
Abstract
An implantable, glucose-responsive insulin delivery microdevice was reported previously by our group, providing rapid insulin release in response to hyperglycemic events and efficacy in vivo over a 1-week period when implanted intraperitoneally in rats with diabetes. Herein, we focused on the improvement of the microdevice prototype for long-term glycemic control by subcutaneous (SC) implantation, which allows for easy retrieval and replacement as needed. To surmount the strong immune response to the SC implant system, the microdevice was treated by surface modification with high-molecular-weight polyethylene glycol (PEG). In vitro glucose-responsive insulin release, in vivo efficacy, and biocompatibility of the microdevice were studied. Modification with 20-kDa PEG chains greatly reduced the immune response without a significant change in glucose-responsive insulin release in vitro. The fibrous capsule thickness was reduced from approximately 1,000 μm for the untreated devices to 30–300 μm for 2-kDa PEG-treated and to 30–50 μm for 20-kDa PEG-treated devices after 30 days of implantation. The integrity of the glucose-responsive bioinorganic membrane and the resistance to acute and chronic immune response were improved with the long-chain 20-kDa PEG brush layer. The 20-kDa PEG-treated microdevice provided long-term maintenance of euglycemia in a rat model of diabetes for up to 18 days. Moreover, a consistent rapid response to short-term glucose challenge was demonstrated in multiple-day tests for the first time on rats with diabetes in which the devices were implanted. The improvement of the microdevice is a promising step toward a long-acting insulin implant system for a true, closed-loop treatment of diabetes.
Introduction
I
An ideal insulin delivery system should provide sustained basal insulin at low glycemic levels, along with responsive, pulsatile release during periods of hyperglycemia. In addition, a “smart,” on-demand delivery system that can provide a “hands-off” means to minimize hyper- and hypoglycemic episodes without patient intervention would improve quality of life and clinical outcomes. To date, the existing technologies based on integration of electronic continuous glucose monitors and mechanical parts (pumps) and algorithms are still far from achieving this goal. 7 –13 In addition, the overall cost of the electromechanical devices and accessories could limit the number of uninsured patients who can afford the therapy or even have access to it at all. 8,10
Other approaches, such as oral, intranasal, and transdermal delivery, have been explored, yet there remain concerns about clinical efficacy, low bioavailability due to limited penetration, absorption, or enzymatic degradation before reaching the site of action. 14 –23 Furthermore, these systems can only provide patient-mediated, open-loop insulin delivery.
Sustained insulin implant systems have shown promise through the use of polymeric materials and microdevices with long periods of efficacy, which can provide basal insulin. 24 –26 However, they must be used in conjunction with fast-acting insulin injections and cannot provide rapid, pulsatile insulin release in response to glycemic challenge without strict patient intervention and compliance. To this end, chemically driven closed-loop insulin systems using stimulus-responsive polymer hydrogels could overcome the aforementioned limitations. They do not require complex electronic and mechanical parts, reducing the cost and complexity of potential implant systems, while providing real-time glucose sensing and insulin delivery as needed. In such “closed-loop” insulin therapy systems, seamlessly integrating the glucose-sensing component with the insulin delivery mechanism is paramount.
Responsive polymer hydrogels have been studied extensively to provide cyclic, pulsatile insulin delivery. A pH-responsive hydrogel as nano- or microparticles, film, or bulk device has been used to modulate insulin release, by the ionization of the anionic or cationic pH-responsive polymer moieties, which causes shrinking or swelling of the hydrogels. 27 –29 Glucose-specific enzymes (e.g., glucose oxidase) have been well studied in glucose-responsive insulin delivery systems. Glucose oxidase converts environmental glucose into gluconic acid, creating an acidic pH trigger to elicit a response from pH-sensitive polymeric materials. 27 –34 As a result, the glucose-responsive systems undergo cyclic response to glucose levels, providing faster or slower insulin release through polymer membranes, microspheres, or bulk hydrogels via a diffusion-controlled mechanism. 32 –43
Based on a bioinorganic nanocomposite membrane, our group has developed implantable microdevices that deliver insulin at physiological and clinical glucose levels. Rapid, pulsatile insulin delivery and in vivo efficacy for 5–10 days were obtained with these devices when implanted in the intraperitoneal (IP) cavity. 44,45 Within these devices, a glucose-sensing, enzyme-based bioinorganic membrane is integrated with a silicone-based insulin reservoir. The increase in glucose concentration results in faster production of gluconic acid catalyzed by glucose oxidase. This acidic product causes the shrinkage of poly(n-isopropylacrylamide-co-methacrylic acid) hydrogel nanoparticles embedded in the bioinorganic, albumin-based membrane. The porosity across the membrane is thus increased owing to vacated “nanopores” created by the collapse of nanoparticles, which leads to an instant increase in insulin diffusion (Fig. 1). Owing to rapid response of pH-sensitive nanohydrogels, the device enabled rapid attenuation of plasma glucose levels in vivo after a glucose bolus injection, mimicking a physiological response to the postmeal hyperglycemia in a healthy subject. 44
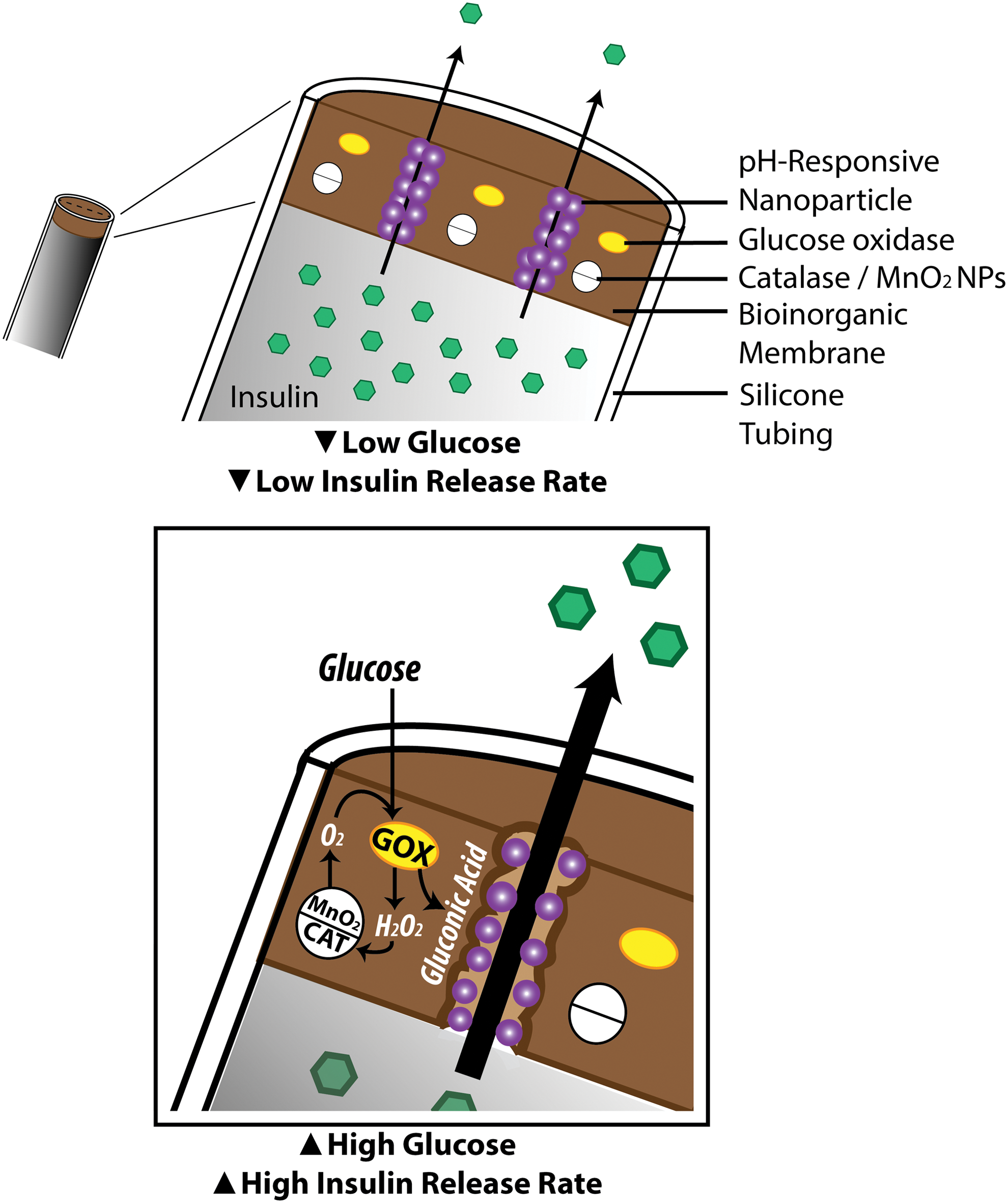
Schematic for glucose-responsive insulin microdevices:
For long-term application and patient safety, easy retrieval and replacement/refill of the implants are important. To this end, subcutaneous (SC) implantation is preferred over IP implantation. Moreover, the stability and longevity of the device, in particular, the glucose-responsive membrane, are crucial. Our preliminary study suggested that the previous version of the device was susceptible to heavy fibrous capsule formation when implanted either IP or SC. Degradation of the bioinorganic membrane also occurred after 2 weeks, owing to cellular adhesion and immune response from destructive cell-mediated oxidization, which compromised long-term application of the microdevice.
Therefore, this work was aimed to optimize the microdevice for SC implantation and improved longevity in vivo. We improved the system design by modifying the surface of the microdevices to reduce immune response from the host to the implants and investigated the effect of polyethylene glycol (PEG) chain length on the inflammation and foreign body response in rats with diabetes.
Materials and Methods
Materials
All chemicals were analytical grade and used without further purification. Bovine serum albumin (99%), catalase (solution 13 mg/mL), 3-aminopropyltrimethoxysilane (97%), glutaraldehyde (25%, grade I), PEG methyl ether (mol wt, 2,000 and 20,000), 4-nitrophenyl chloroformate (NPC), and tripentylamine (TPA) were purchased from Sigma-Aldrich (St. Louis, MO). Glucose oxidase (230 U/mg) was purchased from Calzyme (San Luis Obispo, CA). Recombinant human insulin (recombinant DNA origin; 27 U/mg) was purchased from Wisent (Saint-Jean-Baptiste, QC, Canada). Pluronic® F-68 and F-127 were provided by BASF Corp. (Ludwigshafen am Rhein, Germany). 4-(2-Hydroxyethyl)-1-piperazinepropanesulfonic acid (HEPPS) was from MP Biomedicals (Santa Ana, CA). Silicone tubing (Nalgene® 50 silicone tubing; inner diameter, 1.6 mm; outer diameter, 3.2 mm; wall, 0.8 mm) was purchased from Nalgene (Rochester, NY). Ethylene-vinyl acetate copolymer resin (EVAC, ELVAX-40W) was provided by E.I. Du Pont (Wilmington, DE). Poly(n-isopropyl acrylamide-co-methacrylic acid) (NIPAM/MAA) nanoparticles (200±110 nm in diameter in pH 7.4 phosphate-buffered saline [PBS] and 60±50 nm in diameter in pH 5.0 PBS, volume distribution) and powder nano-MnO2 (80±30 nm) were prepared as previously described by our group without further modifications. 36,37 Distilled, deionized water was obtained from a Milli-Q® water purifier (Millipore Inc., Billerica, MA). PBS at pH 5.0 or pH 7.4 was prepared with 0.01 M phosphate and 0.15 M NaCl in distilled, deionized water.
Activation of PEG chains
mPEG with 2 kDa or 20 kDa was activated with NPC as described elsewhere. 37 In brief, NPC and TPA were mixed in the molar ratio 1:5:5 (PEG:TPA:NPC). mPEG (2 g) was dissolved with toluene (20 mL) under a nitrogen atmosphere. The temperature of the resulting solution was increased to 60°C, and 0.15 mL of TPA was added, followed by 100 mg of NPC. After 24 h under stirring, the temperature was reduced to 35°C, 20 mL of methyl-tert-butyl ether was added, and the solution was allowed to stir for 5 min. The reaction flask was then placed in an ice bath, and the resulting thick slurry was stirred for another 30 min. The obtained solid was isolated by centrifugation (at 3,000 rpm; IEC 243 rotor [Thermo, Waltham, MA]), dried under vacuum, and redissolved with methanol (10 mL) at 40°C. The methanol solution was added dropwise in ice-cold isopropanol (30 mL) under stirring, and the white solid obtained was collected by centrifugation (at 3,000 rpm, IEC 243 rotor [Thermo]). The washing step was repeated two more times to remove unreacted molecules, and the final product was dried under vacuum for 24 h at room temperature. The activation of mPEG with NPC was confirmed by using a proton 400-MHz 1 H nuclear magnetic resonance spectrometer (Varian Mercury 400; Varian Inc., Palo Alto, CA). 45
Preparation of microdevices
Glucose-responsive bioinorganic microdevices were prepared as previously described. 35 In brief, medical-grade silicone tubing (a length of 3 cm) was surface treated with oxygen plasma and silanized with 3-aminopropyl trimethoxysilane (0.1 M in ethanol). Silanized devices were cross-linked with a mixture of bovine serum albumin (51 wt%) glucose oxidase (5.5 wt%), catalase (1.56 wt%), MnO2 nanoparticles (11 wt%), and NIPAM/MAA nanoparticles (30 wt%) to create a bioinorganic membrane at one end of the tubing. Glutaraldehyde was used as a cross-linker (0.08:1 mol crosslinker-to-protein ratio). The other end of the tubing was sealed with EVAC solution (18% [wt/vol] in dichloromethane). Surface PEGylation of microdevices was achieved by soaking in 0.1 M activated PEG solution in pH 7.4 PBS for 24 h. Microdevices were washed several times with distilled, deionized water. The devices were stored in pH 7.4 PBS at 4°C prior to use. Prior to both in vitro and in vivo studies, devices were filled with buffered insulin solution (human insulin, 50 mg/mL; HEPPS, 50 mM; Pluronic F-68, 0.02 M; pH approximately 8) (approximately 50 μL containing 2.5 mg or 67.5 units of insulin per device). A thin needle (27½ gauge) was used, and air bubbles were prevented by piercing a second needle in the opposite side of the device during the filling step. Devices were stored in pH 7.4 PBS at 4°C prior to use.
In vitro test of glucose responsiveness of the device
Microdevices were placed in glass vials containing pH 7.4 PBS (2 mL) and glucose (100 mg/dL) as release medium and placed on a rotary mixer at 37°C for the duration of the experiment. Insulin release was determined by monitoring insulin absorbance manually with a ultraviolet/visible spectrophotometer (Lambda 25 UV/VIS spectrometer; Perkin Elmer, Norwalk, CT) every 30 min at λ=276 nm. Glucose concentration was increased from normal (100 mg/dL, 0–2 h) to hyperglycemic levels (400 mg/dL, 2–4 h) halfway through the duration of the experiment.
Implantation of the insulin delivery device in rats
All in vivo procedures strictly complied with the ethical and legal requirements under Ontario's Animals for Research Act and the Federal Canadian Council on Animal Care guidelines for the care and use of laboratory animals and were approved by the University Animal Care Committee of the University of Toronto.
Animals
Male Sprague–Dawley rats (weighing 250–300 g) were used, and diabetes was induced by IP injection of streptozotocin (STZ) (65 mg/kg in sterile saline). Animals were allowed 3 days of resting to confirm the diabetes state. For all experiments rats were kept in a 12:12-h reverse light cycle state and fed chow and water.
Biocompatibility and in vivo stability of the microdevice
For the experiment devices were prepared with different surface treatments (no PEG, 2-kDa PEG, and 20-kDa PEG). STZ-treated rats were randomized into three groups (n=3 per group) and implanted SC with silanized (no PEG) or PEGylated (2- or 20-kDa PEG) insulin devices in the interscapular tissue of the abdomen. Each animal served as its own control and was implanted with the three different surface-treated devices, each one in a separate SC pocket. After a 15- or 30-day implantation period, animals were sacrificed, and the devices with surrounding tissue were carefully explanted. Retrieved devices encapsulated with newly formed surrounding tissue were fixed in 10% buffered formalin and embedded in paraffin for histological analysis. Cross-sectioned slices were stained with hematoxylin and eosin, MAC2, and Mason's trichrome to identify and quantify immune cells, macrophage recruitment, and collagen capsule thickness, respectively. To determine membrane degradation, explanted devices were fixed with buffered formalin and surface morphology was analyzed by environmental scanning electron microscopy (eSEM) (model S3400 microscope, 15 kV; Hitachi, Tokyo, Japan). Wet devices were directly fixed onto a cold-stage sample holder with double-sided carbon tape and frozen at −24°C under a pressure of 90 Pa. Tissue preparation and histology analysis were performed by the CMHD Pathology Core Laboratory at Mount Sinai Hospital, Toronto, ON, Canada.
In vivo glucose responsiveness of the device: glucose challenge test
Long-chain (20-kDa) PEG-treated microdevices were implanted in STZ-treated rats as described above (three devices per animal, n=5) and allowed to rest for 72 h to confirm the decrease of blood glucose (BG) to normal levels by the insulin release from the implant. One hour prior to the experiment, food was removed from cages to prevent confounding glycemic overlap. Rats were given an IP injection of glucose (1 g/kg, 50% dextrose), and their BG levels were continuously monitored during a 90-min period using a One Touch® glucometer (LifeScan, Inc., a Johnson & Johnson Company, Milpitas, CA) with blood samples taken from the tail vein. At the end of the experiment food was returned to the cages, and animals were allowed to rest for 24 h. The experiment was repeated with the same group of animals for 3 consecutive days. Healthy animals without diabetes were used as controls for comparison (n=3).
In vivo long-term efficacy of the microdevice
STZ-treated rats were implanted with 20-kDa PEG microdevices as described above (three devices per animal, n=5). Blood samples were collected daily from the tail vein to determine fed BG and plasma insulin levels. After 21 days, microdevices were surgically retrieved, and animals were maintained for further postimplantation BG measurements. Collected blood samples were assayed to determine insulin levels using an antibody radioimmunoassay kit specific for rat insulin (Linco Research Inc., St. Charles, MO) (the assay kit was used according to the manufacturer's instructions). Rats with diabetes but without implants were used as controls (n=3).
Statistical analysis
Student's t test or analysis of variance followed by Tukey's t test (Origin® Pro 8 software; OriginLab® Corp., Northampton, MA) were used to determine statistical significance between two or more groups, respectively. A P value of <0.05 was considered to be statistically significant.
Results
Effect of PEG chain length on the glucose-responsive insulin release of the microdevice
PEGylation of the device surface was performed through amide bond formation between carboxylate groups of NPC-activated PEG and amine groups in the device surfaces from both protein molecules in the membrane and aminopropyl groups on the silanized device surfaces. 45 PEG chains of different molecular weights (mPEG mol wt, 2,000 or 20,000) were conjugated onto the membrane surface. The effect of PEG chain length on the device performance in vitro and in vivo was investigated to ensure that the chemical treatment would not compromise the ability of the membrane to respond to glucose changes in the environment.
First, the in vitro glucose responsiveness of the devices prepared with 2-kDa or 20-kDa PEG was examined by monitoring the in vitro release of insulin as a function of time and glucose levels, by comparison with control devices without surface modification (no PEG). It is seen in Figure 2 that when the glucose concentration in the release medium was changed from clinically relevant ranges of 100 mg/dL (normal) to 400 mg/dL (hyperglycemia), the ratios of insulin release at hyperglycemia versus normal glucose (R 400/R 100) were all above twofold (Table 1). Moreover, the change in insulin release occurred rapidly, with the insulin release rates increasing almost immediately after the glucose level was increased at 2 h, in all three groups. Release rate in hyperglycemic conditions is the highest initially from 2 to 3 h, with a slight decrease from 3 to 4 h, but the net insulin release is still significantly greater than that at the normal BG level, reflecting the device response to glycemic levels. This result is comparable to previous observations of the insulin microdevice, with a similar ratio of change in insulin release rate. Moreover, the microdevice modifications with PEG surface grafting did not show a significant difference in insulin release profiles. Insulin formulation remained stable within the devices with no observable fibrillation or aggregation, attributable to the treatment with PEG that increases the surface hydrophilicity of the reservoir.
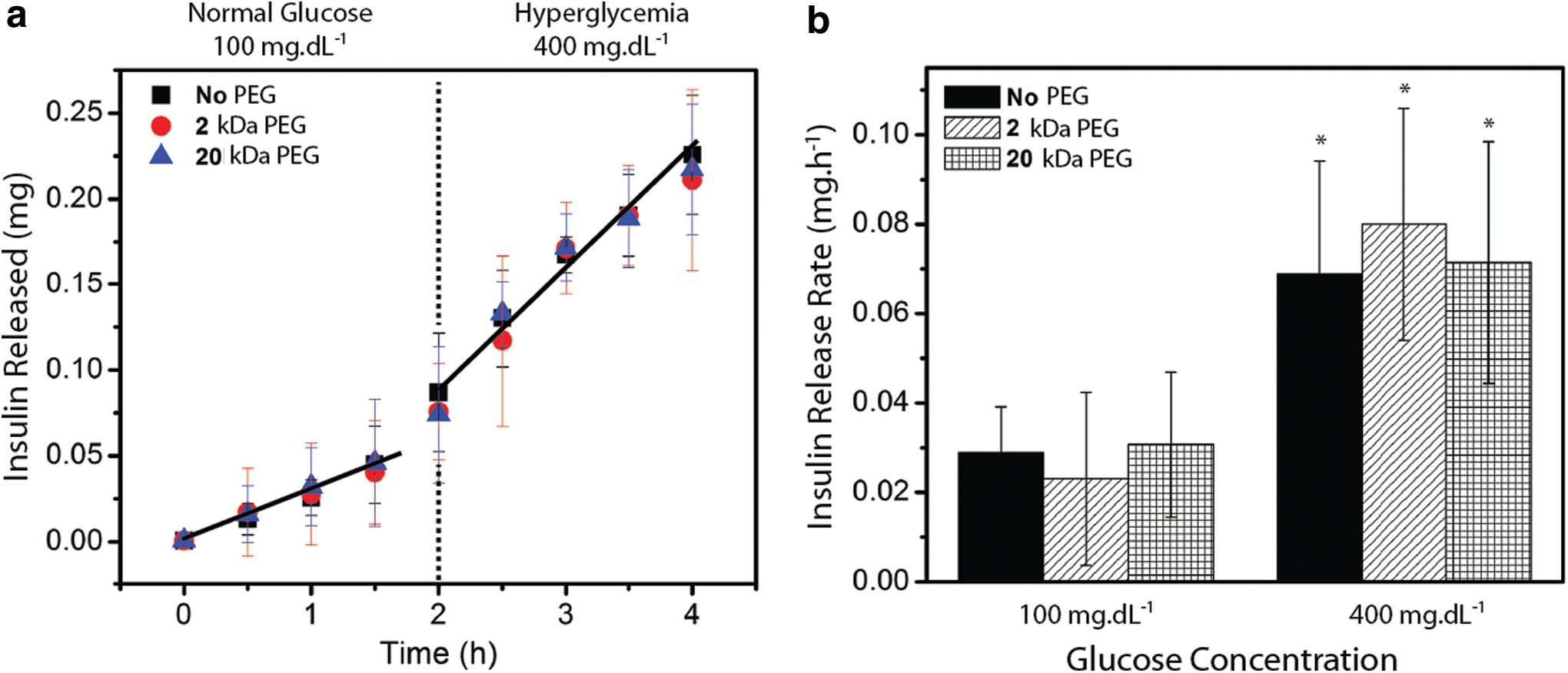
The release ratio was calculated by the release rate at 400 mg/dL glucose (R 400)/release rate at 100 mg/dL glucose (R 100).
Effect of PEG chain length on biocompatibility of the microdevice
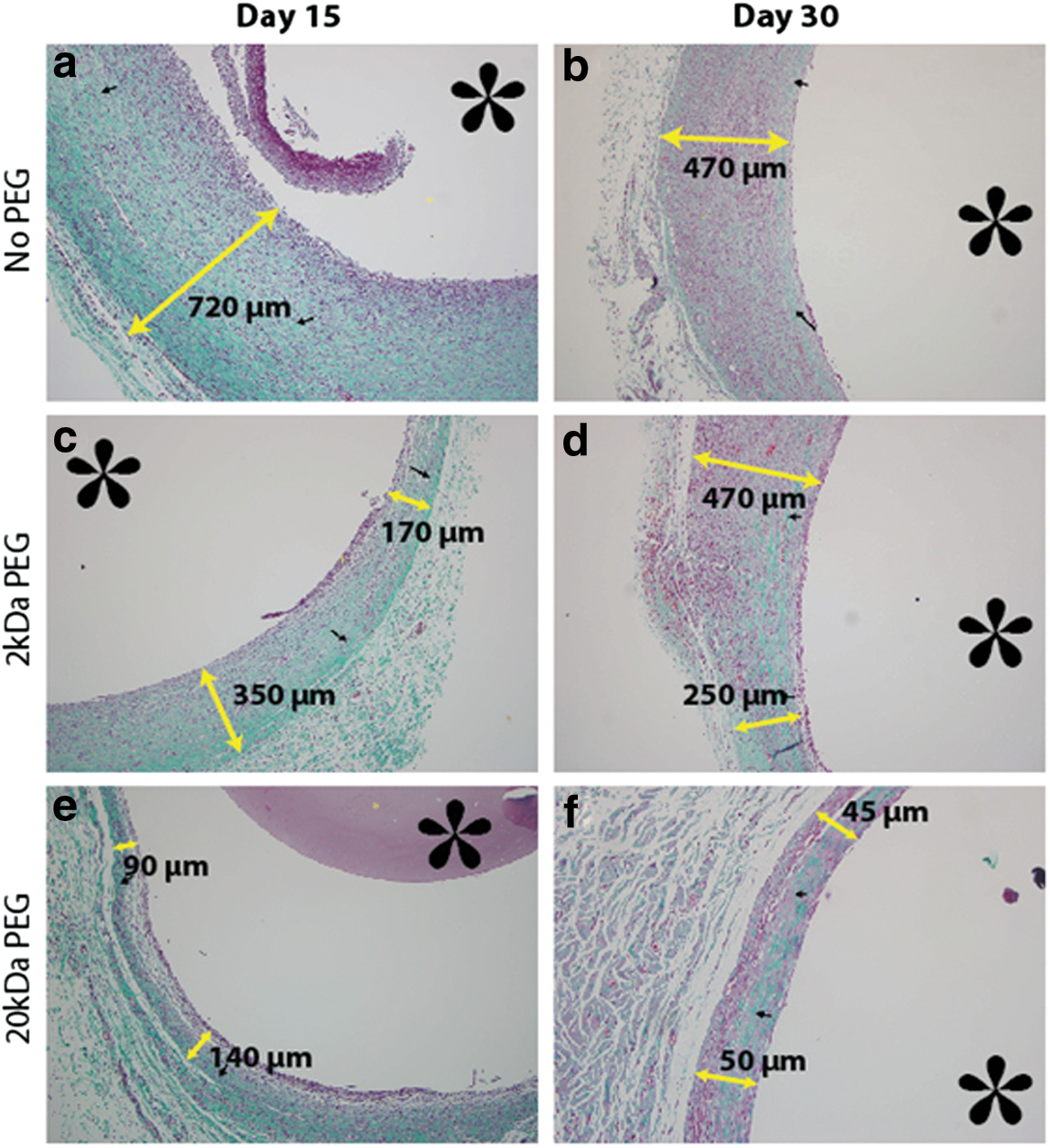
To study whether PEGylation and PEG chain length would influence biocompatibility of the device, such as cell adhesion and immune response, rats were subcutaneously implanted in the abdomen with microdevices treated with no PEG or with 2-kDa or 20-kDa PEG conjugation. After implantation for 15 or 30 days, the devices were explanted. Histological analysis of surrounding tissue around the microdevices showed apparent differences in the thickness of fibrous capsules, immune response, and cell types (Fig. 3 and Table 2). A reduction of inflammation and fibrosis (tissue encapsulation of the device) was observed in the order 20-kDa PEG >2-kDa PEG>no PEG.
PEG, polyethylene glycol.
Capsule thickness was greatest for animals implanted with no PEG microdevices, up to 1,000 μm at 15 days after implantation (Fig. 3a) and 100–500 μm at 30 days after implantation (Fig. 3b). In contrast, PEGylated devices showed thinner fibrous capsule, lower inflammation, and little to no allergic reaction. Devices treated with 2-kDa PEG showed a thinner fibrous capsule with presence of wavy, mature collagen matrix, with a thickness of 100–350 μm (15 days, Fig. 3c) and up to 500 μm (30 days, Fig. 3d). Capsule thickness was further reduced for devices treated with 20-kDa PEG (<100 μm) at both time points and was much more uniform across the entire cross-section (Fig. 3e and f).
At 15 days after implantation, heavy inflammation was seen near the internal capsule walls surrounding the device with no PEG, characterized by dark purple staining from active neutrophil recruitment (Fig. 4a) (a color graphic is available online at
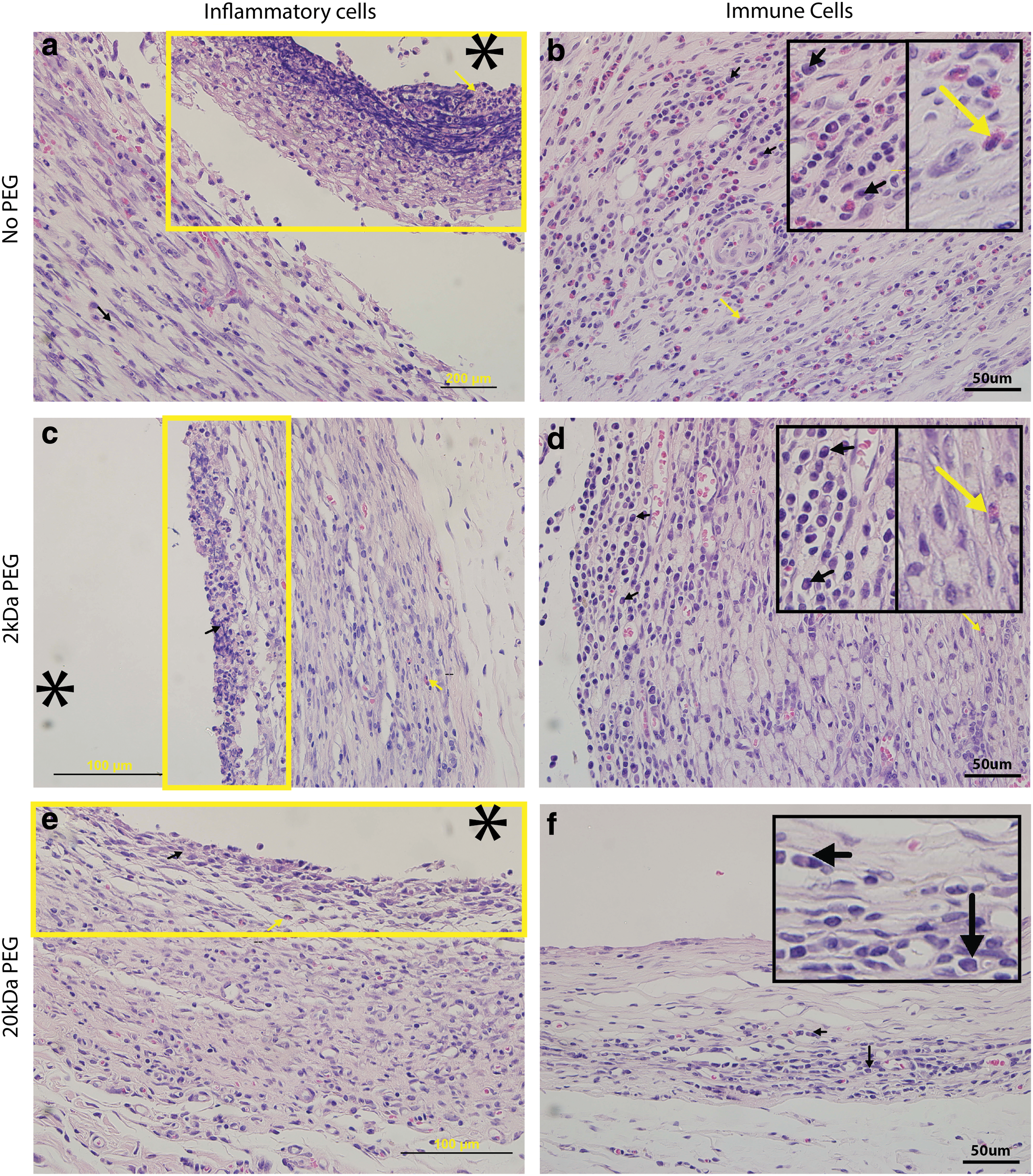
With 20-kDa PEG modification, the internal neutrophil recruitment within the capsules was minimal and presence of eosinophils was insignificant (Fig. 4e and f) compared with the samples surrounding the devices with no PEG or 2-kDa PEG, suggesting very low or absent inflammation and allergic response. All three groups showed the presence of plump plasma cells, an indicator of chronic immune response to foreign material but that are not highly active in cell recruitment and inflammatory response. These results are summarized in Table 2.
Effect of PEG chain length on the morphology and cell adhesion of bioinorganic membrane
For long-term applications, minimal host response to the device and low degradation rates of glucose-responsive membrane are important. In order to evaluate the effect of the surface treatments on the in vivo degradation of the membrane, devices retrieved from animals at 15 or 30 days after implantation were fixed with formalin, and their surface morphology was analyzed by eSEM.
Before implantation (Day 0), devices showed no differences in membrane morphology and integrity as expected between the three groups (Fig. 5a, d, and g). At 15 days after implantation, cell attachment was seen on the membrane with no PEG (Fig. 5b), whereas cell attachment and agglomeration were reduced on the membrane with 2-kDa PEG (Fig. 5e). On the 20-kDa PEG-treated devices, negligible cell attachment was observed (Fig. 5h), an indication of good resistance to initial nonspecific protein attachment and subsequent cascade response. In addition, cellular and protein adhesion on the silicone tubing was easily visible on the devices with no PEG, whereas little adhesion was observed for both PEGylated samples. After 30 days, complete central degradation of the membrane occurred in the devices with no PEG, with obvious damage of the permeable membrane and heavy cellular and tissue adhesion throughout the surface (Fig. 5c). Compared with the device with no PEG, the 2-kDa PEG-treated device showed less membrane degradation and cellular attachment. However, the 2-kDa PEG treatment did not completely prevent intense cell attachment on the membrane surface and the adjacent silicone tubing (Fig. 5f). Further reduction of cellular attachment was obtained when 20-kDa PEG was used. More important is that the images revealed that the integrity of the membrane was not compromised even at 30 days after implantation (Fig. 5i). Little to no cellular adhesion onto the silicone surface adjacent to the membrane was observed, indicating a significant improvement of the biocompatibility of the device by addition of long-chain PEG to the silanized silicone surface.
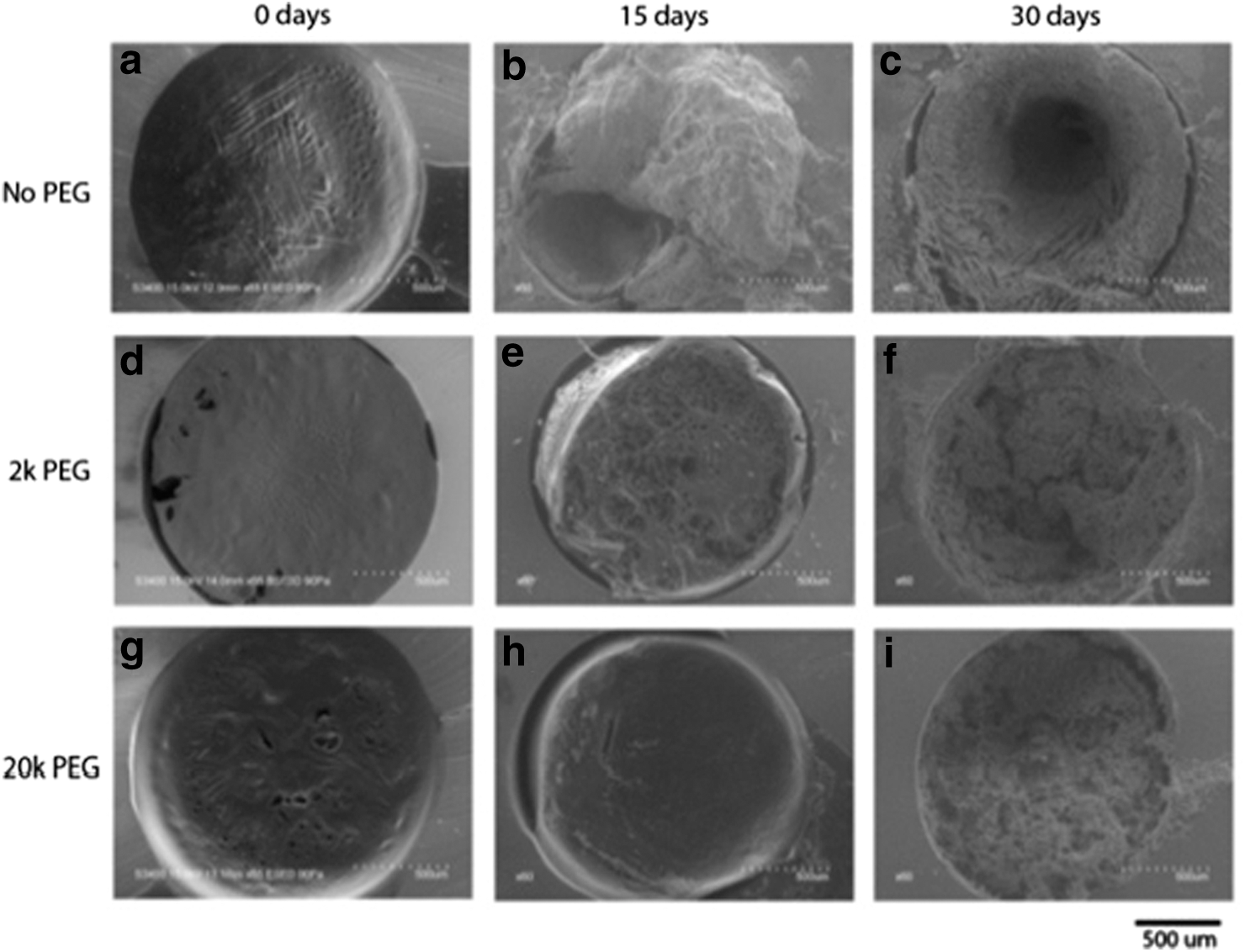
The eSEM results are in agreement with the observations by histological analysis, showing that the PEG treatment can greatly decrease cellular adhesion on the device surfaces in the order 20-kDa PEG >2-kDa PEG>no PEG. Because of the highest biocompatibility and lowest degradation, with negligible change in glucose-responsiveness, the devices modified with 20-kDa PEG were further investigated for their in vivo efficacy.
Long-chain PEG-modified microdevices show multiple-cycle glucose responsiveness in vivo
An ideal closed-loop insulin device should be able to release more or less insulin in response to real-time glucose level changes in vivo, similarly to healthy β-cells. In previous work we have demonstrated in vivo efficacy of insulin microdevices implanted IP over a 5-day period and their effect on rapidly decreasing plasma glucose levels in response to a short-term glucose challenge. 44,45
Herein, we wanted to investigate whether microdevices implanted subcutaneously would present similar in vivo glucose responsiveness and maintain this activity over several cycles. The short-term in vivo performance of the devices was determined by monitoring BG levels in animals with implanted 20-kDa PEGylated microdevices over the time period immediately after glucose bolus injection, to simulate meal-time glucose challenge and glycemic response. The same experiment was performed simultaneously in healthy animals for comparison. Ideal glycemic response of insulin release should minimize the hyperglycemic period and return glucose concentration to euglycemia rapidly. As shown in Figure 6, the implanted insulin microdevices mimic the pancreatic β-cells in healthy rats and bring the glucose level to normal values within 30–60 min in three separate glucose challenge tests at different days, indicating consistent and repeatable performance of the devices.

Multiple-cycle glucose challenge testing for healthy rats (squares) and device-implanted rats with streptozotocin-induced diabetes (circles). Rats were fed for 12 h in between glucose challenge cycles and fasted 1 h before glucose injection until the end of the test. Error bars represent SD (n=3). (A color graphic is available online at
Long-chain PEGylated microdevices show long-term in vivo efficacy
Finally, we wanted to determine whether the optimization of the device would lead to prolonged efficacy for the control of BG in vivo, as compared with our previous device prototypes. Long-term in vivo performance of the microdevice was determined by monitoring glycemia and plasma insulin in SC device-implanted rats with diabetes over a 28-day period. As shown in Figure 7a, rats with diabetes showed very high glucose levels, as expected (>500 mg/dL) throughout the duration of the experiment. In contrast, animals treated with implanted 20-kDa PEG-treated insulin microdevices showed an immediate decrease in BG levels from hyperglycemic (>500 mg/dL) to normoglycemic (75–140 mg/dL) within 24 h. Normoglycemia was maintained over 18 days, without evident episodes of hypo- or hyperglycemia. After 18 days, the glucose level increased outside of normal range (approximately 180–270 mg/dL); however, it was still significantly lower than levels observed in the control rats. Upon device removal from the implanted rats, the BG level increased to hyperglycemic levels, confirming that the glycemic control was provided by the insulin microdevices.
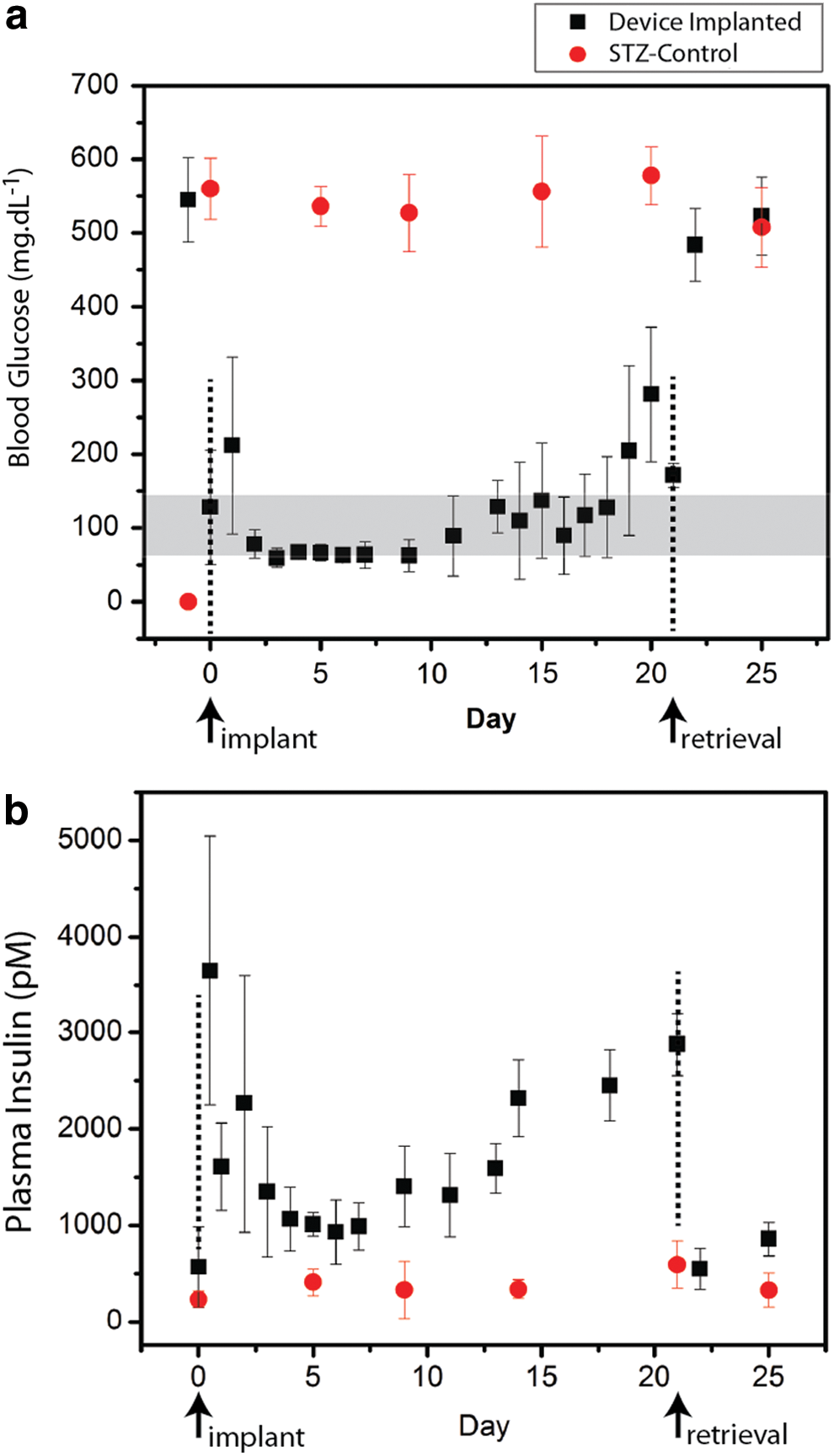
In vivo performance of subcutaneously implanted insulin microdevices in rats with streptozotocin (STZ)-induced diabetes. Microdevices (squares) were subcutaneously implanted at Day 0 and retrieved at Day 21. STZ controls (circles) were not implanted.
Analysis of plasma insulin levels showed an initial increase postsurgery, but steady levels throughout the duration of the experiment (Fig. 7b). A slight increase in plasma insulin levels observed after 15 days (Fig. 7b) seems to not cause hypoglycemia (Fig. 7a), which might suggest that more insulin is needed to maintain euglycemia owing to body weight increase in the rats or partial deactivation of insulin. Despite this return to hyperglycemia, the results are positive when compared with current duration of efficacy of implantable pump–sensor combination devices, such as the MiniMed (Medtronic, Minneapolis, MN) and OmniPod® (Insulet Corp., Billerica) systems, which require replacement of the glucose sensor after 3 days to maintain optimal efficacy. 46,47 Upon removal of the insulin microdevice, insulin levels dropped to preimplantation levels. This result suggests that no endogenous insulin was produced to exert effect on glycemic levels and that the detected circulating insulin was provided solely from the microdevices. All rats in the insulin microdevice-treated group remained healthy throughout the duration of the experiment, with slight weight gain over time.
Discussion
Long-chain PEG surface modification extended in vivo efficacy and reduced host-foreign body response
The closed-loop insulin delivery microdevice was optimized for extended in vivo efficacy with reduced host-foreign body response to the implant. Previously, we have applied advanced surface modification techniques (e.g., silanization) to the microdevice prototype and covalently attached amino-reactive moieties on both the membrane and insulin reservoir surfaces. These advanced surface treatments improved safety, hydrophilicity, and biocompatibility of the device for IP implantation in rats. 42 Through this approach we could improve adherence of the membrane to the insulin reservoir and also avoid aggregation of insulin within the interior of the reservoir that may be induced by contact of the hydrophobic domains of insulin with hydrophobic surfaces. 48 –51 However, the previous prototype microdevice was still susceptible to biodegradation of the glucose-responsive permeable membrane in vivo owing to tissue encapsulation and immune cell response toward the foreign implant. The characteristic porous morphology of the glucose-responsive membrane and its composition (approximately 60% cross-linked proteins) allow relatively free diffusion of substrates and make the exposed hydrophilic membrane vulnerable to degradation in vivo because of cellular infiltration, compared with dense, hydrophobic materials, such as silicone. This is typical with cross-linked hydrophilic implant systems, which is attributed to an oxidative degradation mechanism. 52 –54 Also, the adherence of immune cells on the membrane surface may potentially cause nanopore obstruction and the failure of the microdevice to release insulin, compromising efficacy.
To solve this problem, herein we have attempted to further modify the device surfaces with improved polymeric coatings that resist protein absorption, based off of nonfouling PEG-based surface treatments (PEGylation). Coupling with PEG has been proven to be the most protein-resistant surface modification and remains the standard for biocompatibility comparison. 55 –57 Through PEGylation of the microdevice we decreased the in vivo degradation of the glucose-responsive membrane and at the same time improved the biocompatibility of the implant with minimal response to the host. PEG is known for masking the overall surface of implants by creating a hydrophilic, protein adsorption-resistant, nonfouling brush layer. This leads to less immune cell recognition of the foreign implant/biomaterial and improved short- and long-term biocompatibility. 55 –59 More important is that it is also known that PEG chain length strongly influences nonfouling properties through increased stearic resistance to attachment proteins (Fig. 8). 60,61 To this purpose, we have attempted to increase PEG chain length to further disturb immune cell and protein attachment to improve biocompatibility.
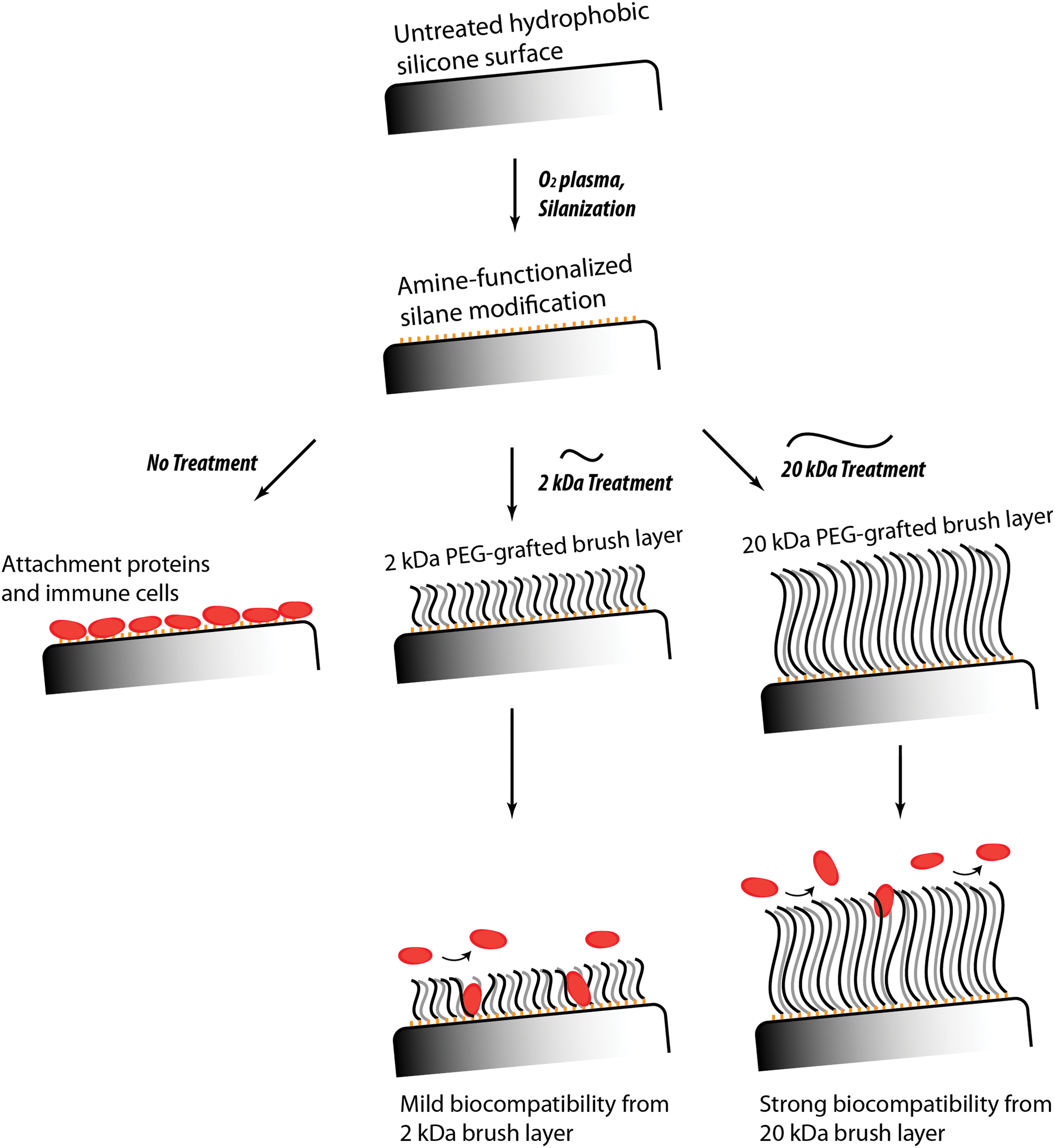
Surface-modification schematic for polydimethylsiloxane (silicone) surfaces. Initial oxygen plasma treatment was followed by silanization and a comparison of three treatment profiles (no polyethylene glycol [PEG], 2-kDa PEG, and 20-kDa PEG). Stearic resistance to immune cell and protein attachment after in vivo implantation is shown. (A color graphic is available online at
The findings showed that the PEGylation of the device leads to marked improvement of short- and long-term implant biocompatibility. Moreover, the improved results of devices treated with 20-kDa PEG compared with 2-kDa PEG define the effect of PEG length on the reduction in both acute and chronic immune response. Negligible recruitment of eosinophils and reduced inflammation on 20-kDa PEG-treated microdevices confer a biofouling resistance to the microdevice surface; this occurs to a lesser extent with 2-kDa PEG. These results agree with previous findings on the effect of PEGylation on implantable materials, which has shown that grafting of a PEG chain layer is an effective deterrent for initial adhesion of blood and immune proteins through dispersion, cross-linking, copolymerization, or grafting. Attachment proteins show reduced adhesion loads when exposed to PEG-treated versus non-PEG treated surfaces, stopping the initial cascade of immune response to foreign bodies. PEG grafting onto a silicone surface has been shown to resist acute bioadhesion and prevent the initial attachment of blood proteins in vivo.
The hydrophilic brush layer shows resistance against attachment protein adhesion, specifically albumin, fibronectin, and fibrinogen, presumably from a sterically mediated mechanism. 57,59 Studies have also shown that extending PEG chain length and density can further enhance this adhesion resistance by increasing the thickness and coverage of the hydrated brush layer, improving “stealthing” of the biomaterial. 56,57 This larger hydration shell around the PEGylated material retards both cellular and protein adhesion and stops the initial cascade toward secondary immune cell recruitment. PEG-modified surfaces have shown improved biocompatibility of SC implant systems by significantly reducing monocyte and macrophage recruitment within acute time periods, 57,58 which coincides with our histology results. We were able to successfully graft long-chain PEG onto our insulin microdevice and significantly improve long-term biocompatibility with SC implantation. It is also important to note the close, inverse relationship between allergy-mediated eosinophil recruitment and PEGylation of the silicone surface, which is promising for potential re-implantation or refilling of our microdevices.
In vivo glucose-responsive performance is improved with 20-kDa PEG-treated devices
Multiple-cycle glucose tolerance testing with device-implanted STZ-treated rats showed rapid glucose-responsive activity. The first cycle was performed after a 4-day implantation period (Day 4), with subsequent cycles being performed on Day 5 and Day 6. As shown in Figure 6, for all cycles, immediately after glucose injection, healthy animals showed an increasing sharp peak in BG level above 180 mg/dL from 0 to 15 min, and the BG level rapidly returned to normal values (80–140 mg/dL) by 30 min. The immediate decrease in BG level is due to the rapid response of the pancreas, releasing insulin from islet cells in response to BG peaks.
Microdevice-implanted animals showed profiles comparable to healthy animals, with a similar return to normal glucose levels within a range of 30–45 min in all three cycles. These results showed the ability of the microdevice to function as a closed-loop system when implanted subcutaneously and its ability to act in real time in response to glucose challenge similarly to a healthy pancreas. The insulin release in response to BG challenge occurs within a tight glycemic window, preventing animals from reaching values above 300 mg/dL. Repeatability in all three glucose challenge cycles shows device consistency, which has not been shown with our system previously.
Despite significantly lower BG levels from 30 to 90 min after the glucose challenge in 2 of the 3 days, hypoglycemia (<65 mg/dL) was not detected in the discontinuous process, suggesting that insulin was not released unspecifically from the highly concentrated depot, which is desirable for the sake of device safety. Moreover, an overshoot of insulin is not likely, as the device released insulin adequately dampening the hyperglycemic challenge without reaching postchallenge hypoglycemic levels. Such a property of glucose-regulated insulin release is very important, as overtreatment of hyperglycemia with excess exogenous insulin can lead to symptoms of hypoglycemic unawareness, which is exacerbated with repeated hypoglycemic episodes. 4,5
As type 1 diabetes patients do not have proper glucagon control, often with glucagon oversecretion, hypoglycemia is a major secondary danger that can arise from improperly managed insulin treatment. Chronic hypoglycemic exposure can lead to deleterious effects on central nervous, vascular, and renal systems. 1 –3 From the cyclic nature of the nanoparticles, low glucose states induce low basal release from implanted microdevices, as expected, and this prevents excess insulin influx and potential hypoglycemic spike. This provides dual attenuation against extreme glycemic states, without the use of glucagon. Not only are primary hyperglycemic conditions minimized, as expected, but hypoglycemic episodes as well. There is an increase in plasma insulin levels at later time points past 15 days, but they do not correlate with a subsequent reduction in BG level. Denatured insulin might exist in the microdevice from long-term implantation; however, it cannot be distinguished from the active form by the radioimmunoassay. Circulating insulin may be contributed from both active and inactive insulin, which could not sufficiently regulate the BG levels that start to steadily increase in later times. Further tests will be needed to analyze insulin in explanted devices with respect to insulin stability and bioactivity.
Long-term in vivo performance was also improved with the optimized 20-kDa PEG-treated SC implant system. Compared with our previous results, the treatment of the device with long-chain 20-kDa PEG extended the efficacy of the implant from 5 to 18 days, over a threefold increase, with minimal hyper- and hypoglycemic episodes. Removal of implanted devices induced a rapid return to hyperglycemia, showing the paramount importance of the SC insulin implant for glycemic control. Furthermore, the SC implantation was achieved through a minor surgical procedure, which is much less invasive than IP implantation. This implantation method also allows for simple removal and potential re-implantation of the device for future extended studies.
Conclusions
We have improved the glucose-responsive insulin delivery microdevice and achieved 18-day in vivo efficacy with SC implantation. A desirable glycemic profile with minimal hyper- or hypoglycemic episode was obtained. The long-chain PEG treatment improved biocompatibility of the device significantly with minimal tissue encapsulation, inflammation, and immune responses. Glucose tolerance testing on rats with diabetes having implanted insulin microdevices over three cycles on different days showed a rapid response to glucose challenge and effective glycemia-regulating capability of the implanted devices, similar to that observed in healthy animals. The results suggest a promising approach to further improve the implantable microdevice to attain a true, long-term “artificial pancreas” system.
Footnotes
Acknowledgments
This work was supported by a MaRS Innovation POP grant, an ORF-RE nanomaterials grant, financial and in-kind support from Sanofi Aventis, and a CIHR equipment grant. An NSERC Canadian Graduate Scholarship to J.L., an Ontario Graduate Scholarship to M.K.L.C., and a Ben Cohen top-up award to both are also acknowledged. Histology was performed by Dr. Hibret Adissu, and tissue preparation and analysis were performed by the CMHD Pathology Core Laboratory at Mount Sinai Hospital, Toronto, ON, Canada.
Author Disclosure Statement
O.P. is an employee of Sanofi-Aventis Deutschland GmbH. M.K.L.C., C.R.G., J.L., A.Z.A., A.G., and X.Y.W. declare no competing financial interests exist.