for prevention and management of diabetes, other NCDs, and their complications. 33 Not only should guidelines be made for each of the NCDs, these should be updated periodically. Finally, meaningful and useful research, specifically, carefully planned intervention studies based on valid hypotheses and scientific questions 33 (and not “me-too” articles), which could alter clinical practice of NCDs, should be part of the national health planning of all South Asian countries.
Footnotes
Acknowledgments
We acknowledge the contribution of Krishnaswami Vijayaraghavan, MD, for contributing to some of the ideas written in this article and for organizing a conference in which many of these issues were deliberated.
Author Disclosure Statement
No competing financial interests exist.