
Abstract
Background:
Carbohydrate counting may improve glycemic control in hospitalized cardiology patients by providing individualized insulin doses tailored to meal consumption. The purpose of this study was to compare glycemic outcomes with mealtime insulin dosed by carbohydrate counting versus fixed dosing in the inpatient setting.
Materials and Methods:
This single-center retrospective cohort study included 225 adult medical cardiology patients who received mealtime, basal, and correction-scale insulin concurrently for at least 72 h and up to 7 days in the interval March 1, 2010–November 7, 2013. Mealtime insulin was dosed by carbohydrate counting or with fixed doses determined prior to meal intake. An inpatient diabetes consult service was responsible for insulin management. Exclusion criteria included receipt of an insulin infusion. The primary end point compared mean daily postprandial glucose values, whereas secondary end points included comparison of preprandial glucose values and mean daily rates of hypoglycemia.
Results:
Mean postprandial glucose level on Day 7 was 204 and 183 mg/dL in the carbohydrate counting and fixed mealtime dose groups, respectively (unadjusted P=0.04, adjusted P=0.12). There were no statistical differences between groups on Days 2–6. Greater rates of preprandial hypoglycemia were observed in the carbohydrate counting cohort on Day 5 (8.6% vs. 1.5%, P=0.02), Day 6 (1.7% vs. 0%, P=0.01), and Day 7 (7.1% vs. 0%, P=0.008). No differences in postprandial hypoglycemia were seen.
Conclusions:
Mealtime insulin dosing by carbohydrate counting was associated with similar glycemic outcomes as fixed mealtime insulin dosing, except for a greater incidence of preprandial hypoglycemia. Additional comparative studies that include hospital outcomes are needed.
Introduction
H
Carbohydrate counting is a novel therapeutic approach to mealtime insulin dosing in the hospital setting despite its widespread outpatient use. When compared with fixed insulin dosing, carbohydrate counting demonstrated improved glycemic control in the outpatient setting in patients with type 1 diabetes 9 and similar glycemic control in patients with type 2 diabetes. 10 Reported glycemic outcomes with carbohydrate counting in the inpatient setting are limited to two investigations, and the results were mixed. 11,12 One study showed improved glycemic control with carbohydrate counting, but the comparator group received mealtime insulin dosed by a correction scale only. 11 Conversely, the second study demonstrated similar glycemic control after comparing carbohydrate counting with fixed mealtime insulin dosing. 12 Although the patients received basal and correction insulin in addition to mealtime, this study was not adequately powered and limited to 3 days of observation. Both studies included heterogeneous patient populations as well.
The purpose of this study was to compare carbohydrate counting with fixed mealtime insulin dosing for glycemic control outcomes in the inpatient setting when both are used in conjunction with basal and correction-scale insulin in a homogeneous patient population.
Materials and Methods
Subjects
This retrospective cohort study was conducted at a large academic medical center. To be eligible for inclusion, patients were at least 18 years of age, receiving care on a medical cardiology unit from 2010 to 2013, and receiving glycemic management by an inpatient diabetes consult service (DCS) consisting of physicians, nurse practitioners, and physician assistants who specialize in inpatient hyperglycemic management. Patients could be enrolled regardless of known diabetes history. Patients were also treated with mealtime, basal, and correction-scale insulin concurrently per national inpatient hyperglycemia management guidelines 6,7 for at least 72 h and up to 7 days while hospitalized. Mealtime and correction insulin was provided as a rapid-acting insulin analog, and basal insulin was provided as neutral protamine Hagedorn (NPH), glargine, or detemir and was dosed as ≥0.1 units/kg of actual body weight/day. Patients were divided into two groups based on whether their mealtime insulin was dosed using carbohydrate counting or fixed dosing. Choice of carbohydrate counting versus fixed dosing was based on the provider's discretion; therefore patients were not randomized. Exclusion criteria were receipt of an insulin infusion prior to study inclusion, diagnosis of diabetic ketoacidosis or hyperosmolar hyperglycemic state during the hospitalization, receipt of enteral tube feedings, or lack of research consent obtained at the time of admission. The study was reviewed and approved by the institution's Institutional Review Board.
Data collection
Records for all eligible patients hospitalized from an index date of March 1, 2010 to November 7, 2013 were retrospectively reviewed for study inclusion. It is notable that carbohydrate counting was implemented on June 1, 2011; therefore patients included prior to this date received fixed mealtime dosing only. The index date of March 1, 2010 was chosen to include an equivalent number of patients in each group. Data collection stopped on November 7, 2013, as an adequate sample had been obtained.
For each subject record, demographic data (age, gender, race, height, weight), diabetes history (type 1 or type 2, insulin use prior to admission), and baseline laboratory data (glycated hemoglobin [HbA1c], serum creatinine, and alanine aminotransferase) were collected. Data on glucose (capillary [point-of-care] values, date/time of lab draw, time of last food intake prior to lab draw), daily insulin doses administered, primary diagnosis, receipt of glucose-interfering medications (systemic corticosteroids or dextrose-containing hydration fluids), and infection (if present) were collected during the study period. Determinations of primary diagnosis and infection were made based on review of progress notes. Admission All Patient Refined Diagnosis Related Groups (APR-DRG) scores were collected as the marker of patient severity of illness. APR-DRG is a proprietary product (3M™ APR-DRG Expert Software) of 3M Health Information Systems (Salt Lake City, UT). 13 Study data were collected and managed using Microsoft (Redmond, WA) Excel™ and REDCap. REDCap (Research Electronic Data Capture) is a secure, Web-based application designed to support data capture for research studies. 14
Variables, end points, and definitions
Independent variables were body mass index, HbA1c, serum creatinine, alanine aminotransferase, primary diagnosis, receipt of glucose-interfering medication, infection, and severity of illness. The dependent variable was capillary glucose. The primary end point was mean daily postprandial glucose values (drawn ≤4 h after last charted meal intake) for the carbohydrate counting group and fixed mealtime dosing group. Secondary end points were preprandial glucose values (drawn >4 h after last charted meal intake), proportions of patients with hyperglycemia (>180 mg/dL) and hypoglycemia (<70 mg/dL), percentage of time within target glucose range (70–180 mg/dL), and mean daily insulin doses received.
Procedures
Providers dosed mealtime insulin as they determined appropriate upon review of the medical record. There were no standardized protocols followed. This flexibility was felt to be important because of the varying clinical status of patients, potential disruption in meal schedules, and patient preference. After implementation of carbohydrate counting, this was typically favored by the DCS providers because of its individualized approach. Use of carbohydrate counting on an outpatient basis and variable food intake in the hospital setting were anecdotally known to influence the decision to use carbohydrate counting. Calculation of the insulin-to-carbohydrate ratio was also based on the provider's discretion. A common practice was to use the Rule of 500 15 (total daily insulin dose/500) for calculation of the insulin-to-carbohydrate ratio. For example, a patient receiving 50 units/day would receive 1 unit for every 10 g of carbohydrate consumed (50/500=0.1 unit insulin/1 g of carbohydrate). Glucose levels were assessed daily, and adjustments were made by the DCS providers as appropriate. Capillary glucose checks were typically performed three or more times per day.
A room service model was used for delivery of patient meals during the study period. Patients could request meals as desired from 07:00 h to 19:00 h each day. Meals delivered for patients on carbohydrate counting included a ticket listing the total carbohydrate contents of each food item. Nurses were educated (via a required inservice) to calculate the total number of carbohydrates ingested based on the portion of each food item consumed and to administer the mealtime insulin dose based on the insulin-to-carbohydrate ratio ordered within 30 min (maximum, 45 min) of meal consumption. A Web-based calculator was used to assist in calculating the dose of insulin. The total grams of carbohydrate consumed and the dose of mealtime insulin were rounded to the nearest whole number. Actual time of insulin administration in relation to meals was not collected. Snacking was not covered by mealtime insulin orders in either group.
Statistical analysis
Daily basal insulin dose, daily mealtime/correction insulin dose (combined), average daily preprandial glucose, and average daily postprandial glucose were compared between treatment groups (carbohydrate counting vs. fixed mealtime insulin dosing) using repeated-measures linear regression models with log-transformed outcome scales. These comparisons were also adjusted for covariates previously identified to affect these outcomes: body mass index, serum creatinine, infection during study period, history of glucose medication, primary diagnosis, and HbA1c. In all these models a linear term for day and an autoregressive correlation structure (decreasing within-patient correlation with increasing distance between days) were used. An interaction between treatment group and day was investigated to assess whether the treatment effect varied by day. If not statistically significant, the interaction was removed from the models for interpretation purposes.
Daily risk of high (glucose >180 mg/dL) and low (glucose <70 mg/dL) preprandial and postprandial glucose values was compared between treatment groups using repeated-measures logistic regression models with generalized estimating equations. The daily high glucose risk comparisons were covariate-adjusted, but the daily low glucose risk comparisons were not because of the relatively small number of patients meeting the threshold. An autoregressive correlation structure and linear terms for day were used. Interactions between treatment group and day were assessed in the same manner as in the previously described models for the continuous outcomes.
The percentage of total follow-up time that glucose was in therapeutic range (70–180 mg/dL) was compared between groups using linear regression models, both unadjusted and adjusted for covariates.
All analysis used SAS software version 9.2 (SAS Institute Inc., Cary, NC).
Results
Characteristics of study population
Data on 225 qualifying patients were collected (113 patients in the carbohydrate counting cohort and 112 patients in the fixed mealtime dosing cohort) (Fig. 1). Patient characteristics are summarized in Table 1 and were similar for both cohorts. A large majority of patients had type 2 diabetes (96%) and were on insulin therapy prior to admission (87%). Mean HbA1c was 7.8% (62 mmol/mol), and most patients had a severity of illness designation of “major” on admission (APR-DRG score of 3). The most common primary diagnosis was heart failure exacerbation (43%). Approximately one-quarter of the patients had a concurrent infection, and fewer than 20% received a glucose-interfering medication during the study period. By study Day 7, 45 patients remained in the carbohydrate counting cohort and 36 patients in the fixed mealtime dosing cohort, indicating respective retention rates of 40% and 32% in each group. The number of capillary glucose values analyzed was significantly higher in the carbohydrate counting group.
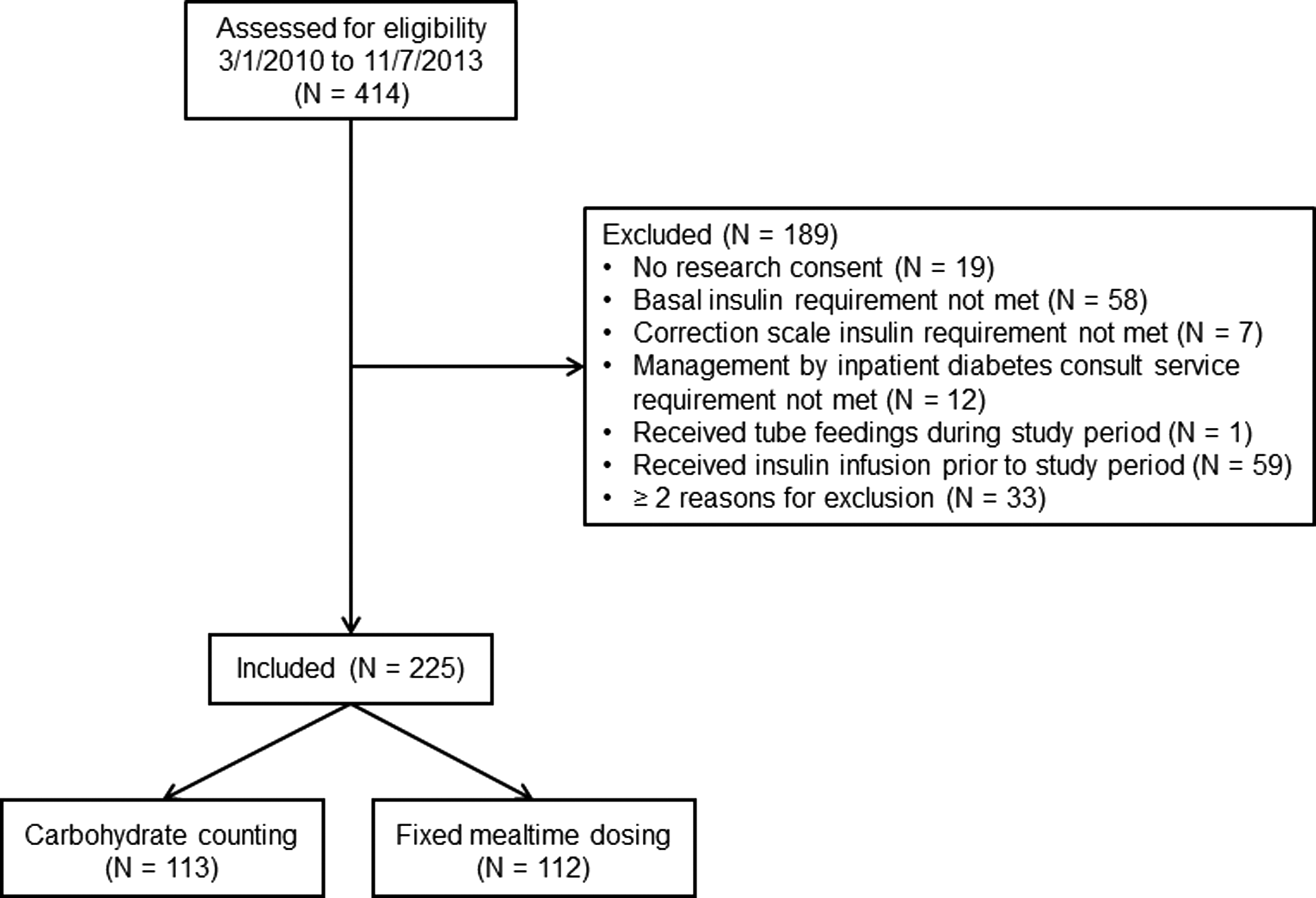
Study design.
Statistical comparisons are by the rank-sum test for continuous variables and Pearson's χ2 test for discrete variables.
n=208 (carbohydrate counting, n=105; fixed mealtime dosing, n=103).
n=189 (carbohydrate counting, n=113; fixed mealtime dosing, n=76).
ALT, alanine aminotransferase; APR-DRG, All Patient Refined Diagnosis Related Groups; BMI, body mass index; HbA1c, glycated hemoglobin; IQR, interquartile range.
Pre- and postprandial glucose values
For the mean daily postprandial glucose comparison (Fig. 2), the model indicated a significant group-by-day interaction, suggesting a difference in postprandial glucose change over time between the two groups (unadjusted P=0.01, adjusted P=0.02). The carbohydrate counting cohort experienced a lower mean daily postprandial glucose on study Day 1 (201 mg/dL vs. 213 mg/dL, unadjusted P=0.05, adjusted P=0.03) and a higher mean daily postprandial glucose on study Day 7 (204 mg/dL vs. 183 mg/dL, unadjusted P=0.04, adjusted P=0.12). Differences on Days 2–6 were not statistically significant.

Postprandial glucose. Group by day interaction: unadjusted P=0.01; adjusted P=0.02. Diamonds: means; lines inside bars: medians; N: number of patients. Mean postprandial glucose values (carbohydrate counting vs. fixed mealtime dosing, mg/dL):
For the mean daily preprandial glucose comparison, the model did not find a significant group-by-day interaction, which suggests there was no difference in preprandial glucose change over time between the two groups (P=0.19). Overall, no differences in preprandial glucose values were observed (unadjusted P=0.71, adjusted P=0.54).
Hyperglycemia, hypoglycemia, time within target range, and insulin doses
There were no differences in the proportion of patients with postprandial hyperglycemia (Fig. 3). A higher proportion of patients in the carbohydrate counting cohort experienced preprandial hyperglycemia on study Day 7 only (45% vs. 21%, unadjusted P=0.04, adjusted P=0.15) (Fig. 4).

Proportion of patients with postprandial hyperglycemia. Group by day interaction: unadjusted P=0.05, adjusted P=0.06. N: number of patients. Proportions (carbohydrate counting vs. fixed mealtime dosing):

Proportion of patients with preprandial hyperglycemia. Group by day interaction: unadjusted P=0.06, adjusted P=0.11. N: number of patients. Proportions (carbohydrate counting vs. fixed mealtime dosing):
There were no differences in the proportion of patients with postprandial hypoglycemia (overall 3.3% and daily range 0–5% for carbohydrate counting vs. overall 2.3% and daily range 0–4% for fixed dosing, P=0.38). A higher proportion of patients in the carbohydrate counting cohort experienced preprandial hypoglycemia compared with the fixed dosing cohort on Day 5 (8.6% vs. 1.5%, P=0.02), Day 6 (1.7% vs. 0%, P=0.01), and Day 7 (7.1% vs. 0%, P=0.008). Eleven patients in the carbohydrate counting cohort experienced a hypoglycemic preprandial event. For five of these patients (45%) the event occurred during morning hours (05:00–10:00 h), for another five patients (45%) it occurred during the late evening/early morning hours (10:01–04:59 h), and for one patient (10%) it occurred during both time frames. Three patients experienced a severe hypoglycemic episode (glucose<40 mg/dL) in the carbohydrate counting cohort; of these, two were preprandial, and one was postprandial. No patients in the fixed dosing cohort experienced severe hypoglycemia.
Mean percentage of time spent within target glucose range was similar between groups (carbohydrate counting vs. fixed dosing, 56% vs. 57%; unadjusted P=0.88, adjusted P=0.62). There were no differences in mean daily basal insulin (P=0.22) and combined mealtime/correction insulin doses administered (P=0.81), indicating similar insulin exposure. Mean daily basal insulin doses ranged from 26 to 31 units/day, and mean mealtime/correction insulin doses ranged from 20 to 31 units/day. On study Day 3, the median weight-based insulin dose was 0.50 units/kg/day (0.32–0.71 units/kg/day) in the carbohydrate counting cohort and 0.47 units/kg/day (0.33–0.68 units/kg/day) in the fixed mealtime insulin cohort (P=0.92). The daily mealtime/correction doses administered trended up during the study period for both cohorts, but this did not reach statistical significance (P=0.21).
Discussion
This study is the first to report the glycemic effects of mealtime insulin dosing by carbohydrate counting versus fixed mealtime insulin dosing in a homogeneous patient population when used in conjunction with basal and correction insulin in hospitalized patients. For the primary end point, fixed mealtime insulin dosing was associated with a lower mean postprandial glucose on Day 7, but this difference was not sustained in the adjusted analysis. Therefore, similar outcomes were observed in the postprandial glucose comparisons. Additionally, the mealtime dosing strategies were not different in the proportion of patients with postprandial hyperglycemia. Even though a higher proportion of patients in the carbohydrate counting cohort experienced preprandial hypoglycemia on the last 3 days of study inclusion, this observation may have been influenced by unknown factors independent of the mealtime insulin method. Total daily insulin doses (basal, mealtime, and correction) were comparable between groups. Insulin doses did not change significantly over the study period, potentially indicating clinical inertia (failure to adjust insulin doses in response to glucose excursions).
Although carbohydrate counting theoretically offers more individualized and targeted insulin dosing, this study does not support a glycemic control benefit for this approach over fixed mealtime dosing in the hospital setting and appears to be consistent with previous investigations. In a cohort of outpatients with type 2 diabetes, carbohydrate counting did not yield a difference in glycemic outcomes. 10 Dungan et al. 12 also compared inpatient glycemic control in patients receiving carbohydrate counting or fixed mealtime insulin; both groups achieved comparable mean glucose levels on study Day 3. Therefore, it is reasonable to assume that mealtime insulin dosing by insulin-to-carbohydrate ratios or by fixed doses adjusted for glucose trends is similarly effective in hospitalized patients. Having multiple strategies may increase a clinician's willingness to use basal–bolus management, 10 thereby improving management of inpatient hyperglycemia. Of note is that Pearson et al. 16 demonstrated improved provider and nurse confidence and satisfaction with dosing of mealtime insulin after the institution of carbohydrate counting.
Daily rates of patients with hypoglycemia in this study were less than those reported by Dungan et al. 12 (0–9% vs. 11–26%, respectively). Contrary to Dungan et al., 12 higher rates of preprandial hypoglycemia were observed with carbohydrate counting in the current study. A plausible explanation may be due to the process requirement of insulin dose administration after meal intake with carbohydrate counting to allow calculation of insulin dose based on the observed meal carbohydrate-content consumption. Because this calculation is not required with fixed dosing, this cohort may have received their mealtime insulin dose with or just following food intake. Closing the time window after meal intake to insulin administration may help decrease mealtime insulin-induced hypoglycemia. Additionally, it is difficult to ascertain the role of the basal insulin in this observation. Even though there was no specific time frame in which preprandial hypoglycemia occurred, 45% of carbohydrate counting patients experienced this in the early-middle morning hours.
This study has several limitations aside from its retrospective design. First, both groups were compared using a combination of basal, mealtime, and correction-scale insulin. It cannot be inferred if the glycemic outcomes were due to this combined approach, specifically the mealtime insulin method, or perhaps the basal insulin dose. Second, the choice of whether to use carbohydrate counting versus fixed mealtime dosing, as well as selection of insulin doses, was not standardized. Because this was based on the individual DCS providers' clinical judgment, it would be difficult to mimic either approach exactly as done in this study. Third, the grams of carbohydrates consumed with each meal were not known in the fixed dosing cohort; therefore differences in meal consumption cannot be analyzed. Additionally, because most patients were taking insulin prior to admission, data on pre-admission mealtime insulin doses may have been more easily used in the fixed dosing cohort. Even though total daily doses of insulin administered were collected, compliance with each of the insulin orders could not be fully assessed because the short-acting doses may have been held owing to an acute change in dietary intake. Lastly, the study cohort consisted of medical cardiology patients where almost all were using insulin prior to admission; therefore these results should not be extrapolated to patients receiving non-insulin therapy prior to admission.
In conclusion, mealtime insulin dosing by carbohydrate counting was associated with similar mean postprandial glucose levels when compared with fixed mealtime insulin dosing in hospitalized medical cardiology patients concurrently receiving basal insulin and correction-scale insulin. Higher rates of preprandial hypoglycemia were observed in the carbohydrate counting group, but it cannot be elucidated if the mealtime insulin method was the direct cause of this. Future studies are needed to prospectively compare carbohydrate counting with fixed mealtime insulin dosing in the hospital setting in a large, multicenter trial, as well as to evaluate patient outcomes aside from glycemic control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.