
Abstract
Background:
The aim of this study is to compare the effectiveness of different models of structured self-monitoring of blood glucose (SMBG) in non–insulin-treated type 2 diabetes.
Subjects and Methods:
This was a prospective, three-arm, randomized, 36-week trial. There were 138 participants with a mean age of 58.7 years and glycated hemoglobin A1c (HbA1c) level of 8.72% who were allocated to the following groups: six-pair glucose test of pre- and postprandial blood glucose (BG) per week (n = 43); three-pair glucose test of pre- and postprandial BG per week (n = 39); and seven-point BG testing before and after each meal and at bedtime over a course of 3 days in 1 month (n = 40).
Results:
The intention-to-treat analysis revealed that all three groups showed significant reductions in HbA1c levels. Comparisons among the groups revealed that only the seven-point group had a significant greater reduction of HbA1c level compared with the three-pair group (between-group mean difference of −0.86 and −0.80 from baseline to 24 and 36 weeks, respectively). No severe hypoglycemic events were reported. Diabetes distress was slightly higher in the six-pair group.
Conclusions:
Our results demonstrated that BG testing at six pairs/week, three pairs/week, and seven points for 3 days/month were all effective in improving glycemic outcome, with greater reduction of HbA1c level in the seven-point for 3 days/month group, without increasing burdensome distress in SMBG.
Introduction
S
The International Diabetes Federation recommends that SMBG should be used only when patients and/or their clinicians “have the knowledge, skills and willingness to incorporate SMBG monitoring and therapy adjustment into their diabetes care plan in order to attain agreed treatment goals.” 1 A key component of the International Diabetes Federation guidelines is the recommendation that structured SMBG be performed initially and periodically in order to obtain glucose information from blood glucose (BG) profiles. Structured algorithms, such as preprandial and postprandial SMBG on consecutive or alternating days (“testing in pairs”), or profiles that are representative of daily glucose excursions can provide impactful glucose information for daily diabetes management.
The benefits of SMBG have been demonstrated in type 1 diabetes mellitus 3 and insulin-treated type 2 diabetes mellitus, 4 –6 but findings from SMBG studies in non–insulin-treated type 2 diabetes 7 –11 have been inconsistent. These contradictions are due mainly to differences in trial study designs, outcome indicators, populations studied, and inherent limitations of the randomized controlled trial models used. Some important limitations of these randomized controlled trials resulted from inadequate collection of glucose information through random BG testing or lack of use of the glucose information collected. 1 The most significant issues of concern, however, are the testing regimens (structure, intensity, and/or frequency) engaged and how the SMBG data were utilized. Therefore the aim of this study was to compare different models of structured SMBG in non–insulin-treated type 2 diabetes.
Research Design and Methods
This was a prospective, three-arm, randomized, 36-week trial that compared the effectiveness of different models of structured SMBG. One-hundred thirty-eight patients with non–insulin-treated type 2 diabetes were recruited from a diabetes outpatient clinic of a tertiary hospital center.
Inclusion criteria were as follows: age ≥20 years; glycated hemoglobin A1c (HbA1c) level between 7.0% and 12.0%; currently treated by diet, exercise, and oral diabetes medication (at least two oral antidiabetes drugs at submaximal dose); able to read and write Chinese; had not previously applied SMBG; and had not participated in any other research protocol within the last 30 days.
Exclusion criteria were as follows: managed with insulin at the start of study; treated with chemotherapy or radiation therapy; pregnant or breastfeeding; had severe depression, other severe psychological condition, psychosis, or recent emotional trauma; or had dementia.
Eligible participants were reviewed by the physicians, referred to a diabetes educator, and then randomly assigned to an intervention group. This study protocol was approved by the Institutional Review Board (protocol number CS-12189). This study was conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines. Written informed consent was obtained from all participants.
Intervention
The three groups consisted of a seven-point profile (fasting, preprandial and 2-h postprandial testing at each meal and at bedtime) on 3 consecutive days every month; intensive “staggered” SMBG regimen, six-pair profile (two consecutive preprandial and 2-h postprandial testing for each meals over the course of a week); and “meal-based” SMBG, three-pair profile (three consecutive preprandial and 2-h postprandial testing over the course of a week). Figure 1 presents the testing protocols of this study.
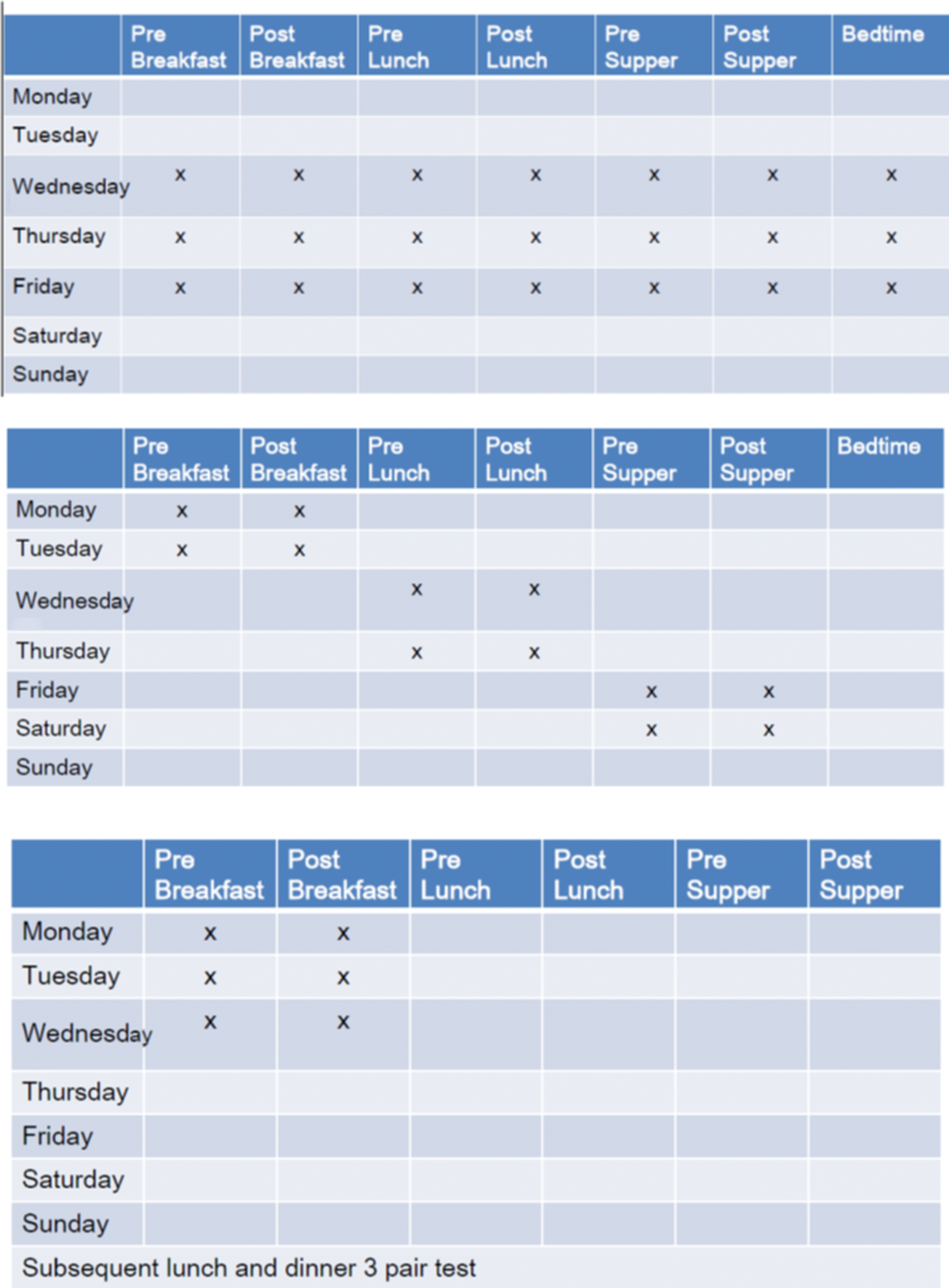
Testing regimens of this study:
All participants were given a new glucose meter and 4 weeks of test strips at Visit 0 (baseline). A further 8 weeks' worth of test strips were also provided at Visit 1. BG meter results were downloaded, or recorded in logbooks, and study diaries were reviewed at Visit 1 (4 weeks) and Visit 3 (12 weeks). Blood samples were collected at visits at 12, 24, and 36 weeks. All participants received diabetes education concerning the value and utility of SMBG testing and options for self-management action based on SMBG results, which included adequate portion size, a comprehensive list of foods with their glycemic index, kinds of physical activity, and physical activity programs.
The physicians, who were all diabetologists, were allowed to change any treatment in any visit according to the patients' BG test results. Treatment change could include adding and further intensifying insulin, adding glucagon-like peptide-1 agonist, or adding or change to other oral antidiabetes agents. Treatment intensification was calculated using information entered into patient medical records at each clinic visit. These included recommended pharmacologic modification (defined as the initiation of a new medication, increase or decrease in the dose of an existing medication, or termination of an existing medication).
Outcomes
The primary end point was change in HbA1c from baseline to 36 weeks. Secondary end points were as follows: change of SMBG record results, fasting plasma glucose, and postprandial plasma glucose from baseline to 24 weeks; change of treatment; lifestyle modification (defined as any change in diet, exercise, or other self-care behavior); hypoglycemia events; and questionnaires that included the General Well-Being scale, Center for Epidemiologic Studies Depression scale, Problem Area In Diabetes, and the Perceived Diabetes Self-Management Scale. Change of treatment was calculated using information entered into the patient's medical records at each clinic visit. These included the initiation of a new medication, increase or decrease in the dose of an existing medication, or termination of an existing medication.
Statistical analysis
Sample size was estimated to be 37 in each group to detect a 0.3% change in HbA1c in 24 weeks with a power of 95%, α 0.05 two-tailed. The data were analyzed using SPSS software (version 17.0; SPSS, Inc., Chicago, IL). The analysis focus on the intention-to-treat population was defined as all participants who completed all blood tests but did not complete all the SMBG protocols (less than 75% adherence) in the first 3 months. The second analysis was a per-protocol population, which was defined as all participants who completed all blood tests and who had adherence of SMBG protocol of more than 75% in the first 3 months. Independent t tests were used to examine the baseline demographic data. Participant characteristics were compared to detect any difference among the three groups at baseline. Changes in the measurements between baseline and the follow-up visits were analyzed by paired t tests to examine the difference between before and after intervention for 24 weeks in the three groups. For between-group differences over time, a repeated-measures analysis of variance was conducted and controlled for within-subject correlation. All P values were two-tailed, and the level of significance was set at 0.05. Data were analyzed on a per-protocol basis, with participant exclusion occurring before release of the double-blind procedure.
Results
After the screening period, 122 participants were randomly assigned to the intervention groups. Of these, 43 participants were included in the six-pair/week SMBG group, 40 participants in the seven-point SMBG group, and 39 participants in the three-pair/week SMBG group (Fig. 2).
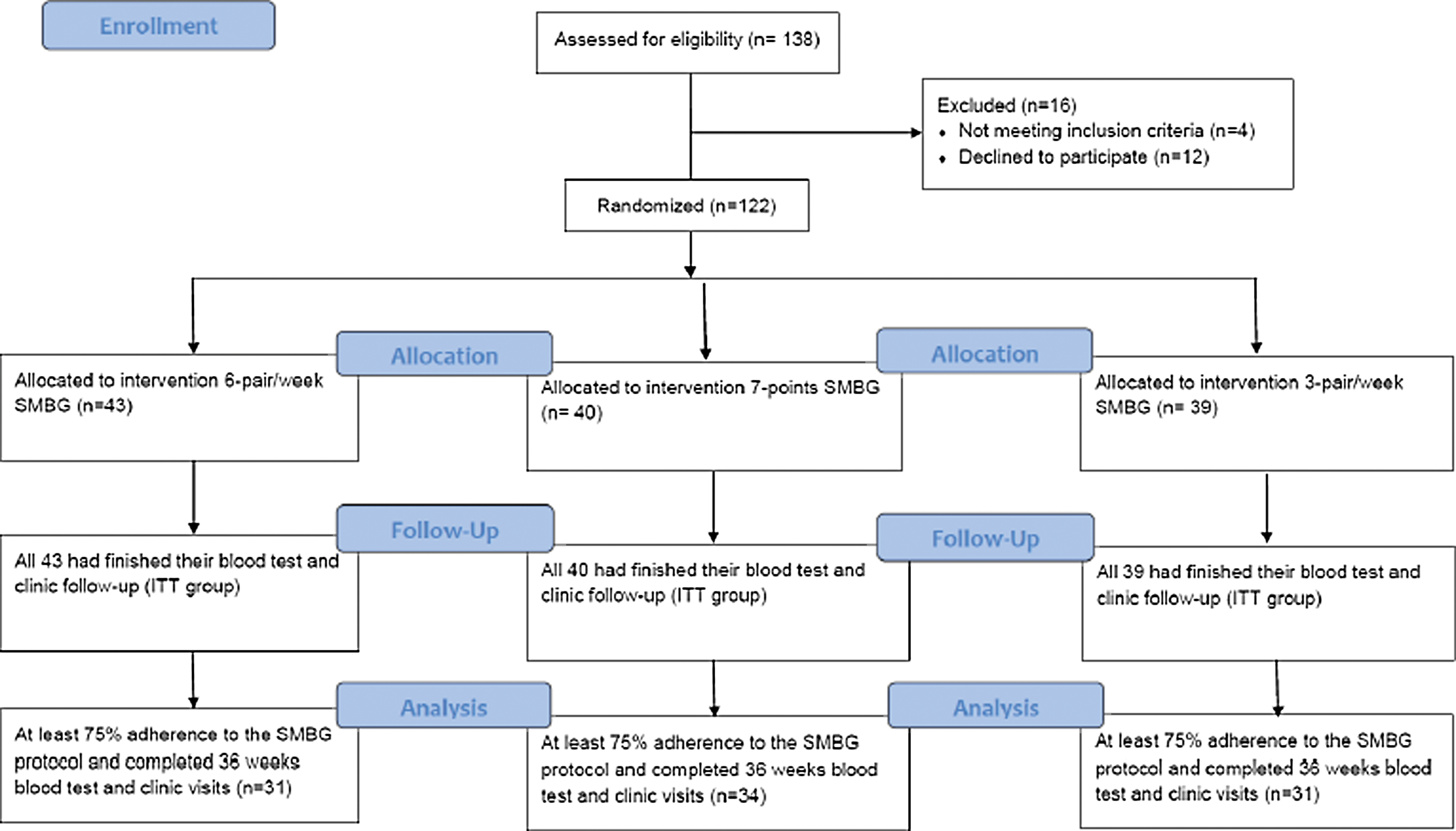
Flow diagram and allocation of the participants. ITT, intention-to-treat; SMBG, self-monitoring of blood glucose.
Patients' characteristics are summarized in Table 1. Patients' demographic and disease-related characteristics at baseline among the three study groups did not differ, and they also did not differ between the intention-to-treat and per-protocol groups.
Data are expressed as mean ± SD values or as number (percentage), as indicated. A value of P < 0.05 was considered statistically significant.
F, female; HbA1c, glycated hemoglobin A1c; FPG, fasting plasma glucose; M, male; PPG, postprandial plasma glucose.
The intention-to-treat analysis revealed that all three groups showed significant reductions in HbA1c levels. When comparing between groups, only the seven-point group showed a significantly greater reduction of HbA1c level compared with the three-pair group (between-group mean difference of −0.86 and −0.80 from baseline to 24 and 36 weeks, respectively) (Fig. 3A). The per-protocol analysis also revealed significant reductions in HbA1c levels in all three groups, with only the seven-point group showing a significant greater reduction of HbA1c level compared with the three-pair group (between-group mean difference of −0.68, −0.93, and −0.82 from baseline to 12, 24, and 36 weeks, respectively) (Fig. 3B).

Mean glycated hemoglobin A1c change from baseline to 36 weeks in the
Table 2 lists the baseline, follow-up, and mean changes in fasting plasma glucose, postprandial plasma glucose, and HbA1c values. The downloaded SMBG results of six- and seven-point BG profile findings are shown. All three groups showed significantly consistently lower average preprandial and 2-h postprandial glucose levels at all meals from baseline to 4, 12, and 24 weeks.
Data are expressed as mean ± SD values. A value of P < 0.05 was considered statistically significant.
P < 0.05 within group before and after intervention; b P < 0.05 when comparing the three groups.
FPG, fasting plasma glucose; HbA1c, glycated hemoglobin A1c; ITT, intention-to-treat; PP, per-protocol; PPG, postprandial plasma glucose.
Change of treatment was allowed at every follow-up visit. Treatment change included adding insulin, glucagon-like peptide-1 agonist, and adding or change to other oral antidiabetes agents. After 36 weeks, there was a change of 32.5%, 37%, and 23% in the seven-point, six-pair, and three-pair glucose testing groups, respectively (P = not significant). Over the 36 weeks of the study period, no intervention-related adverse events and no severe hypoglycemic events were reported. The incidence of hypoglycemia based on downloaded meter data was 2.5% in the seven-point SMBG group, 1.25% in the six-pair/week SMBG group, and 1.3% in the three-pair/week SMBG (P = not significant).
The results of prespecified secondary outcome measurements among the three groups all showed improved lifestyle modification factors, including decreased daily carbohydrate content and increased daily physical activity. There was no significant effect on Center for Epidemiologic Studies Depression and Perceived Diabetes Self-Management Scale scores. However, there was a trend of lesser magnitude of improvement in general well-being and Problem Area In Diabetes scores in the six-pair/week SMBG group, compared with the three-pair/week SMBG and seven-point SMBG groups (Fig. 4).
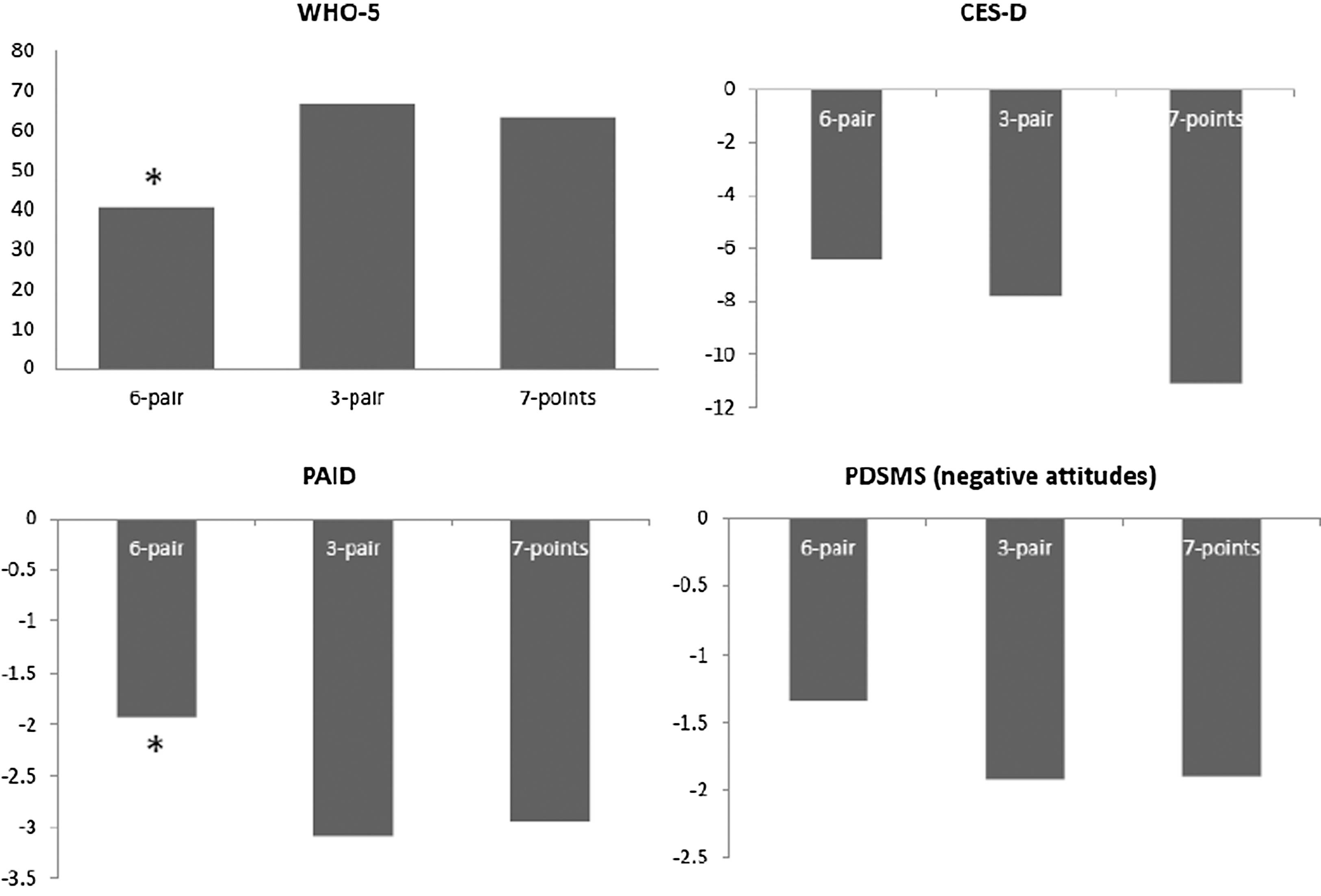
Psychosocial and attitudes outcomes changes from baseline to 3 months by general well-being (WHO-5), Problem Areas In Diabetes (PAID), Center for Epidemiologic Studies Depression (CES-D), and Perceived Diabetes Self-Management Scale (PDSMS) scores in the six-pair/week, three-pair/week, and seven-point self-monitoring of blood glucose regimen groups. *P < 0.05 for between-group comparison.
Discussion
We found in this randomized trial of three models of structured SMBG that all interventions contributed to a significant improvement in glycemic control in non–insulin-treated type 2 diabetes patients, with particular improvements with two or three combined oral antidiabetes agents on submaximal dose.
There was a greater likelihood of improvement in the seven-point group compared with the three-pair structured SMBG method; however, there were no significant differences between the three- and six-pair groups, as well as the seven-point and six-pair groups. Outcomes that improved significantly included glycemic improvement and positive attitudes toward diabetes care. However, in terms of burden of SMBG, the six-pair group tended to have less improvement in scores of general well-being and Problem Areas In Diabetes.
Our results were consistent with those of previous studies, which showed a positive effect of a structured SMBG in type 2 diabetes. However, there was an even greater impact in our study compared with previous findings, with an average HbA1c reduction of 0.7–1.7%. This result could be explained by several factors. First, this was a group that received a submaximal dose of oral antidiabetes agent, who possibly refused further insulin injection therapy, and could therefore put greater effort into lifestyle changes according to their glucose meter results. Second, the results downloaded from the glucose meter at clinic visits could have resulted in timely treatment changes and even a greater acceptability of injection therapy, accounting for about a 30% treatment change over the study period.
Individuals who are treated with diet, exercise, and/or oral antidiabetes medications may not require daily SMBG; pre- and postprandial testing 2–3 days each week may be sufficient in some cases. However, it is valuable for all patients to perform intensive SMBG periodically to create datasets that facilitate identification of glucose patterns that are reflective of daily glycemic control. 12 For example, patients may use a seven-point SMBG regimen, testing before and after each meal and at bedtime, over the course of 3–7 days. Or, patients may use a “staggered” regimen, testing before and after alternating meals (e.g., pre- and postbreakfast on Monday, pre- and postlunch on Tuesday, etc.), over a 2–3-week period. 13,14 By staggering SMBG measurements at different times on different days, patients can generate an accurate portrait of day-to-day glycemic excursions while avoiding the need to test many times in a single day. 15 There are several situations in which intensive, episodic (short-term) SMBG can be beneficial in this patient group. These situations include times when patients have symptoms of hypoglycemia, are undergoing adjustment in medication, nutrition, and/or physical activity, or experience worsening HbA1c values. In this study, in particular, patients who experienced persistent worsening HbA1c values were instructed to conduct intensive monitoring as a means to obtain comprehensive preprandial and 2-h postprandial glucose measurements periodically and to test before clinician visits to guide adjustments in diabetes management.
The seven-point protocol showed superior effects compared with the three-pair group but did not differ from the results of the six-pair group. We did not analyze actual cost-effectiveness, but judging solely by the number of test strips used, the seven-point group used 21 strips/month, the three-pair group used 24 strips/month, and the six-pair group used 42 strips/month. Thus it is reasonable to postulate that the seven-point group yielded a more cost-effective result in terms of the similar degree of glycemic outcome obtained and the lower burden of SMBG.
Greater improvements in HbA1c levels over time after receiving structured SMBG were associated with less SMBG frequency. 16 This finding has important policy implications, suggesting that it may be appropriate to shift the current focus from SMBG quantity (testing frequency) to SMBG quality (meaningful test results that contribute to positive action), using protocols that place more emphasis on when patients test and how they and their physicians organize and make clinically relevant use of the resulting data.
Many studies have demonstrated a benefit of SMBG, but sometimes it was associated with a slightly higher score on the depression subscale or a lower quality of life. In the DIGEM trial, a lower quality of life was reported in those receiving SMBG among relatively well-controlled non–insulin-treated patients. 7 In contrast, there were no changes in diabetes-specific quality of life scores, indicating no deterioration in quality of life with structured SMBG in non–insulin-treated patients with type 2 diabetes. 17 Patients with reasonably well-controlled diabetes do not need active encouragement to use a meter. In our study, scores of general well-being, Problems Areas In Diabetes, and depression all improved after 36 weeks. Utilization of treatment strategies in addition to medications, including structured SMBG, appears to help patients achieve their glycemic goals and improve clinical outcomes as well as health-related quality of life. Improvements in self-behavior management and better healthy lifestyle modification may also enhance quality of life. However, there tended to less improvement in quality of life scores in the six-pair group compared with those seen in the seven-point and three-pair groups. Therefore increased frequency of SMBG might be beneficial in the management of type 2 diabetes, but sometimes patients may perceive it to be somewhat of a burden.
Strengths and limitations
Although there was a relatively small number of participants in this investigation, few studies have compared different models of structured SMBG. The participants were randomized independently. The intention-to-treat and per-protocol groups did not differ in baseline characteristics. Designing a trial to evaluate SMBG is complex because it must include an educational component on the use and interpretation of testing for the intervention group, and this may affect the outcomes. The treatment changes on oral antidiabetes drug were decided by the patient's physician, so we did not design a protocol to driven the standard treatment changes. Therefore we established a common structure for interventions, incorporating standardized care in all three groups of the trial within which diabetes educators and physicians discussed issues of glycemic control, assessed by either SMBG or HbA1c levels, and its role in setting and monitoring self-care goals. This may have created a more real-world clinical practice decision pathway.
In conclusion, the three models of structured SMBG appeared to be effective for treatment of patients who were on a submaximal dose of oral antidiabetes agent treatment and had suboptimal or worsening glycemic control. The seven-point testing group seemed to be more cost-effective and less burdensome compared with the three-pair and six-pair testing groups.
Footnotes
Acknowledgments
We thank all the patients, physicians, and diabetes educators who collaborated in the study. This study was supported by the Chung Shan Medical University Hospital (grant CSH-2014-A-004).
Author Disclosure Statement
No competing financial interests exist.