
Abstract
Aim:
Cholesterol absorption has been suggested to be an independent risk factor for cerebral and cardiovascular events. We studied the clinical efficacy of ezetimibe in Japanese patients with type 2 diabetes mellitus complicated by dyslipidemia, in whom increased cholesterol absorption had been reported.
Subjects and Methods:
Ninety-six patients with type 2 diabetes complicated by dyslipidemia received ezetimibe at 10 mg/day for 12 weeks. The lipid profile, a cholesterol synthesis marker (lathosterol), and cholesterol absorption markers (cholestanol, sitosterol, and campesterol) were measured before and after the therapy to evaluate the clinical efficacy of ezetimibe.
Results:
Serum low-density lipoprotein-cholesterol (LDL-C) levels were positively associated with cholesterol absorption markers but not associated with a cholesterol synthesis marker, suggesting that serum LDL-C levels are more strongly related to cholesterol absorption than synthesis. During the 12-week ezetimibe treatment period, cholesterol absorption markers significantly decreased, and serum lipid profiles, including LDL-C levels, significantly improved. The LDL-C-lowering rate was greater in those patients who had been receiving statin therapy and were newly started on ezetimibe additionally than in the ezetimibe monotherapy group (−31.4% vs. −18.4%; P<0.001).
Conclusions:
It is suggested that ezetimibe improves the lipid profile in Japanese type 2 diabetes patients with dyslipidemia through the substantial reduction of cholesterol absorption.
Introduction
M
Unfortunately, increasing the statin dose would not be the best strategy because doubling the statin dose did not greatly improve the LDL-C-lowering rate (“Rule of Six” for statins) but did increase the number of adverse effects. 2,3 Furthermore, many clinical trials, including PROVE-IT, 4 have shown that the extent of the LDL-C-lowering effect decreased as the duration of statin therapy was prolonged. This is called the “statin escape phenomenon”: the cause of the phenomenon may be that statins inhibit cholesterol synthesis in the liver, and the decreased synthesis will cause a compensatory increase in cholesterol absorption in the small intestine. Additionally, several studies, including the DEBATE, LURIC, and PROCAM studies, 5 –9 suggested that “cholesterol absorption” is an independent risk factor for cerebral and cardiovascular events. Retrospective data of the 4S study also showed that, although statins inhibited cholesterol synthesis, the effect was offset by an increased cholesterol absorption and that an increased cholesterol absorption may be associated with a higher incidence rate of cerebral and cardiovascular events. 10
Therefore, inhibiting cholesterol absorption in the small intestine is attracting attention, and the molecular mechanism is being clarified. Altmann et al. 11 found a transporter in cholesterol absorption in the small intestine, Nieman-Pick C1-like 1 (NPC1L1), using the genomic-bioinformatics approach. In recent years, some studies have reported that addition of ezetimibe, an NPC1L1 inhibitor, 12 to statin therapy inhibited the statin escape phenomenon (i.e., a compensatory increase in cholesterol absorption) 13 –17 and provided a higher LDL-C-lowering effect than that provided by only increasing the statin dose. 18,19 Currently, therefore, ezetimibe is used in routine clinical practice as an additional drug for patients in whom therapeutic effect of statin monotherapy was insufficient or as an option for patients in whom statins cannot be used.
It is interesting that in patients with DM, the expression of NPC1L1, which facilitates cholesterol absorption in the small intestine, increases, and the expressions of ABCG5 and ABCG8, which bring cholesterol back to the small intestinal lumen from small intestinal epithelial cells, decrease, which essentially results in increased cholesterol absorption and leads to hyper-LDL-cholesterolemia in this population. 20
The aim of the present study was to investigate the effects of ezetimibe on cholesterol synthesis and absorption as well as the serum lipid profile in Japanese type 2 diabetes patients with hyper-LDL-cholesterolemia.
Subjects and Methods
Study subjects
Screening of the study subjects was performed at the outpatient diabetes clinics of the Osaka Police Hospital (Osaka, Japan). Patients who fulfilled the following criteria were considered eligible as subjects: 1. Diagnosed as having type 2 diabetes based on criteria of the Japan Diabetes Society: • Early morning fasting plasma glucose level of ≥126 mg/dL • 2-h plasma glucose level after 75-g glucose loading of ≥200 mg/dL • Random plasma glucose measurements of ≥200 mg/dL • Hemoglobin A1c (HbA1c) level (NGSP) of >6.5% 2. 20 years of age or older 3. Without familial hypercholesterolemia. Diagnosis of heterozygous familial hypercholesterolemia is based on the presence of hyper-LDL-cholesterolemia (an untreated LDL-C level of ≥180 mg/dL), tendon xanthoma or thantoma tuberosum, and familial history of familial hypercholesterolemia or premature coronary artery disease. Diagnosis of homozygous familial hypercholesterolemia is based on the presence remarkable hypercholesterolemia (an untreated total cholesterol [T-Chol] level of ≥600 mg/dL), xanthoma, and cardiovascular disease from childhood. 4. LDL-C of 120 mg/dL or higher (for patients with ischemic heart disease, LDL-C of 100 mg/dL or higher) 5. HbA1c level of <9% 6. Range of variation in HbA1c level within±1% for the previous 2 months 7. Serum triglycerides (TG) level of <350 mg/dL 8. Treatment regimen had not been changed for at least the previous 4 weeks.
Patients who met the eligibility criteria were randomly selected and asked if they could participate in the present study, and all the patients who agreed to participate were registered. In total, 96 patients were enrolled.
Written informed consent was obtained from all the participants after they had received a full explanation of the study. This study was approved by the ethical committee of the Osaka Police Hospital and was conducted in accordance with the ethical principles set forth in the Helsinki Declaration of 1975 as revised in 1983.
Study design and observation items
This was a prospective, open-label, single-arm study with a 12-week observation period. Ninety-six Japanese type 2 diabetes patients who had been treated for hyper-LDL-cholesterolemia with (Statin group) and without (Nonstatin group) statins newly received ezetimibe at 10 mg/day for 12 weeks. Lipid profiles (T-Chol, LDL-C, high-density lipoprotein-cholesterol [HDL-C], and TG), lathosterol as a cholesterol synthesis marker, and cholestanol, sitosterol, and campesterol as cholesterol absorption markers were measured before and after ezetimibe therapy (at Week 0 and Week 12) to evaluate associations between these metabolic markers and clinical efficacy of ezetimibe. LDL-C levels were calculated using the Friedewald formula (LDL-C=T-Chol – HDL-C – TG/5). The lipid profile markers were measured using a Labospect automatic analyzer (Hitachi, Ltd., Tokyo, Japan). Levels of lathosterol, cholestanol, sitosterol, and campesterol were measured by gas chromatography.
Statistical analysis
Data are reported as mean±SD values, median for continuous variables, or number with percentage in parentheses for categorical variables. For significance tests, baseline clinical and laboratory characteristics within-group comparisons were performed with the paired t test or Wilcoxon signed-rank test. Intergroup comparison was performed with unpaired Student's t test or the Mann–Whitney U test. For all tests, a value of P<0.05 was considered statistically significant. JMP software (SAS Institute, Inc., Cary, NC) was used for statistical analyses.
Results
The baseline characteristics of the study subjects are shown in Table 1. Mean age of the study population was 62.6 years, 63% of whom were male, with a median diabetes duration of 7 years. At baseline, 58 out of 96 study subjects had not been receiving statins (Nonstatin group; the subjects who were newly started on ezetimibe at 10 mg/day), and 38 patients had been receiving statins (Statin group; the patients who had been receiving statins and were newly started on ezetimibe at 10 mg/day additionally). There was no significant difference in any factor of gender, age, body mass index, HbA1c, disease duration, or lipid profile between the two groups. No patients discontinued the study treatment because of adverse effects, such as digestive symptom and laboratory test abnormality, including liver function test and serum creatine phosphokinase levels; all patients completed the 12-week ezetimibe treatment.
Data are mean±SD values or number of subjects (%) as indicated.
BMI, body mass index; CVD, cardiovascular disease; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
First, we evaluated associations between LDL-C and a cholesterol synthesis marker (lathosterol) and cholesterol absorption markers (cholestanol, sitosterol, and campesterol) at baseline. Although there were statistically significant positive associations between LDL-C and cholesterol absorption markers (cholestanol, r=0.431, P<0.001; sitosterol, r=0.381, P<0.001; and campesterol, r=0.329, P=0.001), there was no significant association between LDL-C and lathosterol (r=0.061, P=0.551). Even after the study subjects were divided into the ezetimibe monotherapy (Nonstatin) group and the combination therapy (Statin) group and the same analyses were performed, similar results were observed in both groups: LDL-C levels were significantly associated with cholesterol absorption markers but not with a cholesterol synthesis marker (Fig. 1).
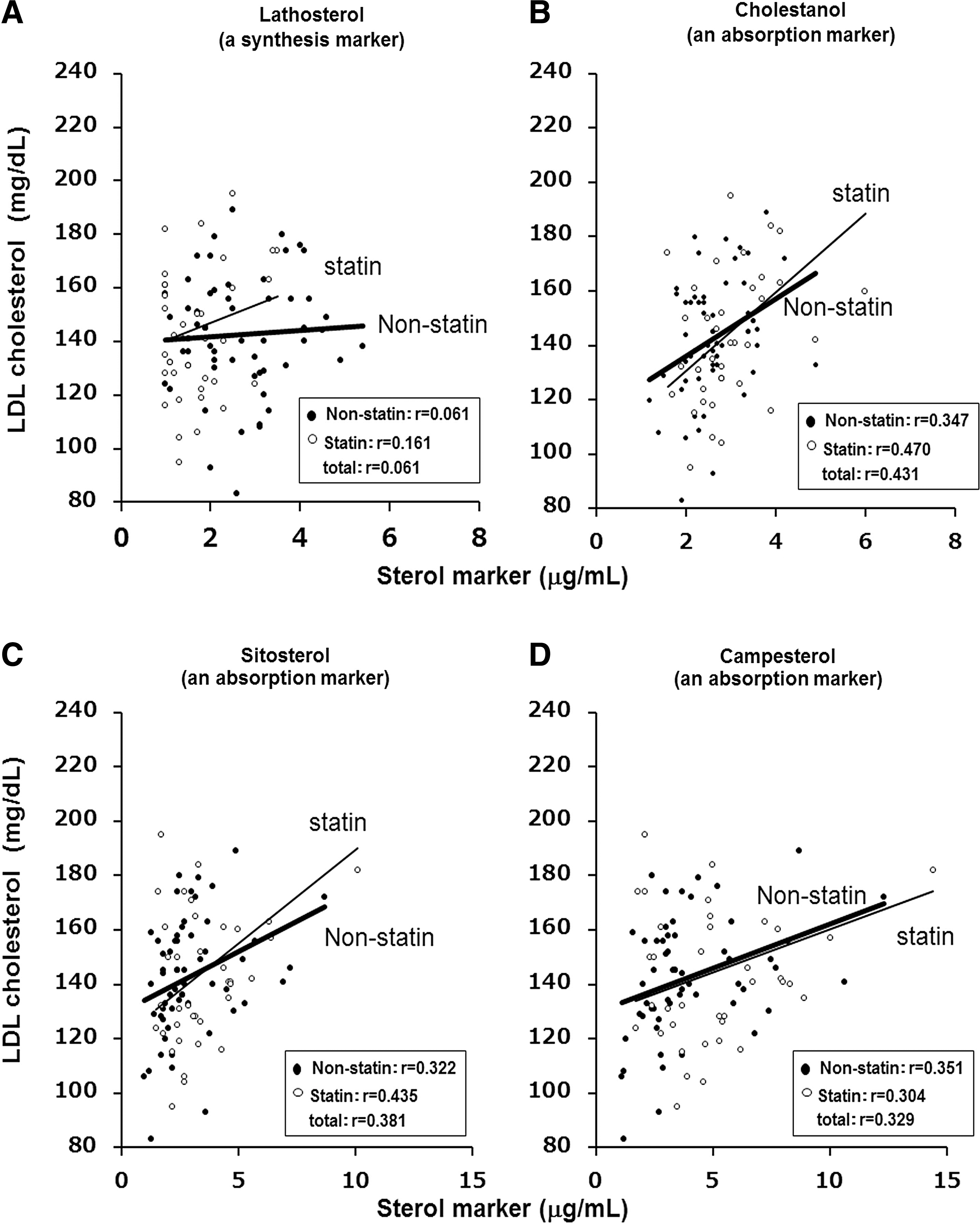
Correlation between low-density lipoprotein (LDL) cholesterol and synthesis/absorption markers at baseline for Japanese type 2 diabetes patients treated with a statin (open dots) or without (nonstatin [black dots]). Although there were statistically significant positive associations between LDL cholesterol and cholesterol absorption markers (
Next, a cholesterol synthesis marker and cholesterol absorption markers at baseline were compared between the Statin group and the Nonstatin group before initiation of ezetimibe therapy. Lathosterol levels were significantly lower (2.6 vs.1.7 μg/mL [P<0.001]), but cholestanol, campesterol, and sitosterol levels were significantly higher (2.6 vs. 3.0 μg/mL [P=0.029], 3.9 vs. 5.2 μg/mL [P=0.015], and 2.9 vs. 3.5 μg/mL [P=0.047], respectively), in the Statin group compared with the Nonstatin group (Fig. 2).
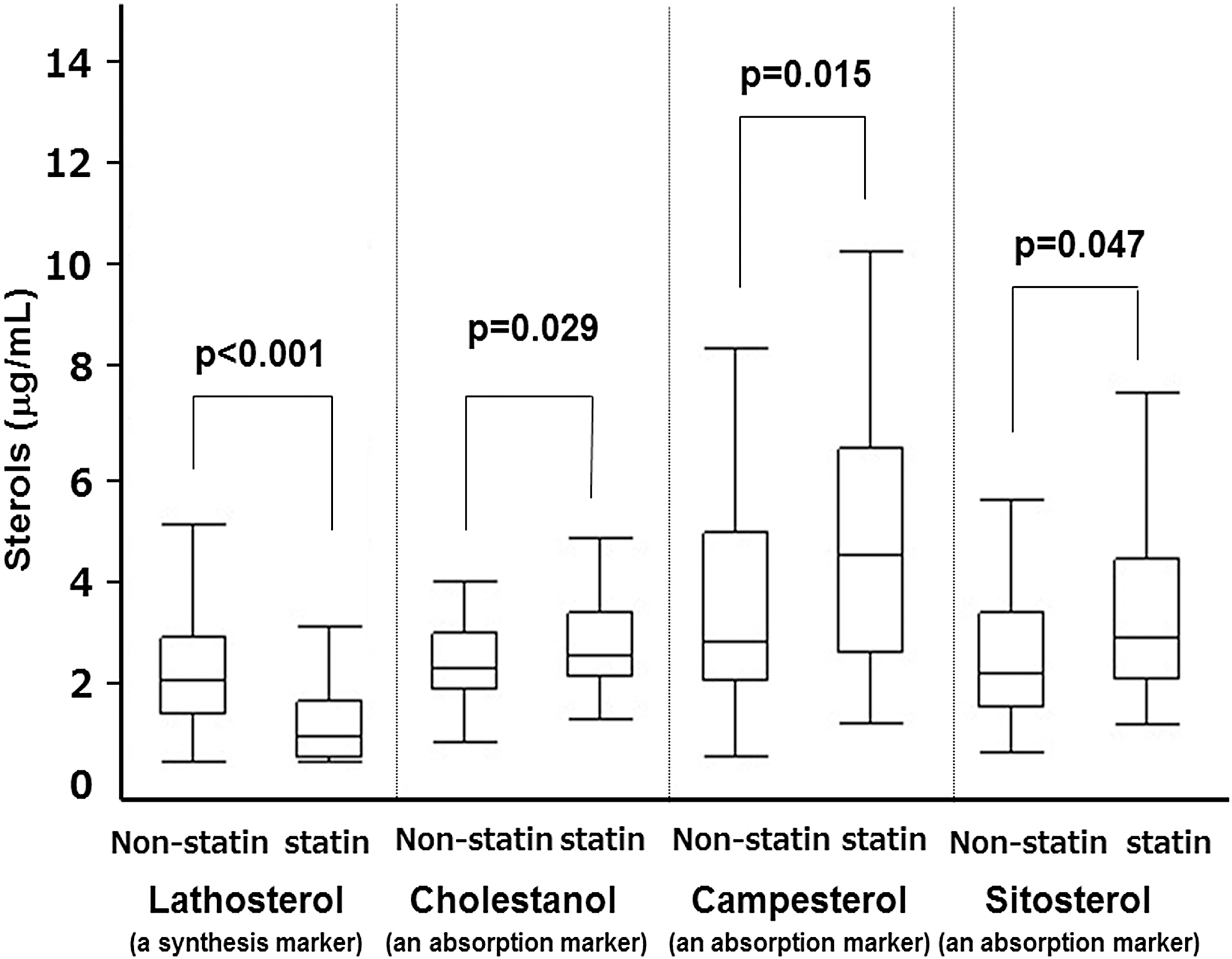
Effect of statin on cholesterol absorption/synthesis (before initiation of ezetimibe treatment). Lathosterol levels were significantly lower (2.6 vs. 1.7 μg/mL [P<0.001]), but cholestanol, campesterol, and sitosterol levels were significantly higher, in the Statin group compared with the Nonstatin group (2.6 vs. 3.0 μg/mL [P=0.029], 3.9 vs. 5.2 μg/mL [P=0.015], and 2.9 vs. 3.5 μg/mL [P=0.047], respectively).
During the 12-week ezetimibe treatment period, most lipid profile serum levels significantly decreased (T-Chol, from 230.4 to 193.0 mg/dL [P<0.001]; LDL-C, from 143.5 to 110.8 mg/dL [P<0.001]; and TG, from 155.9 to 136.4 mg/dL [P=0.015]), whereas HDL-C levels increased (from 50.2 to 50.8 mg/dL [P=0.341]), although without statistical significance (Fig. 3). Even after the subjects were divided into the Nonstatin group and the Statin group and the same analyses were performed, similar results were observed in both groups. It is interesting that the improvement of lipid profile serum levels tended to be greater in the latter group. In particular, the LDL-C-lowering rate was greater in the Statin group than in the Nonstatin group (−31.4% vs. −18.4% [P=0.04]) (Fig. 4), suggesting that improvement effect on lipid profile was greater in the Statin group than in the Nonstatin group.

Changes in lipid parameters during the 12-week ezetimibe therapy. During the 12-week ezetimibe treatment period, most lipid profile serum levels significantly decreased (total cholesterol [T-Chol], from 230.4 to 193.0 mg/dL [P<0.001]; low-density lipoprotein [LDL] cholesterol, from 143.5 to 110.8 mg/dL [P<0.001]; and triglycerides [TG], from 155.9 to 136.4 mg/dL [P=0.015]), whereas high-density lipoprotein (HDL) cholesterol levels increased (from 50.2 to 50.8 mg/dL [P=0.341]), although without statistical significance. Significant differences versus baseline are indicated: *P<0.001, † P=0.015.
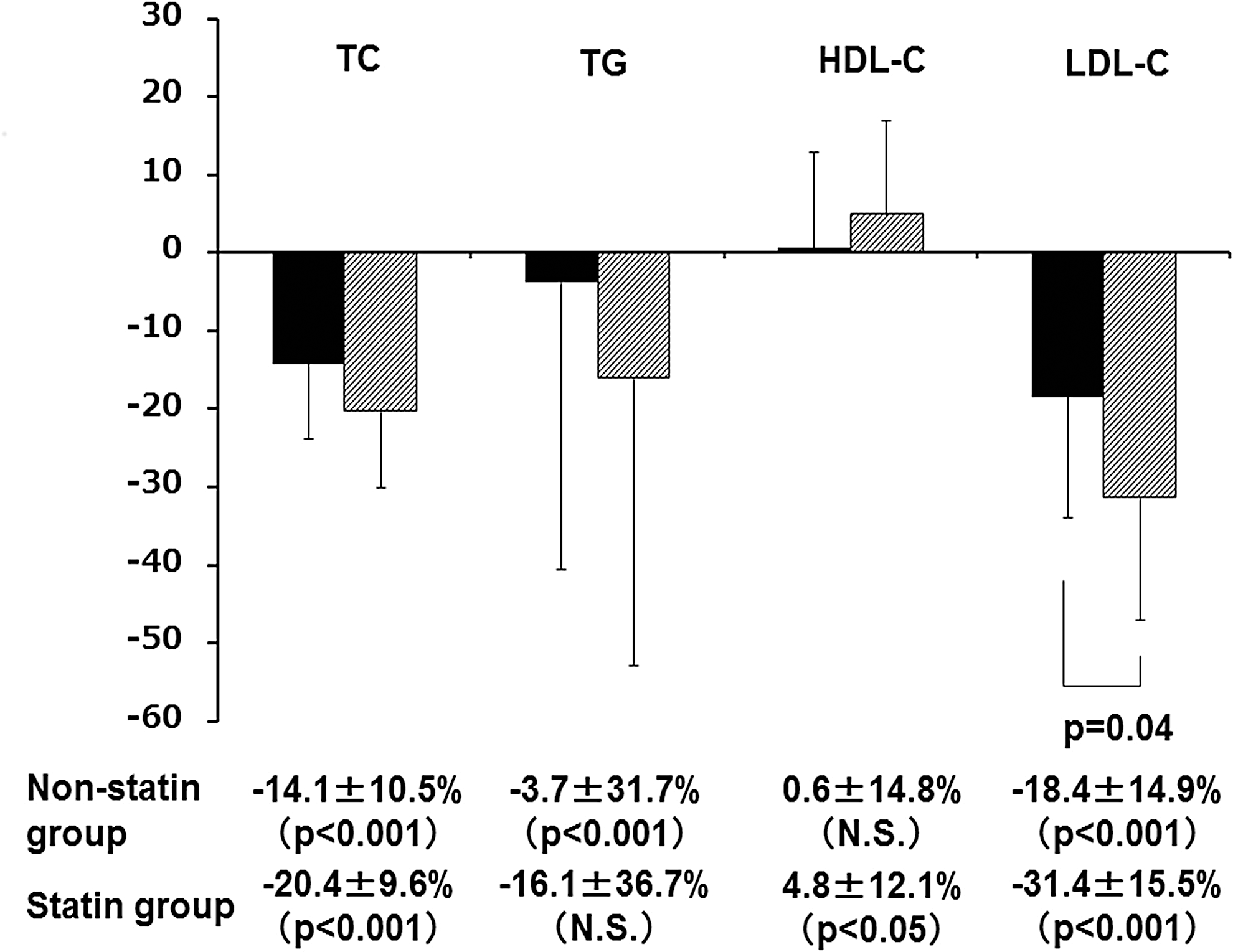
Percentage of change in serum lipids with ezetimibe therapy in the Statin group and the Nonstatin group. The improvement effect of ezetimibe therapy on the lipid profile tended to be greater in the Statin group than in the Nonstatin group. In particular, the low-density lipoprotein-cholesterol (LDL-C)-lowering rate was significantly greater in the Statin group than in the Nonstatin group (−31.4% vs. −18.4% [P=0.04]). HDL-C, high-density lipoprotein-cholesterol; N.S., not significant; TC, total cholesterol; TG, triglycerides.
Finally, the cholesterol synthesis marker (lathosterol) significantly increased (from 2.2±1.1 to 3.4±1.9 μg/mL [P<0.001]) and cholesterol absorption markers (campesterol, cholestanol, and sitosterol) significantly decreased (from 4.4±2.6 to 2.5±1.5 μg/mL [P<0.001], from 2.7±0.8 to 2.3±0.8 μg/mL [P<0.001], and from 3.1±1.7 to 2.0±1.0 μg/mL [P<0.001], respectively) during the 12-week ezetimibe treatment period (Fig. 5). Similar results were observed when the study subjects were divided into Statin and Nonstatin groups and analyses were separately performed (Fig. 6).

Changes in cholesterol absorption/synthesis markers during the 12-week ezetimibe therapy. During the 12-week ezetimibe treatment period,
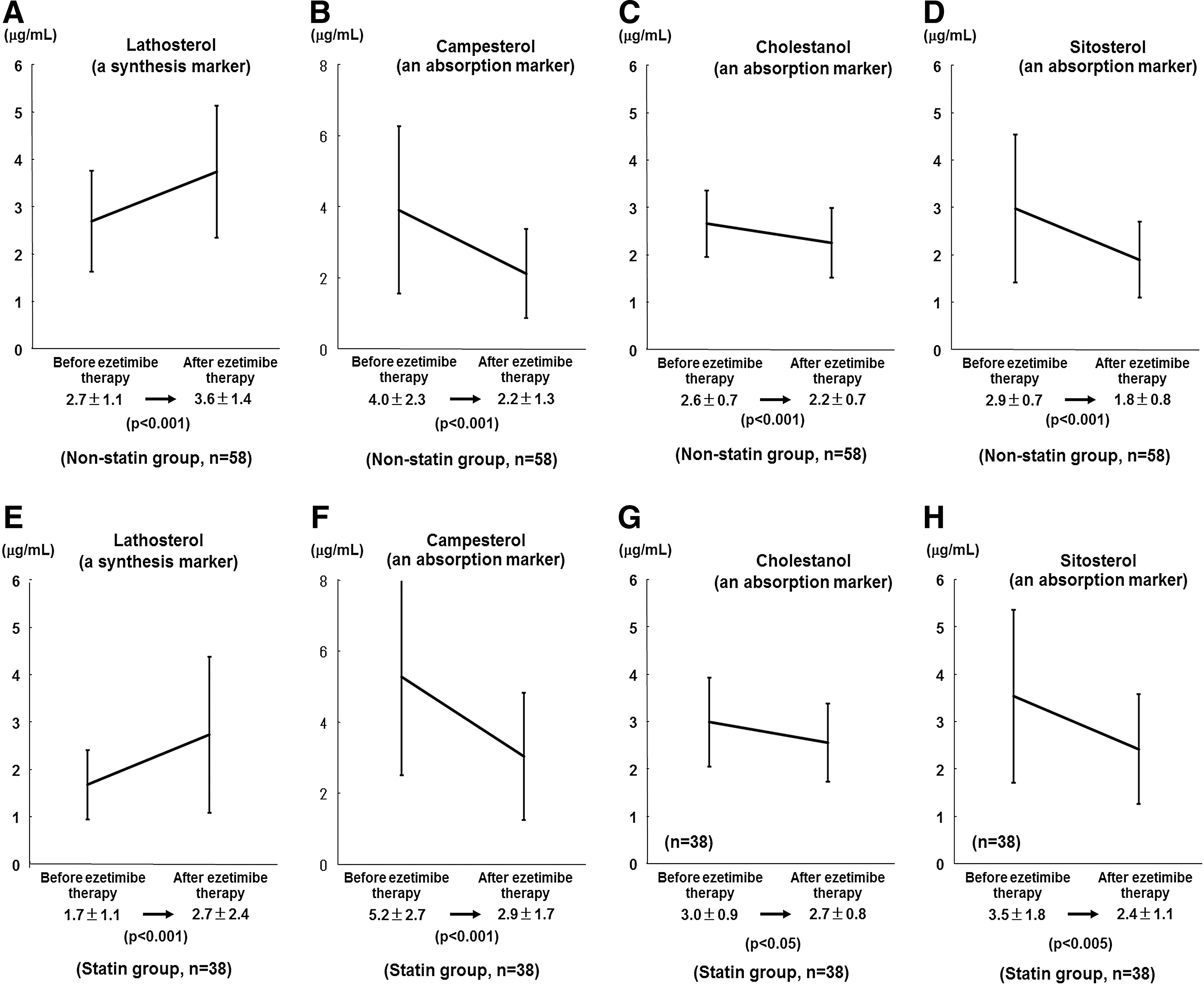
Changes in cholesterol absorption/synthesis markers during the 12-week ezetimibe therapy in the
Discussion
Previous large studies with statin showed that, with or without DM, there was positive correlation between LDL-C and the incidence rate of coronary events 21 and that the incidence rate of coronary events was lower as the ultimate LDL-C level was lower. 22 In addition, because the proportion of small dense LDL having a high ability to induce arterial sclerosis increases in patients with DM, 23 it seems reasonable that the target level of apparent LDL-C should be set at a lower level in patients with DM than that in patients without DM.
However, in reality, despite addition of statin therapy to dietary therapy and exercise therapy, few patients with DM achieved target LDL-C levels. 20 This low rate may be partially due to a poor compliance with statin therapy but can be mainly explained by the fact that the LDL-C-lowering effect tends to be less strong in patients with an increased cholesterol absorption. 13 Cholesterol absorption will increase, especially in patients with DM, probably because of an increased expression of NPC1L1, which facilitates cholesterol absorption in the small intestine, and decreased expressions of ABCG5 and ABCG8, which bring cholesterol back to the small intestinal lumen from small intestinal epithelial cells. 24,25 In the present study, we also confirmed that serum LDL-C levels were positively associated with cholesterol absorption markers but were not associated with a cholesterol synthesis marker in diabetes subjects with hypercholesterolemia, whether they were receiving statins or not (Fig. 1). The results suggested that serum LDL-C levels are more strongly related to cholesterol absorption than synthesis in this population, and thus we should reinforce the importance of dietary therapy for diabetes subjects with hypercholesterolemia. It is also assumed that the administration of an inhibitor of cholesterol absorption can be an effective approach for reducing serum LDL-C levels in this population.
Therefore, to test the above hypothesis, we next performed a single-arm prospective study. This study demonstrated that cholesterol absorption markers significantly decreased (Fig. 5) and serum lipid profiles, including LDL-C levels, significantly improved (Fig. 3) during a 12-week ezetimibe treatment period, whether statins had been administered or not (Fig. 5). These results suggest beneficial effects of ezetimibe on cholesterol absorption as well as serum lipid profile in Japanese type 2 diabetes patients with hyper-LDL-cholesterolemia.
It is interesting that serum levels of cholesterol absorption markers at baseline were significantly higher in the subjects who were receiving statins compared with those were not (Fig. 2), suggesting that cholesterol absorption was up-regulated in these subjects. Because the addition of ezetimibe to statin therapy can prevent the statin escape phenomenon, it is expected that ezetimibe can provide a higher LDL-C-lowering effect in these patients. Indeed, the current study showed that the LDL-C-lowering rate was greater in the Statin group than in the Nonstatin group (Fig. 4). However, despite our expectation, there were no between-group differences in the changes in cholesterol absorption markers. Regardless, ezetimibe concomitantly used with statin inhibited cholesterol synthesis/absorption adequately and lowered LDL-C significantly in patients with type 2 diabetes complicated by dyslipidemia. Thus, ezetimibe might be useful for management of hypercholesterolemia, especially in diabetes subjects, although the American College of Cardiology/American Heart Association guideline does not recommend the use of ezetimibe owing to the lack of evidence of atherosclerotic cardiovascular diseases.
Furthermore, combination therapy of ezetimibe and statin may be more desirable than statin monotherapy from a safety standpoint, especially in those who have concerns about tolerability due to reduced drug metabolism. Although aggressive therapy with high-dose statins has been shown to provide clinical benefit, it should be used more conservatively in patients with an increased risk of adverse events because of advanced age and concomitant illnesses such as advanced diabetes complications. In addition, combination therapy may deliver complementary effects on lipids that surpass those of statin monotherapy titrated to higher doses, by providing comparable tolerability.
Thus, ezetimibe can be a good clinical option as an additional drug for patients in whom the therapeutic effect of statin monotherapy was insufficient or as an option for patients in whom statins cannot be used. Needless to say, ezetimibe itself is not completely exempt from side effects, including liver dysfunction and myopathy. However, the incidence of adverse effects in ezetimibe-treated patients is low, whether it is used as the sole regimen or in combination with a statin. 26,27 Indeed, no apparent adverse effects were observed during the 12-week follow-up period in the present study.
Several limitations of our study should be discussed. First, this was a single-arm uncontrolled study with a relatively small number of subjects. Therefore, the utility of ezetimibe in Japanese type 2 diabetes patients with dyslipidemia should be verified in further studies. Second, because the observation period was relatively short, the long-term effect of ezetimibe treatment should be evaluated in another study. Third, because all the study subjects had type 2 diabetes, the current study cannot answer the question of whether the therapeutic effects of ezetimibe are greater in subjects with DM compared with those without it. Finally, it should be noted that the subjects of this study were Japanese type 2 diabetes patients. It would thus be premature to generalize our findings to other racial or ethnic groups.
Notwithstanding these limitations, this prospective study indicates that new administration of ezetimibe to Japanese type 2 diabetes patients can reduce cholesterol absorption and improve serum lipid profile, whether the patients had been receiving statins or not.
In conclusion, our study suggests that ezetimibe improves the lipid profile in Japanese type 2 diabetes patients with dyslipidemia through the substantial reduction of cholesterol absorption.
Footnotes
Acknowledgments
This research was funded by Osaka University.
Author Disclosure Statement
N.K. is a staff member of the Department of Metabolism and Atherosclerosis and holds an endowed chair donated from Kowa Pharmaceutical Co. Ltd. I.S. has received lecture fees from Takeda Pharmaceutical Company, MSD, and Boehringer Ingelheim and research funding from Eli Lilly Japan, Novartis Pharmaceuticals, MSD, Sanofi-Aventis, Shionogi Inc., Daiichi Sankyo, Inc., Takeda Pharmaceutical Company, Teijin Pharma Ltd., Eli Lilly Japan, Boehringer Ingelheim, Novo Nordisk Pharma, and Mochida Pharmaceutical Co., Ltd. T.K., Y.I., Y.Y., T.O., F.K., Y.K., I.N., K.Y., K.S., H.K., and K.K. declare no competing financial interests exist.