
Abstract
Background:
Glucose control in artificial pancreas (AP) studies is commonly assessed by metrics such as the percentage of time with blood glucose (BG) concentration below 70 mg/dL or in the nearly normal range 70–180 mg/dL (in brief, time in hypoglycemia and time in target, respectively). In outpatient studies these control metrics can be computed only from continuous glucose monitoring (CGM) sensor data, with the risk of an unfair assessment because of their inaccuracy. The aim of the present article is to show that the control metrics can be much more accurately determined if CGM data are preprocessed by a recently proposed retrofitting algorithm.
Subjects and Methods:
Data from 47 type 1 diabetes subjects are considered. Subjects were studied in a closed-loop control trial prescribing three 24-h admissions. Glucose concentration was monitored using the Dexcom® (San Diego, CA) SEVEN® Plus CGM sensor. Frequent BG reference values were collected in parallel with the YSI analyzer (Yellow Springs Instrument, Yellow Springs, OH). To simulate the few reference values available in outpatient conditions, we down-sampled the YSI data and provided to the retrofitting algorithm only the reference values that would have been collected in outpatient protocols. Time in hypoglycemia, time in target, mean, and SD of glucose profile were computed on the basis of both the original and the retrofitted CGM traces and compared with those computed using the frequently obtained YSI data.
Results:
Using the retrofitted traces, the average error affecting the estimation of time in hypoglycemia and time in target was approximately halved with respect to the original CGM traces (from 4.5% to 1.9% and from 8.7% to 4.4%, respectively). Error in mean and SD was reduced even further, from 10.0 mg/dL to 3.5 mg/dL and from 8.6 mg/dL to 2.9 mg/dL, respectively.
Conclusions:
The improved accuracy of retrofitted CGM with respect to the original CGM traces allows a more reliable assessment of glucose control in outpatient AP studies.
Introduction
I
At present the most exciting use of CGM is online, assisting either in manual diabetes therapy (sensor-augmented pump therapy) or in closed-loop (CL) BG control (the so-called artificial pancreas [AP]; see, for instance, Cobelli et al.
1
for a review). However, CGM could also be key in several offline applications, among which is the evaluation of glucose control achieved in AP studies or, more generally, in any study aiming to assess the efficacy of a glucose control therapy. Unfortunately, possible inaccuracy of CGM data can complicate such an assessment. As an illustrative example, consider the data of Figure 1, displaying CGM (continuous blue line) and BG references measurements (red dashed line) (color graphic available at

Illustrative examples of erroneous assessment of overnight glucose control using continuous glucose monitoring (CGM) (solid blue line) versus frequent blood glucose (BG) reference measurements (red dots interpolated by dashed line). The shaded area denotes the 70–180 mg/dL range.
This problem is relevant in outpatient trials where highly accurate but invasive BG measurement instruments cannot be used, unlike with inpatient clinical testing. The AP community is currently facing this issue, 2 as it is moving from inpatient (the subject of more than 30 articles in the last 7 years [see Cobelli et al., 1 Thabit and Hovorka, 3 and Doyle et al. 4 for reviews]) to outpatient clinical trials.
Because CGM-based glucose control assessment appears to be the only viable option in outpatient clinical studies, several researchers have used CGM in a straightforward manner, accepting the possible inaccuracy produced by this choice. To the best of our knowledge, only four contributions have explicitly proposed methods to mitigate inherent limitations of CGM use for glucose control assessment. 5 –8
The first one, proposed by Kovatchev and Breton 5 and discussed by Beck et al., 2 is a document prepared for the Food and Drug Administration.
In the second contribution, Hovorka et al. 6 proposed two algorithms for CGM-based trial assessment, developed for the Navigator® sensor (Abbott Diabetes Care, Alameda, CA): the first is an offline retrospective CGM adjustment aiming to reduce CGM error; the second, called stochastic adjustment, aims instead to directly reduce the bias in the CGM-based estimation of time in target, time in hypoglycemia, and time in hyperglycemia, by probabilistically accounting for the possibility that the true BG could lie in a different range with respect to that of CGM. The stochastic adjustment method was then analyzed by Kollman et al., 9 showing that it might effectively produce a better estimation of glucose control metrics, but it might also worsen the error, depending on the controller efficacy.
The third contribution by Mitre et al. 7 investigated if it is possible to apply the stochastic adjustment method also to the Medtronic Sof-Sensor® CGM device (Medtronic Diabetes, Northridge, CA). They showed that a straightforward extension is not effective and proposed a different mathematical transformation of CGM data.
The fourth contribution is the “retrofitting” algorithm 8 that, through a constrained deconvolution, enhances CGM by exploiting a few BG reference values.
In this article we consider the Dexcom® (San Diego, CA) SEVEN® Plus CGM sensor, and by using a large clinical dataset, we demonstrate that the error in the assessment of glucose control metrics is significantly reduced by preprocessing CGM traces with the retrofitting algorithm of Del Favero et al. 8
Materials and Methods
Data
Original dataset
Data were collected during a large multicenter inpatient clinical trial, 10 conducted within the European Union–funded project AP@home. 11 The trial aimed to compare two different CL algorithms against the standard open-loop (OL) therapy and involved 47 patients in six European centers. Each patient underwent three admissions, lasting about 24 h and using three different therapies (i.e., OL and two different CL algorithms). Frequent BG measurements were collected throughout the admission, every hour during the night, and at least every 30 min during the day. BG references were measured with the YSI2300 STAT Plus analyzer, and the CGM sensor was the Dexcom SEVEN Plus CGM sensor. More details on the trial can be found in Lujif et al. 10
Outpatient-like dataset
When many accurate BG measurements are available (e.g., about 55 YSI reference values/day in the original dataset), glucose control metrics can be accurately computed without the need to resort to CGM data.
10
In an outpatient setting, there are only a few BG reference values, and CGM data become necessary. Here we emulated the few outpatient reference data by discarding about 80% of the available reference values and by retaining only those that would have been collected in our outpatient protocols.
12
–15
Specifically, we retained: • BG reference values collected at calibration times • BG reference values prescribed prior to the admission and the discharge of the patient • BG check in response to a CGM hypoglycemia alarm • BG reference values collected at mealtime, to compute the meal bolus • BG reference values performed about 2 h after the meal
For each admission, in the outpatient-like dataset we retained a median of 12 (25th –75th percentile: 11–13) samples, which correspond to 21.4% (20.0%-23.6%) of the samples collected during the trial.
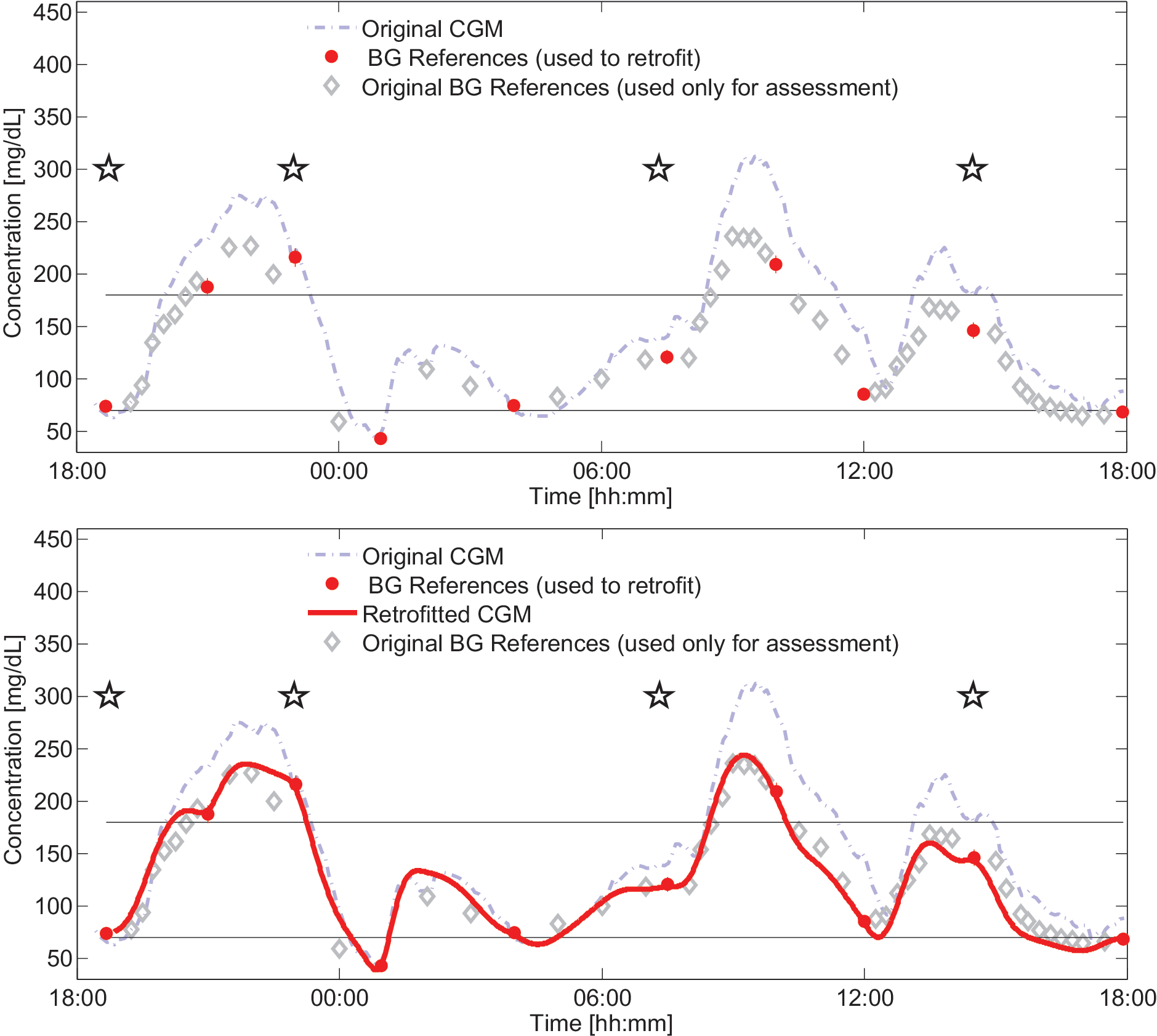
An example of the original and the outpatient-like datasets is illustrated in Figure 2, upper panel (color graphic available at
The retrofitting algorithm
The retrofitting algorithm is described by Del Favero et al., 8 to which we refer the reader interested in the mathematical details of the method. Here we review only that the retrofitting algorithm is a two-step procedure, briefly described by the following.
Step A: retrospective CGM recalibration
This step is designed to correct errors in CGM reading due to under-/overestimation of true glucose values and drift in time due to changes in sensor sensitivity. Recalibration parameters are estimated taking into account and compensating the plasma-to-interstitial fluid glucose transportation delay.
Step B: regularized constrained deconvolution
Recalibrated CGM values are still measurements of glucose concentration in the interstitial fluid and not in the blood. Moreover, no processing has been performed to reduce the noise. Step B processes the recalibrated CGM traces by exploiting also the available reference values to obtain an estimate of the BG profile. The key features of this procedure are as follows: • It compensates for the delay due to glucose transport from plasma to interstitial fluid by deconvolution. • It exploits a physiological prior on the smoothness of the BG profile to filter out the measurement noise. • It takes advantage of the reference measurement to improve the estimate of the BG signal. This is done by introducing the additional constraint that the estimated profile has to lie within the confidence interval of the measurement at the time instant in which a reference BG measurement is available.
Furthermore, a preprocessing step is performed to detect anomalous data and outliers.
Figure 2 (lower panel) illustrates the inputs of the retrofitting algorithm (i.e., CGM [dashed blue line] and the few BG reference [red dots]) and its output, the retrofitted CGM (solid thick red line). We recall that the YSI references represented by the gray diamonds were not used in the retrofitting algorithm.
Glucose control metrics
Gold standard
The availability of frequent YSI measurements in the original dataset allows for accurate computation of glucose control metrics such as percentage of time spent in the nearly normal range (70–180 mg/dL) (time in target), percentage of time spent below 70 mg/dL (time in hypoglycemia), and the mean and SD of the glucose concentration profile. The value of these metrics computed on the basis of all the available YSI measurements will be considered as the gold standard for our analysis.
Outpatient metrics
In outpatient-like conditions the above-mentioned metrics are computed by using either the CGM trace or the retrofitted CGM trace, with the latter being obtained by using the retrofitting algorithm of Del Favero et al. 8 on the CGM trace and the few BG reference values of the outpatient-like dataset.
Comparison
CGM and retrofitted CGM metrics are compared with the gold standard ones. For each patient the absolute estimation error is computed. The difference between the error distributions is tested by using a nonparametric Wilcoxon sign rank test if a Lilliefors test rejects the Gaussian hypothesis or with a paired t test otherwise. To verify if the use of CGM or retrofitted CGM traces induces systematic over-/underestimation, the (signed) estimation error distributions have also been considered. This was done, as in Hovorka et al., 6 by analyzing separately the OL from the CL admissions, to assess the impact of using the same trace both to feed the controller and to evaluate the control achieved. The (signed) error data were tested for the null hypothesis that they come from a normal distribution with zero mean by a parametric t test or, in case of non-normally distributed indices, for the null hypothesis they come from a distribution with zero median by a nonparametric Wilcoxon rank sum test.
Results
The gold standard YSI metrics were compared with CGM and retrofitted CGM metrics. Figure 3 shows a consistent reduction in the absolute errors distribution. For instance, the absolute error introduced using retrofitted CGM profiles rather than YSI to evaluate time in target is not larger than 6.5% in 75% of the cases, whereas, by using CGM, an error larger than 6.6% happens in more than 50% of the cases. The difference between the error distributions was found to be highly statistically significant for all the four considered glucose control metrics (all P<0.001).

Comparison of glucose control metrics using original continuous glucose monitoring (CGM) or retrofitted CGM.
In Figure 4 the two upper panels report the boxplots of the (signed) errors in the assessment of time in target and time in hypoglycemia using either CGM or retrofitted CGM traces with respect to the gold standard YSI metrics (color graphic available at
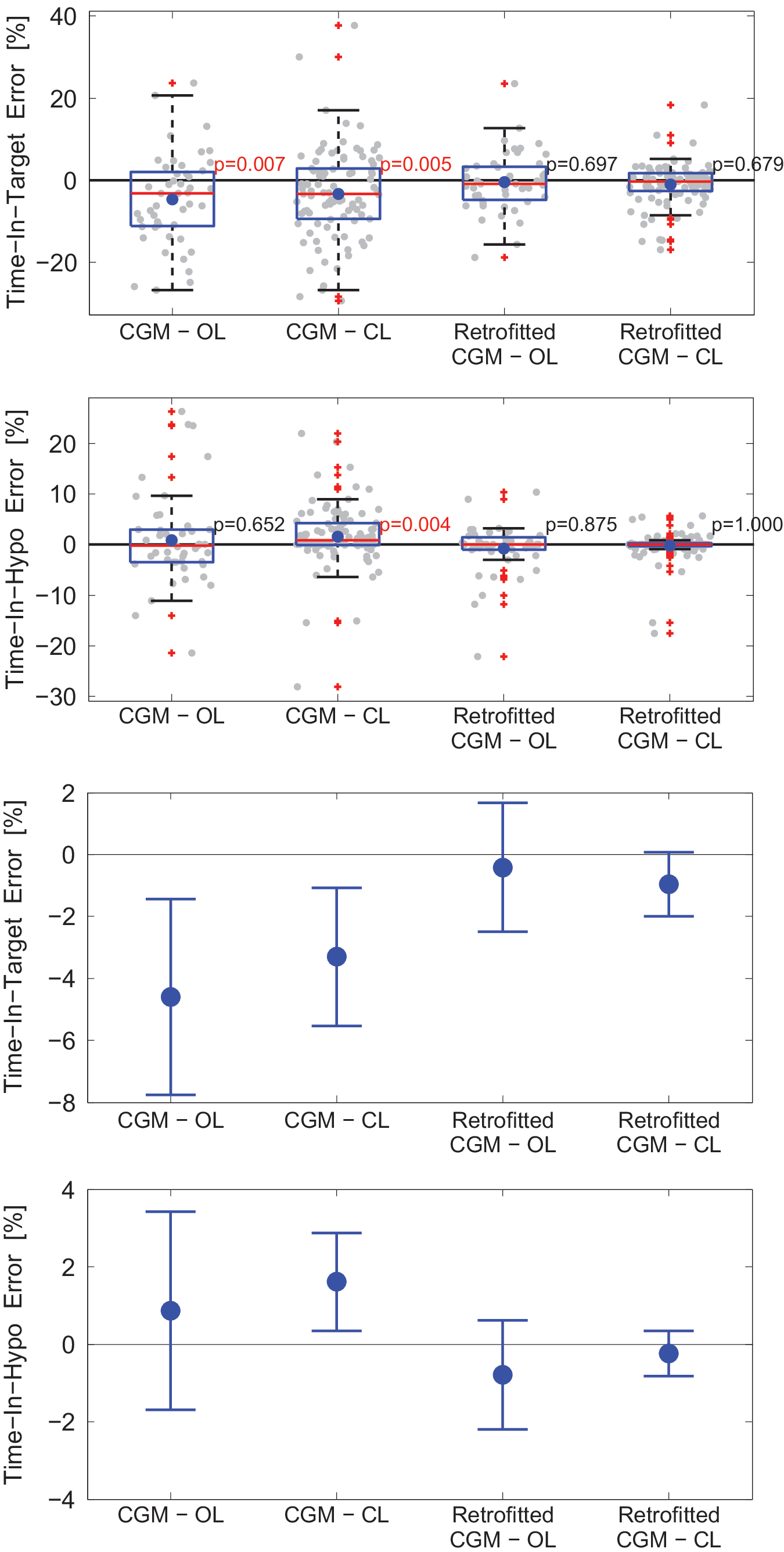
Boxplots of signed errors in
Discussion
Comments on results
The results reported above confirm the preliminary finding of Del Favero et al. 8 and, given the larger size of the used dataset, allow us also to draw stronger statistical conclusions. In particular, it has been shown that, for what it concerns the use of the retrofitted profile to evaluate glucose control achieved during a trial, the retrofitting algorithm not only reduces the assessment errors, but also substantially reduces the bias of this error, in both OL and CL.
Of note is that results on the use of original CGM in CL are not in line with the finding of Hovorka et al. 6 for the Navigator sensor and of Mitre et al. 7 for the Medtronic Sof-Sensor CGM device. In fact, Hovorka et al. 6 showed that CGM-based assessment tends to overestimate time in target and to underestimate time in hypoglycemia in CL but not in OL. As discussed by Hovorka et al., 6 this phenomenon can be explained by the fact that the same CGM profile is used both to feed the controller and to assess the achieved control. The controller strives to bring in target range the CGM trace, but this does not imply that it will bring in target the true BG, especially if a bias between CGM and YSI exists.
With the sensor considered here, the above-mentioned effect is dominated by another phenomenon, illustrated in Figure 2. In this example, it can be noted an overstretching of the CGM trace after the meals, which tends to magnify the glycemic excursions. This effect is well known and is taken into account by the model used within the retrofitting algorithm. The tendency to overstretch of the Dexcom SEVEN Plus has been confirmed by Facchinetti et al. 16 Apparently, the overstretching of postprandial glycemic excursions leads to underestimation of time in target in OL, but the same effect impacts also on CL, because the control algorithm cannot fully compensate for the magnified postprandial excursion keeping the CGM trace in target. Therefore, as forewarned by Hovorka et al. 6 and Hovorka and Nodale, 17 the tendency to inflate time in target when using the same CGM device for both control and performance assessment, observed using the Navigator and Medtronic Sof sensors, cannot be straightforwardly extended to the Dexcom SEVEN Plus sensor. Nonetheless, as suggested by the analysis of Kollman et al., 9 the differences observed here with the behavior observed by Hovorka et al. 6 should not be exclusively imputed to the different sensor model, but also to the different ability of the controllers to maintain in target the possibly erroneous CGM trace.
Comparison with other methods
Regarding a comparison with other techniques, below we considered two standard reference interpolation techniques (linear and cubic interpolations) and the recalibration of Hovorka et al., 6 which represents an excellent example of the simple CGM-informed reference interpolation method. A comparison with Kovatchev and Breton 5 is not possible because, at present, the method is still unpublished. In addition, the correction of Mitre et al. 7 was not considered because it was specific for the Medtronic Sof-Sensor; nor was the stochastic correction method described by Hovorka et al. 6 considered, as it was designed for the Navigator CGM device and would require adaptation to be applied to Dexcom SEVEN Plus data.
Figure 5 reports, for each of the assessed methods, the distribution of the absolute error in the assessment of time in target (Fig. 5, top panel) and time in hypoglycemia (Fig. 5, bottom panel). As is seen, linear and cubic interpolation of the reference values are less effective than CGM-based evaluation, whereas the recalibration by Hovorka et al. 6 allows an improved estimation of glucose control metrics with respect to the original CGM trace. Finally, the higher sophistication of the proposed retrofitting method allows a further improvement in the accuracy.
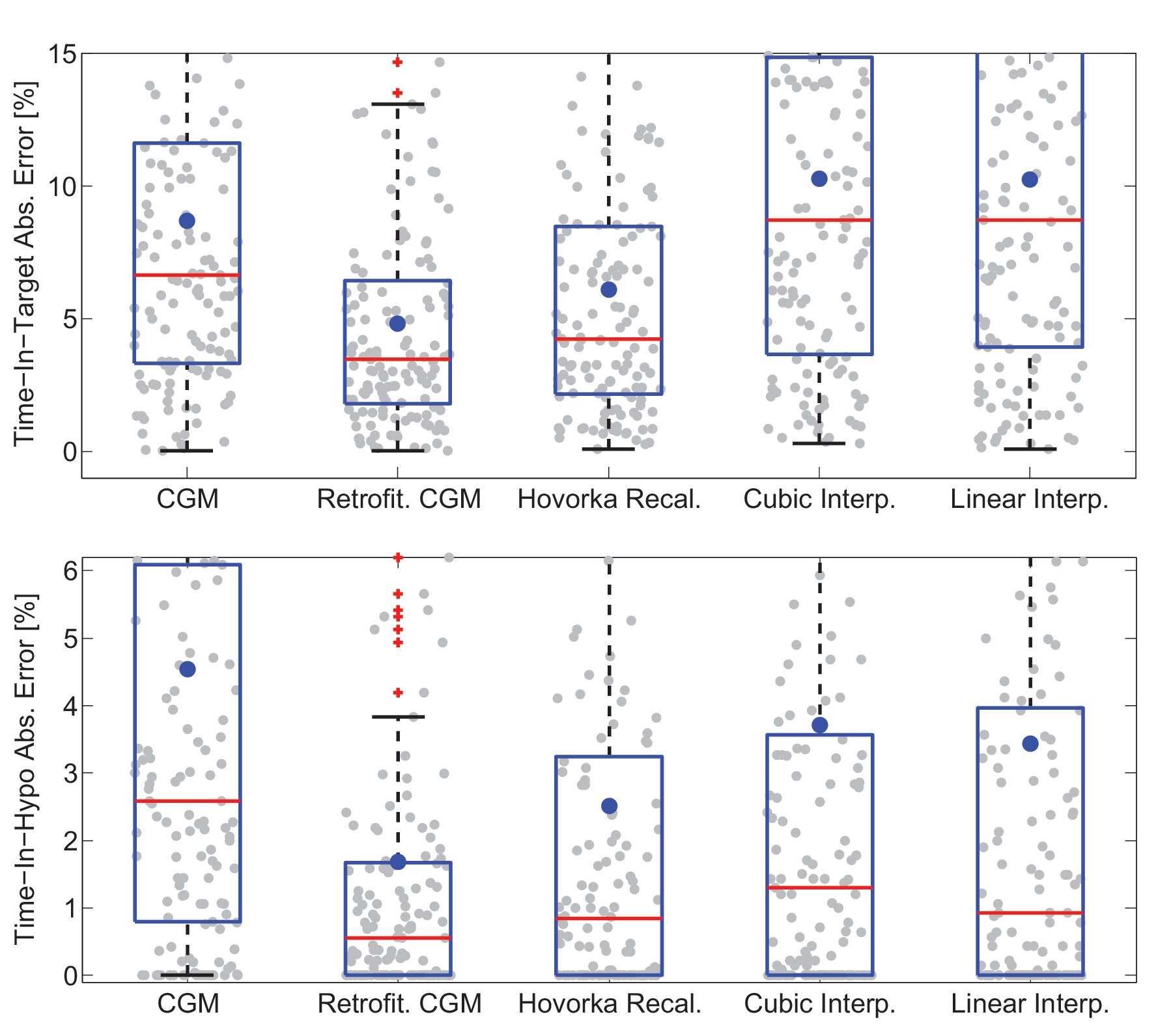
Boxplots of the distribution of the absolute (Abs.) error in the assessment of
Finally, let us remark that a key structural feature of the retrofitting algorithm is that it achieves increased accuracy in control metrics estimation by improving accuracy and precision of CGM. To illustrate this we report in Figure 6, left panel, the boxplot of the relative absolute error of the original CGM trace and of the retrofitted CGM trace (color graphic available at

Accuracy of continuous glucose monitoring (CGM) versus retrofitted CGM.
Figure 6, right panel, reports the boxplots of MARD distribution in the population (each gray dot represents a patient admission). In both panels of Figure 6, errors are computed only on the YSI reference values that were not made accessible to the retrofitting algorithm, to guarantee the fairness of the comparison. Further elaboration on this can be found in Supplementary Data Appendix 1 (Supplementary Data are available online at
Thanks to its capability of improving accuracy, the retrofitting algorithm is well suited to process CGM data in other offline applications (e.g., in modeling applications to achieve more accurate estimates of model parameters).
Comments on the data set-up
The results presented in this article have been obtained on an “outpatient-like” dataset that resembles our outpatient studies 12 –15 and, in particular, has a similar number of reference values with similar accuracy (HemoCue was used in the outpatient studies, YSI here). By doing so we showed that the retrofitting algorithm improves the estimation of glucose control metrics and quantified such an improvement in a practically relevant set-up. Nevertheless, it should be noted that the considered set-up benefits of favorable assumptions in terms of frequency of the reference values and in their accuracy with respect to other outpatient settings. As for any method leveraging on reference measurements to improve CGM, an effectiveness degradation should be expected when less frequent or less accurate reference values are available.
A preliminary evaluation of the method's performance reducing reference frequency has been performed by separating daytime and nighttime, where fewer values were available (only two per night, median value). Details of this analysis are reported and discussed in Supplementary Data Appendix 2. Overnight results are encouraging: the method still allows relevantly improved estimation of glucose control metrics with respect to CGM and improves its accuracy even when fewer references are present. Yet, this analysis does not cover the portion of the day when the variability in glucose is larger. A more comprehensive analysis of the performance degradation when fewer reference values are available is the object of our current investigation.
For what it concerns the problem of using less accurate references, it should be noted that the method accounts for the inaccuracy of a BG reference by constraining the retrofitted CGM profile to lie within the confidence interval associated with that measurement, which will be tighter the more accurate the reference is. So the use of self-monitoring of BG in place of YSI is possible with no methodological changes. Moreover, the retrofitting method has a preprocessing step aiming to detect outliers and hence to perform reference value verification, to increase its robustness to human errors (e.g., wrong manual data insertion but also dirty/wet fingertips, etc.). Yet, despite any possible sophistication of the algorithm, a less accurate assessment of glucose control metrics is expected when using self-monitoring of BG in place of YSI. A detailed quantification of this performance degradation is currently under investigation.
Conclusions
In this article we showed that the CGM retrofitted with the algorithm from Del Favero et al. 8 allows accurate computation of glucose control metrics. Moreover, given its ability to enhance precision and accuracy of CGM, the retrofitting algorithm can be used to process CGM data prior to using them in offline applications.
To conclude, although in this article we proposed a method to improve CGM data, how to interpret such a rich source of information and to make it easily exploitable by caregivers and decision makers remains a challenge. In this regard, effective standardization in reporting of CGM results would be a major step forward.
Footnotes
Acknowledgments
This study was supported by the European Community Framework Programme 7 (FP7-ICT-2009-4 grant 247138).
Author Disclosure Statement
The authors are consultants for Dexcom Inc., San Diego, CA. The authors hold patents and patent applications related to diabetes technology.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.