
Abstract
Background:
Much evidence has shown that pregnancies in women with preexisting diabetes are affected by an increased risk of maternal and fetal adverse outcomes, probably linked to poor glycemic control. Despite great progress in medical care, the rate of stillbirths remains much higher in diabetes patients than in the general population. Recent technological advances in the field of glucose monitoring and noninvasive fetal heart rate monitoring made it possible to observe the fetal–maternal dependencies in a continuous manner.
Subjects and Methods:
Fourteen type 1 diabetes patients were involved into the study and fitted with a blinded continuous glucose monitoring (CGM) recorder. Fetal electrocardiogram data were recorded using the Monica AN24™ device (Monica Healthcare Ltd., Nottingham, United Kingdom), the recordings of which were matched with CGM data. Statistical analysis was performed using a generalized mixed-effect logistic regression to account for individual factors.
Results:
The mean number of paired data points per patient was 254±106, representing an observation period of 21.2±8.8 h. Mean glycemia equaled 5.64±0.68 mmol/L, and mean fetal heart rate was 135±6 beats/min. Higher glycemia correlated with fetal heart rate (R=0.32; P<0.0001) and was associated with higher odds of the fetus developing small accelerations (odds ratio=1.05; 95% confidence interval, 1.00–1.10; P=0.04).
Conclusions:
Elevated maternal glycemia of mothers with diabetes is associated with accelerations of fetal heart rate.
Introduction
A
Subjects and Methods
The study group consisted of 14 white pregnant women with diabetes, treated with insulin. All available patients treated during the 2012–2013 period were assessed for eligibility and asked to participate in the study. The inclusion criteria were set as following: singleton pregnancy >30 weeks of gestation and established type 1 diabetes. We excluded patients with any comorbidities necessitating pharmacological treatment, patients after in vitro fertilization, pregnancies at risk of premature termination, abnormal findings in prenatal ultrasonography, or triple test.
The study was approved by the Bioethics Committee of the Medical University of Lodz, Lodz, Poland. Eligible patients invited to the study, after their informed consent was obtained, were fitted with a CGM recorder (iPro®2; Medtronic, Minneapolis, MN) for a standard, at least 48-h-long, recording. Throughout the study the patients had the option of staying in the hospital or remaining in their own home.
The sensor was placed in the subcutaneous tissue using a dedicated insertion device. Calibration of the CGM device was done using the ACCU-CHEK® glucometer (Roche, Basel, Switzerland), and measurements were performed at least four times per day. The obstetrics team was blinded to CGM recordings during the study, and its results did not influence their clinical management during the study.
The endocrinological team was blinded to fetal electrocardiography data but could adjust insulin treatment depending on current glucose levels when necessary (blood glucose concentration less than 70 mg/dL [3.9 mmol/L] and more than 126 mg/dL [7 mmol/L]). Fetal electrocardiogram (ECG) data were recorded using the Monica AN24™ device (Monica Healthcare Ltd., Nottingham, United Kingdom). All patients were fitted with this device between 1 p.m. and 5 p.m. after a run-in period of at least 3 h of CGM. After a calibration period of the ECG, the recording was started and continued for at least 20 h.
After removal of both devices, the ECG recording was analyzed for a 5-min time frame using the manufacturer's software (Monica DK; Monica Healthcare Ltd.), matched with the CGM recording up to the nearest minute. Small FHR accelerations and decelerations were defined, respectively, as increases in the FHR from the baseline greater than 10 beats/min (bpm) and lasting for at least 15 s and as decreases of ≥10 bpm for ≥10 s. A large acceleration event was defined as an increase greater than 15 bpm and lasting for more than 15 s. A large deceleration event was defined as a fall in FHR from the baseline, where the area below the baseline was greater than 20 beats. Imputation of missing data was not attempted.
The paired CGM/ECG data points were used in the analysis.
Frequency of hypoglycemia (<70 mg/dL [3.9 mmol/L] and <54 mg/dL [<3 mmol/L]) and hyperglycemia (>126 mg/dL [7 mmol/L]) were presented as percentage of the total CGM time. Mean glucose values and three parameters of glycemic variability (SD, M100, and J index) were calculated using an online CGM variability calculator designed by the authors (GlyCulator) and verified using Microsoft (Redmond, WA) Excel™. These indices of glycemic variability were selected as their methodology allows for noncontinuous data, which was the case in our study. 8 –11
Statistical analysis was performed using a generalized mixed-effect logistic regression model to estimate the glucose-dependent risk of FHR disturbances while accounting for individual effects. The lme4 package for R was used for this analysis.
Results
Mean age of patients was 30.4±4.2 years (range, 25–37 years). Mean duration of diabetes was 14.6±7.6 years. Two patients had a body mass index of >30 kg/m2, with the mean value in the whole group being 28.1±3.8 kg/m2. Gestational week at evaluation was 33.5±1.0 (range, 32–36) (Table 1). No adverse events during the CGM/ECG recordings were noted in any of the studied patients. The mean number of paired data points per patient was 254±106, representing an observation period of 21.2±8.8 h. The mean glucose level equaled 5.64±0.68 mmol/L, and the mean FHR was 135±6 bpm.
Individual data of all 14 participants are presented in the respective rows. Means with SDs are presented in the last row.
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; MDI, multiple daily injections; T1DM, type 1 diabetes mellitus.
Glycemic variability data and FHR characteristics are summarized in Table 2. In nine patients FHR showed significant, positive correlation with the time-point-matched maternal glycemia, which consequently held true for an aggregate correlation analysis (R=0.32; P<0.0001) (Fig. 1). In five patients no such correlations were noted, and in one case a significant negative correlation was noted. In mixed-effect logistic regression analysis, higher glucose levels were associated with higher odds of the fetus developing small accelerations (odds ratio=1.05; 95% confidence interval, 1.00–1.10; P=0.04). None of the analyzed individual-level factors, like patient's age (P=0.38), body mass index (P=0.66), duration of diabetes (P=0.32), gestational week (P=0.93), or nighttime measurements (P=0.07), significantly affected the association between maternal glucose and FHR accelerations. The risk of small decelerations did not, however, depend significantly on current maternal glucose levels (odds ratio=0.97; 95% confidence interval, 0.92–1.03; P=0.32), with nighttime measurements significantly decreasing the odds of deceleration events (odds ratio=0.49; 95% confidence interval, 0.41–0.58; P<0.0001). Similarly, with acceleration events, none of the evaluated individual factors—patient's age (P=0.51), body mass index (P=0.56), duration of diabetes (P=0.83), or gestational week (P=0.35)—showed any associations with the odds of deceleration events.
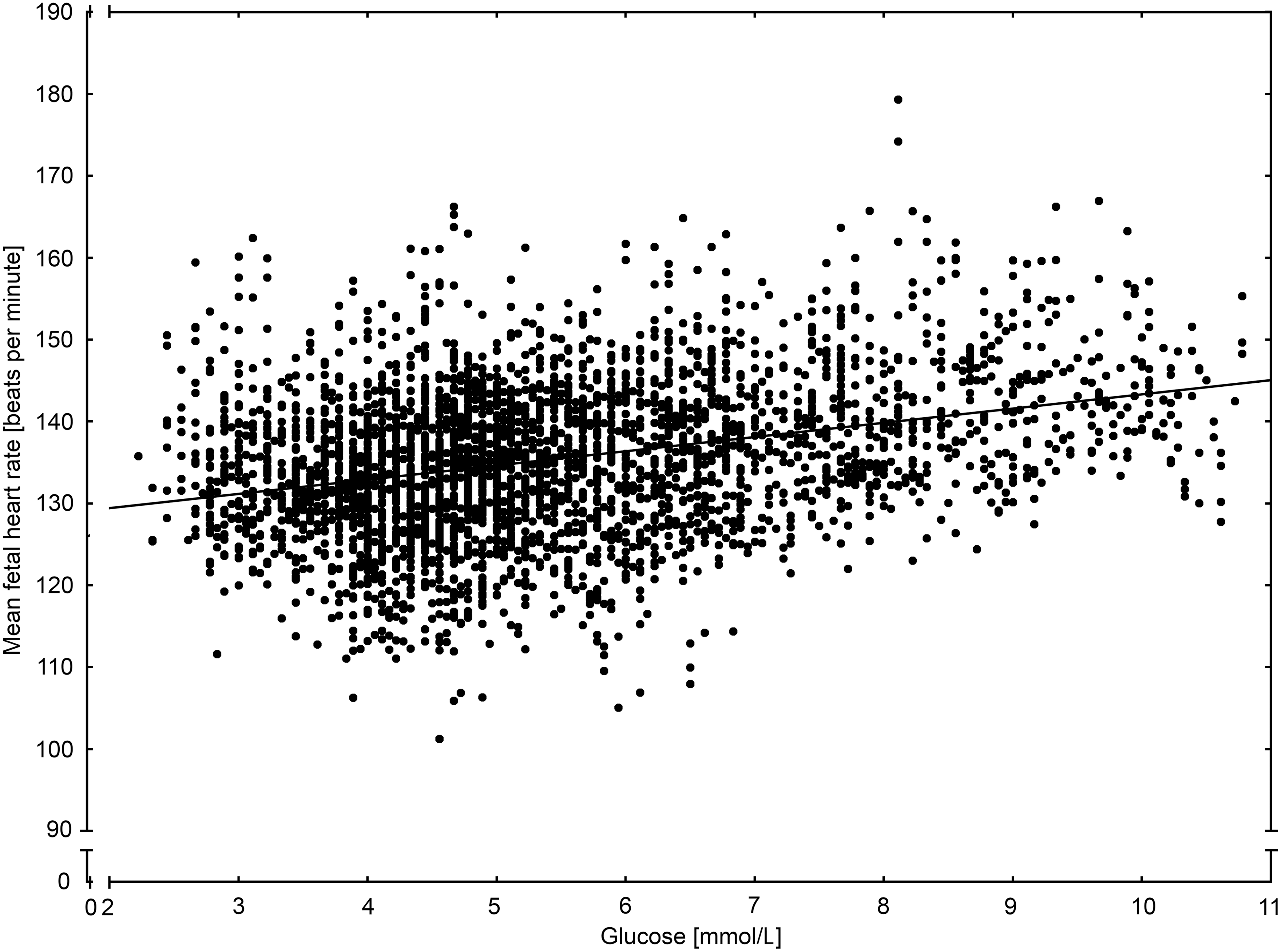
Correlation between the time-point-matched maternal glycemia and fetal heart rate for pooled data points of all available patients/recordings.
P<0.0001, b P<0.05.
bpm, beats/min; FHR, fetal heart rate; NA, not applicable; R, Pearson's correlation coefficient.
In our study we did not observe any large, long-lasting deceleration, the most dangerous heart disturbance, probably because diabetes control achieved in the studied patients was excellent. The mean HbA1c was 5.95±0.48%, and glycemia during the observation ranged from 2.22 to 10.78 mmol/L.
Discussion
Adequate metabolic control of diabetes in pregnant women is a crucial method of preventing neonatal and obstetric complications. Hyperglycemia in pregnant women can cause fetal malformations, growth disturbances, development delay of the central nervous system, chronic hypoxemia, and, finally, spontaneous abortion, stillbirth, prematurity, and many other fetal complications, including hypoglycemia, macrosomy, etc. Those are well documented in the in vitro and in human studies. 1 –5
A Swedish study proved that stillbirth rate in women with type 1 diabetes was more than three times higher than in the background population. 6 Cardiotocography (fetal ECG) is an established method to monitor fetal well-being and is essential to avoid intrauterine death by early detection of fetal compromise. Björklund et al. 12 revealed that maternal hypoglycemia induced during hyperinsulinemic/hypoglycemic clamp with induction and maintenance of an arterial blood glucose level of about 2.2 mmol/L was associated with an increase in frequency and amplitude of FHR accelerations and a slight decrease in the pulsatility index of the umbilical artery and with a rise in the maternal catecholamine levels. However, Reece et al. 13 did not observe an influence of maternal hypoglycemia in pregnant women with diabetes on the mean number of fetal limb, body, and breathing movements or a heart rate, although maternal epinephrine and growth hormone levels were significantly increased.
In a study by Serra-Serra et al. 14 the impact of maternal blood glucose concentration on cardiotocographic results in pre- and postmeal stage was measured. The authors concluded that FHR parameters are unaffected by prandial glycemic changes over a wide range (4.2–14.8 mmol/L) of maternal glucose levels in any of the groups of women with gestational diabetes, pregestational diabetes, and healthy pregnant volunteers without diabetes. 14
On the other hand, Buscicchio et al. 15 showed that gestational diabetes did impact FHR. The alteration was slight but evident, and it correlated with neonatal reactivity. 15 Unfortunately, in this study the blood glucose level was measured only once, at delivery.
Wiener et al. 16 revealed significantly reduced FHR variation as well as frequency of accelerations in fetuses of woment with well-controlled diabetes compared with fetuses of mothers without diabetes. In this study, published in 1996, HbA1c was only estimated every 3 months during pregnancy, self-monitoring of glucose was performed, and there were no data about blood glucose concentration during the test.
Costa et al. 17 also found a positive correlation between basal FHR and mean glycemia. A significant negative correlation was observed in this study between short-term variation and mean glycemia.
All these studies did not combine directly maternal blood glucose concentration with fetal ECG data. Our study seems to confirm direct relationship between maternal glycemia and fetal well-being as it demonstrates that elevated maternal glycemia of mothers with diabetes is associated with accelerations of FHR, even in very well-controlled diabetes. We are aware that the study does have its limitations due to a single time point of CGM/ECG examination, a lack of a healthy control group, and limited sample size. It would be, however, extremely difficult to justify such an experiment on healthy pregnant women without any a priori reason to conduct a cumbersome CGM examination. Moreover, the dynamic range of glycemic changes in healthy women is incomparably narrower than that observed in women with diabetes. This ultimately convinced us that if any meaningful associations between GCM and ECG variability are to be discovered, it should be done first in a group in which fluctuations of both heart rate and glycemia may have direct consequences. Finally, having established that FHR does correlate with maternal glycemia, we are able to focus on the impact of further inquiries on fetal outcomes of either parameter fluctuations.
This is the first study conducted in real life that shows this correlation in a continuous manner. We believe that investigation using a combined fetal ECG/maternal CGM is feasible and provides insight into impact of maternal diabetes on fetal well-being.
Conclusions
Elevated maternal glycemia of mothers with diabetes is associated with accelerations of FHR. Further studies are needed to explore the association between glucose variability of the mother and fetal well-being in various levels of glycemic control.
Footnotes
Acknowledgments
This study was supported financially by funds of the Medical University of Lodz (project number 502-03/0-160-01/502-04-014).
Author Disclosure Statement
No competing financial interests exist.