
Abstract
Background:
Liraglutide is a glucagon-like peptide-1 receptor analog recently approved for the treatment of type 2 diabetes mellitus (T2DM). We aimed to assess the efficacy and safety of liraglutide versus glimepiride, as adjunct treatments to metformin, in achieving glycemic control in Italian patients with T2DM uncontrolled by metformin alone.
Subjects and Methods:
One hundred seventy-nine diabetes patients treated with metformin plus liraglutide (1.8 mg) or glimepiride (4 mg) were retrospectively assessed at baseline, during, and after 18 months of continuous therapy.
Results:
Treatment with liraglutide resulted in mean decreases in hemoglobin A1c (HbA1c) of −1.4%, when compared with glimepiride (−0.4%) (P<0.001), and was followed by a significant reduction (P<0.001) in fasting plasma glucose. Variations in HbA1c occurred independently from weight loss, which was significantly reduced (P<0.001) in liraglutide-treated patients. The percentage of subjects reaching HbA1c levels below 7% or ≤6.5% was significantly different between the two treated groups (P<0.001). Treatment with liraglutide reduced waist circumference (WC) (P<0.001) and decreased both systolic and diastolic blood pressure (BP) (P<0.001). It is interesting that the study also showed the impact of female gender in predicting a better glycemic response to liraglutide (P=0.028).
Conclusions:
Liraglutide was more effective than glimepiride in reducing HbA1c levels in treated patients with T2DM. This was evident in both genders, but particularly in women. Furthermore, liraglutide reduced body weight, WC, and BP, which are critical risk factors for cardiovascular disease.
Introduction
T
The risk of developing diabetes increases as body mass index (BMI) increases. Consistent with this trend, the higher prevalence of obesity in Calabria, Southern Italy, parallels the greater proportion of individuals with T2DM in this area, compared with the entire Italian population (
Patients and Methods
Participants
Data were retrospectively collected from 76 diabetes patients who started treatment with liraglutide (in addition to metformin [2.31±0.47 g/day]) on the basis of current recommendations for management and treatment of hyperglycemia in T2DM. 8 Participants were recruited after the launch of liraglutide in Italy (September 2010) and until April 2012 from the diabetes outpatient clinic of the Hospital Pugliese-Ciaccio in Catanzaro (n=57), from the University of Catanzaro outpatient clinics (n=13), and from the diabetes outpatient clinic of Soverato (n=6). The following inclusion criteria were applied: 18–80 years of age, BMI ≤45 kg/m2, poor glycemic control (hemoglobin A1c [HbA1c] levels of >7% and <11%), receiving metformin therapy alone (≥1,500 mg/day) for a minimum of 3 months of treatment, and at least 18 months of continuous treatment with liraglutide (1.8 mg). Subjects were excluded if they had used insulin, a glucagon-like peptide-1 receptor agonist (exenatide or liraglutide), or any dipeptidyl peptidase-4 inhibitor during the previous 3-month period. In addition, we excluded patients who were pregnant or lactating, who had impaired hepatic or renal function, or who had clinically significant cardiovascular disease, cancer, or any contraindication to liraglutide therapy. One hundred three T2DM patients who were treated with 4 mg/day glimepiride plus metformin (2.29±0.46 g/day) were also retrospectively recruited from the same outpatient clinics, during the same time period. This latter population was selected according to the same criteria of inclusion and exclusion used for the liraglutide group.
Data collection was approved by the ethics committee of the Azienda Ospedaliera “Mater Domini” in Catanzaro and the ethics committee at the Hospital Pugliese-Ciaccio in Catanzaro. As the data were analyzed anonymously, there was no need for written informed consent. Study was performed in accordance with the Declaration of Helsinki.
Assessments
All patients performed self-monitoring of capillary blood glucose at scheduled intervals during the study period (preprandial and 2-h postprandial measurements) and underwent periodical clinical and biochemical evaluations to monitor efficacy and safety of therapy. The variables analyzed to assess efficacy included HbA1c, fasting plasma glucose (FPG), self-measured FPG, weight, waist circumference (WC), fasting lipid profile, and BP. Safety variables included hypoglycemic episodes, physical examination, and biochemical analyses. Patients recorded any medical problems on diary cards, including possible adverse events, and the entries were reviewed at each study visit.
Outcomes
The primary efficacy outcome measure was the change from baseline in HbA1c after 18 months of treatment. The secondary outcome measures included changes in body weight, BP, WC, FPG, lipid profile, aspartate aminotransferase and alanine aminotransferase enzyme activities, proportion of participants achieving HbA1c level <7.0% or ≤6.5%, and the percentage of subjects reaching the composite end point of HbA1c <7.0% with reduced systolic BP ≥10 mm Hg, no weight gain, and no hypoglycemic events. In addition, we searched for potential baseline predictors of better response to therapy.
Statistical analyses
Initially, each quantitative trait was tested for normality of distribution, using the Shapiro–Wilk normality test. Continuous variables were expressed as medians and interquartile range, and categorical variables were expressed as numbers and percentages. The nonparametric Wilcoxon signed-rank test was used for within-group differences. The two-tailed Fisher's exact test was used for comparisons of proportions, whereas the Mann–Whitney test was used for comparisons of continuous variables between two groups. Each significant change was examined using analysis of covariance, including the appropriate covariates and treatment as fixed effect. Before this analysis, all examined variables have been transformed to better approximate a normal distribution. To identify quantitative determinants of liraglutide efficacy, all variables were tested in multivariate linear regression analysis, where appropriate covariates were added. A significance level of 0.05 was set for all analyses.
Results
Clinical and biochemical baseline characteristics of the study population
In total, 179 patients completed 18 months of treatment with either liraglutide or glimepiride as add-on therapy to metformin. Clinical and biochemical characteristics, summarized by treatment group in Table 1, were adequately balanced.
Data are median (interquartile range) values or number (%) as indicated. The nonparametric Mann–Whitney test was used for comparisons of continuous variables. The two-tailed Fisher's exact test was used for proportion comparisons between groups. Significance level was set as <0.05.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BP, blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein-cholesterol; WC, waist circumference.
Glycemic efficacy
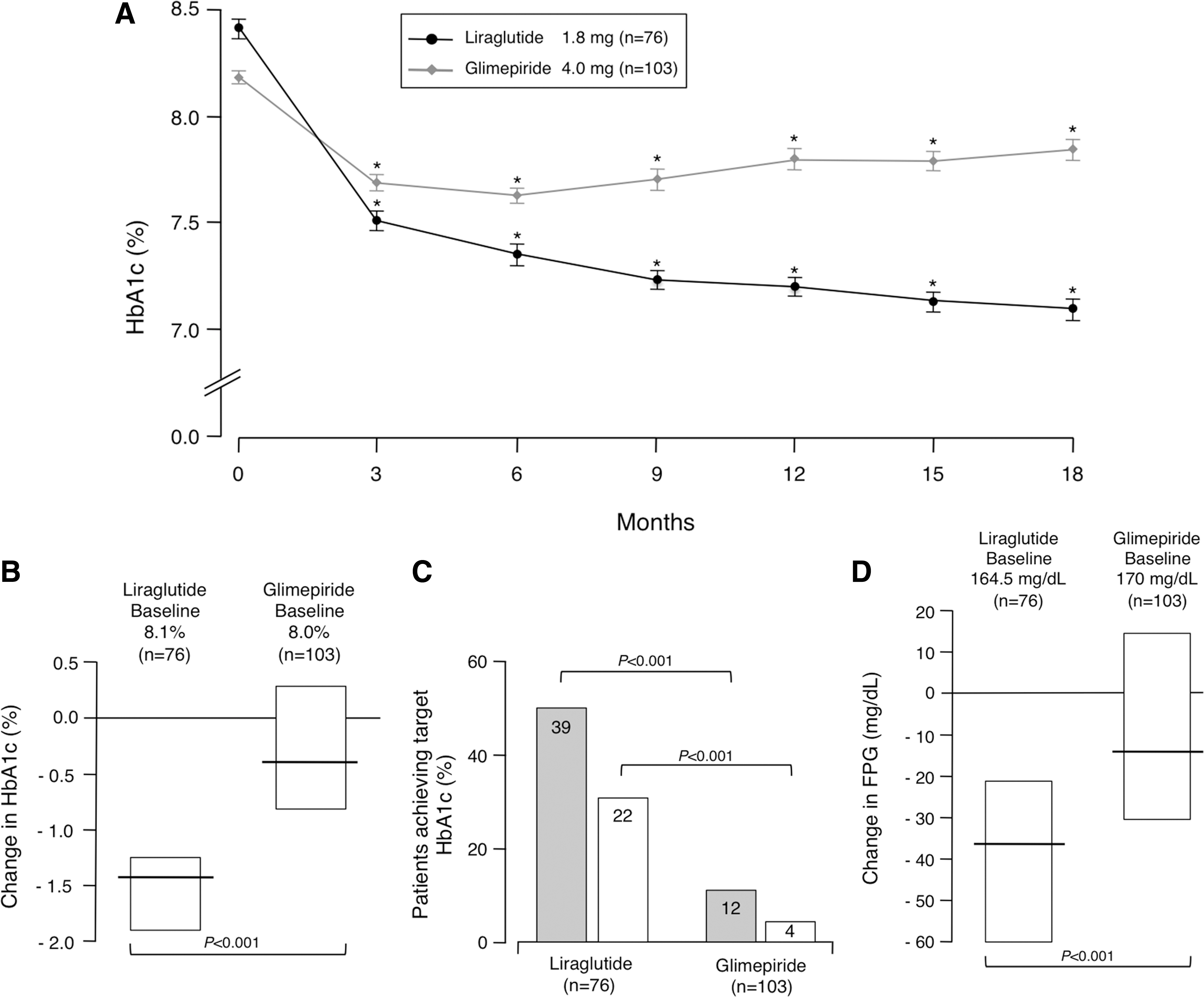
A significant reduction of HbA1c was observed during and after 18 months of treatment in both groups of patients (Fig. 1A). The decrement was more pronounced during the first 3 months for both groups, whereas it was attenuated later in the liraglutide group. Instead, a subsequent trend toward an increase in HbA1c levels was shown in the glimepiride group (Fig. 1A). Overall, HbA1c decreased from 8.1% (7.6–8.8%) to 6.9% (6.3–7.7%) in the liraglutide group (P<0.001) and from 8.0% (7.7–8.5%) to 7.9% (7.2–8.4%) (P<0.001) in the glimepiride group. Differences in HbA1c levels from randomization to the end point were −1.4% (−1.8 to −0.7%) in the liraglutide group and −0.4% (−1.5 to 0.8%) in the glimepiride group (Fig. 1B). As measured with the Mann–Whitney test, the difference between the two groups was statistically significant (P<0.001), even after inclusion of the baseline value as covariate (P<0.001) (Table 2), and this significance was also maintained after adjustment for reduction of body weight (Table 2). As shown in Figure 1C, the proportion of patients reaching the American Diabetes Association target for glycemic control (HbA1c <7%) in the liraglutide group (51.3%) was significantly higher compared with the glimepiride group (11.6%) (P<0.001). Similar results were obtained when an HbA1c cutoff of 6.5% (American Association of Clinical Endocrinologists' target for glycemic control) was considered (Fig. 1C).
Glycemic efficacy.
Data are median (interquartile range) values. Significance level was set as <0.05.
The nonparametric Mann–Whitney test was used for comparisons among the two groups.
Analysis of covariance including each change as dependent variable and treatment as fixed effect with the following covariates: aage, duration of diabetes, body mass index, and baseline hemoglobin A1c (HbA1c); bage, duration of diabetes, body mass index, baseline HbA1c, and change in body weight; cage, duration of diabetes, body mass index, and baseline fasting plasma glucose (FPG); dage, duration of diabetes, body mass index, baseline FPG, and change in body weight; eage, duration of diabetes, and baseline weight; fage, duration of diabetes, body mass index, and baseline waist circumference (WC); gage, duration of diabetes, body mass index, baseline WC, and change in body weight; hage, duration of diabetes, body mass index, anthypertensive treatment, and baseline blood pressure (BP); and iage, duration of diabetes, body mass index, anthypertensive treatment, baseline BP, and change in body weight.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; HDL-C, high-density lipoprotein-cholesterol.
Similarly, levels of FPG decreased from 164.5 mg/dL (156–188 mg/dL) to 135.5 mg/dL (121–147 mg/dL) with liraglutide (P<0.001) and from 170 mg/dL (150–196 mg/dL) to 160 mg/dL (134–180 mg/dL) with glimepiride (P=0.002). As shown in Figure 1D and Table 2, comparison of these changes among study groups showed a significantly greater efficacy of liraglutide versus glimepiride (P<0.001), even after inclusion of the FPG baseline value as covariate, and was maintained after adjustment for reduction of body weight (Table 2).
Secondary outcomes
At the end of the study, significant body weight loss was observed in the liraglutide-treated group: from 73.5 kg (68.0–89.3 kg) to 70.0 kg (64.0–83.5 kg) (P<0.001). No weight change occurred in the glimepiride-treated group: from 75.0 kg (67.0–85.0 kg) to 75.0 kg (67.0–85.0 kg). Change in body weight in the liraglutide group was significantly greater than in the glimepiride-treated group (P<0.001), even after inclusion of the baseline body weight value as covariate (Table 2). Also, the percentage of patients achieving weight loss of ≥5% at the end of the study was significantly higher in the liraglutide group (21%) compared with the glimepiride group (only 1.0%) (P<0.001). Consistent with these results, WC decreased from 100.0 cm (95.3–106.0 cm) to 98.5 cm (92.0–104.0 cm) in the liraglutide group (P<0.001), whereas no change occurred in the glimepiride group (from 101.0 cm [95.0–106.0 cm] to 102.0 cm [95.0–106.0 cm]). As expected, decreased WC was related to reduction in body weight (Table 2).
Concerning BP, systolic BP diminished from 135 mm Hg (130–140 mm Hg) to 125 mm Hg (120–130 mm Hg) in the liraglutide group (P<0.001), whereas no difference was observed in the glimepiride group: from 135 mm Hg (125–145 mm Hg) to 135 mm Hg (130–140 mm Hg). Similar results were observed with diastolic BP, which decreased from 80 mm Hg (80–85 mm Hg) to 80 mm Hg (75–80 mm Hg in the liraglutide group (P<0.001) but was unchanged in the glimepiride group: from 80 mm Hg (75–80 mm Hg) to 80 mm Hg (75–85 mm Hg). The reduction of both systolic and diastolic BP in the liraglutide-treated group was significantly greater than in the glimepiride group (P<0.001 and P=0.006, respectively) (Table 2). These results were confirmed by analysis of covariance, after adjustment for body weight loss, except for the diastolic BP reduction, for which statistical significance was not confirmed (Table 2).
Also, in each treated group a significant reduction in total cholesterol was observed with respect to their basal values (P<0.001 for the liraglutide group and P=0.004 for the glimepiride group). No other significant intra- and intergroup differences were found regarding serum lipid profile and liver enzymes (Table 2).
Finally, a composite end point (including HbA1c <7.0%, reduced systolic BP ≥10 mm Hg, no weight gain, and no hypoglycemic events) was adopted. This end point was achieved in 34.2% of patients receiving liraglutide versus 1.9% of patients receiving glimepiride (P<0.001), thus supporting the greater efficacy of liraglutide in comparison with glimepiride.
Baseline determinants of liraglutide efficacy
In an attempt to identify the baseline determinants of liraglutide efficacy, a multivariate linear regression analysis was performed after normalization of continuous variables. Levels of baseline HbA1c and FPG appeared to be independent predictors of change in HbA1c (unstandardized coefficient B=−2.203, P<0.001) and FPG (B=−1.85, P<0.001), respectively, after adjustment for age, duration of diabetes, and BMI. Similarly, baseline systolic BP was the only predictor of change in systolic BP (B=−1.993, P=0.002), and diastolic BP was the only predictor for change in diastolic BP (B=−2.272, P<0.001), after adjustment for age, duration of diabetes, BMI, and antihypertensive treatment. Addition of change in body weight as a further covariate did not alter the significance of the results, thus indicating that glycemic efficacy of liraglutide and its effect on BP were independent from weight reduction. Also, baseline weight was the only predictor of change in body weight (B=−1.308, P<0.001). It is interesting that females of the liraglutide group had a significantly stronger reduction in HbA1c level than males (−1.5 [−1.925, −1.2] versus −0.75 [−1.525, −0.375]), showing an impact of female gender in predicting a better glycemic response to liraglutide, even after adjustment for age, duration of diabetes, and BMI (B=0.243, P=0.028). There was no female impact on body weight, WC, and BP.
Safety
Treatment with liraglutide and glimepiride was well tolerated, and the majority of adverse events during the 18-month period were mild to moderate and comparable among the two treated groups, except for hypoglycemic events, which were more common in the glimepiride group, and gastrointestinal disorders, which were more frequent in the liraglutide group (Table 3). Although hypoglycemia occurred at low incidence (2.6%) in the liraglutide group, it was experienced by 22 individuals (21.4%) of the glimepiride group. In contrast, among individuals who reported gastrointestinal-related symptoms during the course of the study, 53.9% were patients in the liraglutide group, and 10.7% were in the glimepiride group (P<0.001) (Table 3). The majority of gastrointestinal disorders were experienced in the first weeks of the treatment, with 41 subjects reporting gastrointestinal side effects in the first 4 weeks of therapy and 6 in the last 4 weeks. No patients dropped out of each group because of persistent gastrointestinal events. No differences were seen between the two studied groups in clinical examination (including the pulse rate) or in biochemical parameters (including serum calcitonin levels). No pancreatic abnormalities were detected over the 18-month observation period, either clinically or biochemically (through amylase and lipase detection results).
Data are number (%). Each patient could experience more than one adverse event.
Discussion
The results of the current study demonstrate that treatment of T2DM patients with liraglutide (1.8 mg/once daily) in combination with metformin provides improvement in HbA1c and FPG superior to that of combination therapy of glimepiride and metformin following a 18-month period of treatment. Both baseline HbA1c and FPG were the main determinants of the decrease of HbA1c and FPG levels in patients treated with liraglutide, in which, as reported by others, 9,10 improvement in glycemic control was independent from baseline BMI or from diabetes duration and independent from other clinical and biochemical features. This finding may have important clinical implications, as it suggests that treatment with liraglutide can be initiated in diabetes patients independently from their baseline BMI and that overweight/obese patients could be treated with liraglutide independently from HbA1c.
It is interesting that, for the first time, we show the impact of female gender in predicting a better glycemic control in patients treated with liraglutide. Given that no similar observation was reported previously, in similar studies, it is reasonable to hypothesize that differences between Calabrian women and those of other populations in liraglutide therapy may be due to differences in the genetic background and/or environmental exposures of the enrolled subjects. In this respect, Calabria, Southern Italy, is often given as an example of a genetically homogeneous population that differs from other populations with more genetic diversity. 11,12 Although further studies with different populations and larger sample size would be useful to corroborate this observation, our findings that gender may moderate responses to liraglutide (and perhaps other pharmacological agents) are in line with existing studies revealing several differences between women and men with diabetes and other diseases. 13
Weight loss in the liraglutide group and the parallel decrease of WC that we observed are consistent with other reports 5 and with the demonstration that weight loss with liraglutide is primarily as a result of a reduction in fat tissue. 14 Although weight gain is frequent among patients taking glimepiride, 15 no significant weight changes were observed in our study in glimepiride-treated patients, reflecting previous observations in an Asian population with T2DM. 16 In this context, the efficacy of liraglutide on lipid profile is well documented, 17 whereas inconsistent data exist about the efficay of glimepiride. 18 –20 Our data in the present study indicate that both drugs cause a significant reduction in total blood cholesterol levels, whereas they show no effects on other lipid parameters. Also, the results indicate that liraglutide causes a significant decrease in systolic and diastolic BP, which is consistent with previous results. 21,22 However, whereas improvement in systolic BP was associated with its baseline value and cannot be explained by weight loss alone, the reduction of diastolic BP was associated with baseline BP and was dependent on body weight reduction.
With regard to safety issues, the incidence of gastrointestinal events in our population was higher in the liraglutide-treated group. However, the occurrence of gastrointestinal disturbances was dose dependent and temporary, typically occurring only during the first week of treatment, confirming that in clinical practice slow up-titration of liraglutide during the first week of therapy may minimize gastrointestinal side effects. 23 Also, the risk of hypoglycemic events was low with this therapy, thus indicating that treatment with liraglutide is generally well tolerated and safe.
Although study groups were balanced with respect to the baseline variables that were measured and the patients were similarly assessed during the follow-up period, to minimize potential interfering factors (i.e., adherence to diet, exercise regimen, and taking medications as prescribed), as a retrospective study, however, we cannot completely rule out the limitations associated with this type of study design, and the strength of our conclusions is somewhat limited. Nevertheless, our findings on the efficacy of liraglutide in relation to glycemic control, BP, and weight loss are in line with those of previous prospective studies, 15,16,24 –28 in which liraglutide was estimated to be a highly cost-effective option for treating inadequately controlled T2DM on oral hypoglycemic agents. 29
Conclusions
The effects of liraglutide in Calabrian patients were comparable with or even better than those of other similar population-based studies, 15,16,24 –28 indicating that the combination treatment of liraglutide plus metformin may provide a superior therapeutic efficacy in T2DM compared with glimepiride plus metformin. In line with the American Diabetes Association's latest Standards of Care, for which diabetes treatment needs to move beyond a glucocentric strategy that not solely focuses on controlling glucose homeostasis disturbance, but also addresses other comorbidities commonly associated with T2DM (i.e., obesity, hypertension, and dyslipidemia), 8 our data confirm and extend the results of earlier studies, indicating that liraglutide may offer a relevant approach to managing T2DM and related morbidities, although its cost is still elevated.
Footnotes
Acknowledgments
We thank the staff of the Diabetes Unit of the Azienda Ospedaliera Pugliese-Ciaccio of Catanzaro, Italy, particularly Mrs. M. Zangari, Mrs. C. Lombardo, Mrs. T. Marghella, Mr. V. Cristofaro, and Mrs. G. Procopio, for their helpful assistance in the recruitment and examination of patients. Also, we would like to thank Prof. Massimo Borelli (Department of Mathematical Sciences, University of Trieste, Trieste, Italy) for statistical revision of the manuscript.
Author Disclosure Statement
No competing financial interests exist.