
Abstract
Background:
Sensor-augmented pump therapy (SAP) provides a useful adjunct relative to continuous subcutaneous insulin infusion (CSII) alone. It can provide early warning of the onset of hyperglycemia and hypoglycemia and has the functionality to suspend insulin delivery if sensor glucose levels fall below a predefined threshold. The aim was to assess the cost-effectiveness of SAP with low glucose suspend (LGS) versus CSII alone in type 1 diabetes.
Materials and Methods:
Cost-effectiveness analysis was performed using the CORE Diabetes Model, using published clinical input data. The analysis was performed in two cohorts: one with uncontrolled glycated hemoglobin at baseline and one at elevated risk for hypoglycemic events. The analysis was conducted from a healthcare payer perspective over a lifetime time horizon; future costs and clinical outcomes were discounted at 4% per annum.
Results:
In patients with uncontrolled glycated hemoglobin at baseline, SAP + LGS resulted in improved discounted quality-adjusted life expectancy (QALE) versus CSII (10.55 quality-adjusted life-years [QALYs] vs. 9.36 QALYs) but higher mean lifetime direct costs (€84,972 vs. €49,171) resulting in an incremental cost-effectiveness ratio (ICER) of €30,163 per QALY gained. In patients at elevated risk for hypoglycemia, the ICER was €22,005 per QALY gained for SAP + LGS versus CSII as lifetime costs were higher (€88,680 vs. €57,097), but QALE was also higher (18.46 QALYs vs. 18.30 QALYs).
Conclusions:
In France, projected improvements in outcomes with SAP + LGS versus CSII translated into an ICER generally considered as good value for money, particularly in patients who experience frequent and/or problematic hypoglycemic events.
Introduction
T
In France in 2013, an estimated 19% of patients with type 1 diabetes used insulin pumps (representing a twofold increase in the use of insulin pumps in children, adolescents, and adults since 2007). 4 Continuous subcutaneous insulin infusion (CSII) represents a valuable alternative to multiple daily injections and is indicated in patients who are unable to achieve glycemic control targets using multiple daily injections or who have frequent or problematic hypoglycemic events. 5 In these patient groups, CSII has been shown to substantially improve glycemic control and reduce the frequency of hypoglycemic events compared with multiple daily injections. 6
A useful adjunct to CSII is the use of continuous glucose monitoring (sensor-augmented pump [SAP] therapy) as this provides real-time feedback of glucose levels, thereby allowing a warning of the onset of hyperglycemia and hypoglycemia. SAP with a low glucose suspend (LGS) feature offers an added benefit over standard insulin pump therapy alone (CSII) in that it emits an alarm if sensor glucose levels fall below a certain preset threshold value and, if the patient does not respond to the alarm, stops insulin delivery for up to 2 h. This function has been shown to be especially useful in patients who are prone to hypoglycemia or have poor awareness of the onset of hypoglycemic events and/or those in whom early symptoms are subtle. In particular, in the ASPIRE study, the use of the LGS feature was shown to lead to a significant reduction in the incidence of nocturnal hypoglycemia in hypoglycemia-prone patients. 7
In the present analysis, the cost-effectiveness of SAP + LGS versus standard CSII alone was compared in two separate patient cohorts. The first cohort was a population with uncontrolled glycated hemoglobin (HbA1c) that used clinical input data from a 2014 meta-analysis by M. Cucherat et al. (manuscript in preparation), which showed that for patients with a baseline HbA1c of 9%, the use of SAP was associated with an HbA1c reduction of −0.88% compared with −0.48% for CSII alone. The second analysis was performed in a cohort with hypoglycemic concerns due to impaired awareness of hypoglycemia. This analysis used data from a randomized controlled trial in patients with impaired hypoglycemia awareness conducted in Australia. 8 After 6 months using SAP + LGS, no severe hypoglycemic events (defined as hypoglycemic seizure or coma) were reported compared with a rate of 2.2 per 100 patient-months in the CSII alone arm. The two separate analyses allowed independent assessment of the benefits of SAP + LGS versus CSII alone in terms of the benefits of improved glycemic control in a population with uncontrolled HbA1c and the effect of the incidence of severe hypoglycemic events in patients with impaired hypoglycemia awareness.
Materials and Methods
Simulation cohorts and treatment effects
Cost-effectiveness analyses were performed in two separate cohorts. The first cohort consisted of patients with uncontrolled HbA1c, and the second consisted of patients with an elevated risk for hypoglycemia due to impaired awareness of hypoglycemia.
For the analysis in the cohort with uncontrolled HbA1c, baseline characteristics were derived from a study by Riveline et al. 9 (n = 178 patients) conducted in the French setting and supplemented where necessary with cohort characteristics from the Diabetes Control and Complications Trial 10 (Table 1). The mean age of the cohort was 36 years, mean duration of diabetes was 17 years, and mean HbA1c at baseline was 9%. In this cohort it was assumed that patients used SAP 70% of the time (based on the SWITCH study 11 ), based on the annual use of 43 sensors each lasting for 6 days. A treatment effect in terms of HbA1c reduction of −0.88% for SAP and −0.48% for CSII alone was used in the model, based on the findings of a 2014 meta-analysis by M. Cucherat et al. (manuscript in preparation). This was an individual patient-level meta-analysis that included data from a total of seven randomized controlled trials 11 –17 that compared SAP with CSII plus self-monitoring of blood glucose (SMBG). For inclusion, studies were required to have a duration of at least 2 months and have a prospective design. Trials conducted in type 2 diabetes patients, pregnant women, and those using retrospective data collection were excluded. Additionally, the rate of severe hypoglycemic events was assumed to be equal in both arms at a rate of 2.6 episodes per 100 patient years. 18 SMBG use was assumed to be 7.11 strips per day in the CSII group and 4.35 strips per day in the SAP group based on data from an observational study by Lynch et al. 19
All values are mean (SD) unless otherwise specified.
Range in parentheses is the 95% confidence interval.
BMI, body mass index; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure.
For the analysis in the cohort with elevated risk of hypoglycemia, baseline characteristics and treatment effects were sourced from a randomized controlled trial by Ly et al. 8 (n = 95 patients). The mean patient age was 18.6 years, mean duration of diabetes was 12 years, and mean HbA1c at baseline was 7.5%. Rates of severe hypoglycemic events included in the model were 0 in the SAP + LGS arm and 2.2 per 100 patient-months in the CSII-alone arm (the incidence of moderate hypoglycemic events was not included in the analysis). 8 For consistency, the number of sensors used per year in this analysis was assumed to be the same as in the base case in the cohort with uncontrolled HbA1c. No treatment effect in terms of HbA1c was modeled, and assumptions relating to SMBG use were the same as in the base case analysis in the cohort with uncontrolled HbA1c.
Model description
The analysis was performed using the CORE Diabetes Model (IMS Health, Basel, Switzerland). The model is a validated non–product-specific policy analysis tool for cost-effectiveness analyses in either type 1 or type 2 diabetes. A detailed description of the model architecture and validation has been published previously. 20 –22 In summary, the model is based on a series of interdependent submodels that simulate diabetes-related complications (angina, myocardial infarction, congestive heart failure, stroke, peripheral vascular disease, diabetic retinopathy, macula edema, cataract, hypoglycemia, ketoacidosis, lactic acidosis, depression, edema, nephropathy and end-stage renal disease, neuropathy, foot ulcer and amputation, and nonspecific mortality). The submodels have a semi-Markov structure and use time-, state-, time-in-state–, and diabetes type–dependent probabilities derived from published sources to simulate disease progression. Monte Carlo simulation using tracker variables is used to overcome the memory-less properties of the standard Markov model and allows for interconnectivity and interaction between individual submodels.
Costs and utilities
The base case analyses were conducted from the healthcare provider perspective. Complication costs were sourced from published literature 23 –34 and where necessary inflated to 2014 € using the consumer price index specific for the healthcare sector from the Institut National de la Statistique et des Études Économiques 35 (Table 2). Intervention costs included in the model were calculated based on the incremental costs between the SAP and CSII arms (including lancet and SMBG use); the incremental cost in the SAP group was €2,603.25 per year (based on 43 sensors per year, a kit including the MiniLink™ transmitter, MiniLink charger, MiniLink tester, batteries, and Enlite™ serter™ [Medtronic International Trading Sàrl, Tolochenaz, Switzerland], and reduced SMBG use). For the sensitivity analysis performed from the societal perspective, indirect costs (using the human capital approach) were included based on a mean salary of €27,744 for males and €22,380 for females, 36 an average of 213.25 working days per year, 37 mean age at first income of 24.8 years, 38 and mean retirement age of 59 years. 39 The number of days off work due to diabetes-related complications was sourced from a study performed by the sponsor (Medtronic) in the Dutch setting.
All costs are presented in 2014 €.
All days off work data are sourced from a study conducted by the sponsor (Medtronic) in the Dutch setting.
Defined as a hypoglycemic event requiring third-party assistance.
Defined as hypoglycemic seizure or coma.
AITH, Agence Technique de l'Information sur l'Hospitalisation; CHF, congestive heart failure; PVD, peripheral vascular disease.
Utility values for complications were sourced from published literature. 40,41 Additionally, a utility gain of 0.0552 was applied to patients using SAP + LGS due to reduced fear of hypoglycemia, based on findings of the INTERPRET study. In this study SAP was associated with a 6.9 unit decrease in the Hypoglycemic Fear Survey, 42,43 and a 1 unit increase in Hypoglycemic Fear Survey score was associated with a 0.008 unit decrease on the EQ-5D™ (EuroQol Group, Rotterdam, The Netherlands) index. 44
In the analysis performed in the population with hypoglycemia concerns, a specific quality of life adjustment was made, 45 based on the findings of the trial by Ly et al. 8 A utility benefit of +0.038 was applied to the SAP + LGS arm, and a decrement of −0.035 was applied to the CSII-alone arm. Conservatively, no specific disutility for severe hypoglycemic events was applied in either arm.
Statistical approach and other model settings
In line with previous analyses performed using the CORE Diabetes Model, for each simulation a simulated cohort of 1,000 patients was run through the model 1,000 times using first-order Monte Carlo simulation. Long-term outcomes included total direct costs, life expectancy, quality-adjusted life expectancy (QALE), and time to onset of complications. The analysis was performed over a lifetime time horizon, and both future costs and clinical outcomes were discounted at 4% per annum in line with current recommendations for the French setting in order to adjust for costs and benefits being incurred at different time points throughout the simulation. 46
Sensitivity analysis
A series of one-way sensitivity analyses were performed to determine the robustness of the base case findings and determine the key drivers of cost-effectiveness. First, the influence of baseline HbA1c was assessed by changing the mean baseline value to 8% and 10% compared with 9% in the base case. The influence of complication costs was examined by increasing and decreasing mean costs by 20%. Similarly, the influence of the cost of the continuous glucose monitoring was examined by changing this by −20%, −10%, and +10% relative to the base case cost. Sensitivity analyses were performed in which the fear of hypoglycemia utility was either removed or increased to 0.0184 based on a study by Yeh et al. 47 The impact of SMBG use was also assessed; in the base case analysis SMBG use was assumed to be 7.11 per day for CSII alone and 4.35 per day for SAP. Scenarios were run where SMBG use was set to 7.11 per day in both arms, 7.11 per day for CSII alone versus 6.11 per day for SAP, and 7.11 per day for CSII versus 2.11 per day for SAP. A sensitivity analysis was performed in which the analysis was performed from a societal perspective, which incorporates indirect costs associated with productivity loss. Finally, the impact of time horizon and discount rate were assessed by varying the time horizon of the analysis to 5, 10, 20, and 40 years and the discount rates for future costs and benefits to 0%, 2.5%, and 6% per annum.
Results
Cohort with uncontrolled HbA1c
In the base case analysis, SAP + LGS was projected to be associated with a gain in discounted QALE of 1.19 quality-adjusted life-years (QALYs) compared with CSII alone (10.55 QALYs vs. 9.36 QALYs) (Table 3). However, SAP + LGS was also associated with higher total direct lifetime costs than CSII alone (€84,972 versus €49,171; difference, €35,801). The higher total direct costs for the SAP + LGS group were driven by higher treatment costs. However, the use of SAP + LGS led to substantial improvements in both life expectancy and QALE relative to CSII alone. The HbA1c benefit associated with SAP also led to a delay in the onset of all long-term complications included in the analysis. The most pronounced benefits were projected for gross proteinuria, first ulcer, neuropathy, and macular edema, where onset was delayed by ≥1.4 years relative to CSII alone (Table 4).
No discount rate is applied here compared with a discount rate of 4% per annum applied to clinical outcomes in the base case analysis.
CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; ICER, incremental cost-effectiveness ratio; LGS, low glucose suspend; QALY, quality-adjusted life-years; SAP, sensor-augmented pump.
CSII, continuous subcutaneous insulin infusion; LGS, low glucose suspend; SAP, sensor-augmented pump.
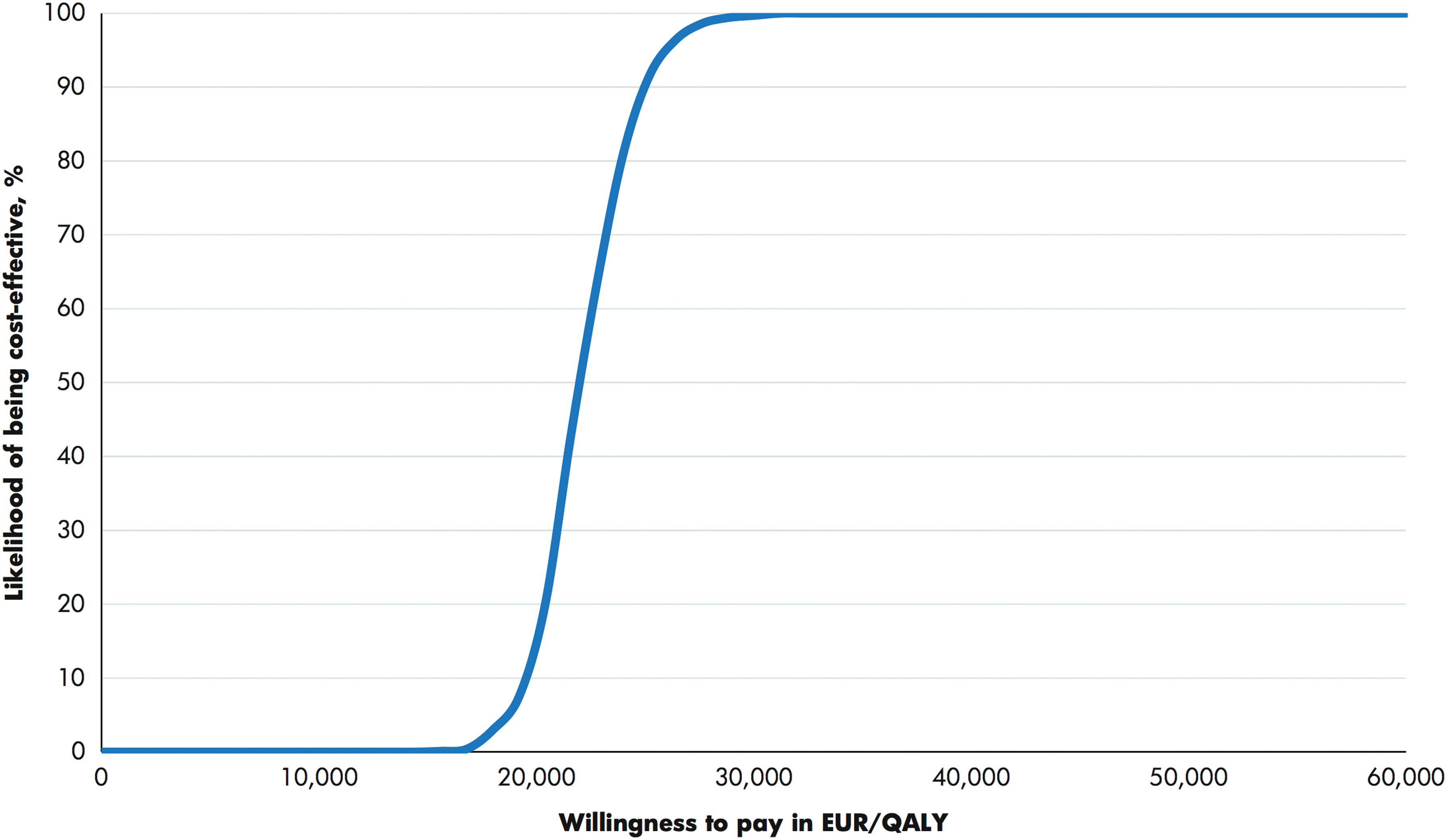
The higher costs and improved QALE resulted in an incremental cost-effectiveness ratio (ICER) of €30,163 per QALY gained for SAP + LGS versus CSII alone. Analysis of the cost-effectiveness acceptability curve, constructed from the cost-effectiveness plane scatterplot (Fig. 1), showed that at a willingness-to-pay threshold of €30,000 per QALY gained SAP + LGS had an 80% probability of being considered cost-effective compared with CSII alone; this value increased to 100% if the willingness-to-pay threshold was increased to €50,000 per QALY gained.

Cost-effectiveness acceptability curve for sensor-augmented pump + low glucose suspend versus continuous subcutaneous insulin infusion alone in the cohort with uncontrolled glycated hemoglobin at baseline. QALY, quality-adjusted life-years.
The findings from the sensitivity analyses showed that cost-effectiveness was most sensitive to changes in assumptions around the utility applied for reduced fear of hypoglycemia (Table 5). In a scenario in which this benefit was entirely negated, the ICER for SAP + LGS versus CSII alone increased to €118,993 per QALY gained. Similarly, if the fear of hypoglycemia benefit was reduced to a utility of 0.0184 (compared with 0.0552 in the base case), the ICER was €60,048 per QALY gained. Additionally, a sensitivity analysis was performed in which the analysis was performed from the societal perspective (i.e., incorporating indirect costs due to lost productivity). Here, the cost-effectiveness of SAP was improved slightly relative to the base case with an ICER of €26,863 per QALY. The cost-effectiveness of SAP was relatively sensitive to short time horizons as time horizons of 5 and 10 years increased the ICER to over €37,265 per QALY gained. The ICER was also influenced by assumptions relating to SMBG use; in a scenario in which no reduction in SMBG use was assumed, the ICER increased to €36,597 per QALY gained. The cost-effectiveness of SAP versus CSII alone was relatively insensitive to changes in discount rate and costs of diabetes-related complications.
CSII, continuous subcutaneous insulin infusion; FoH, fear of hypoglycemia; HbA1c, glycated hemoglobin; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year; SAP, sensor-augmented pump; SHE, severe hypoglycemic event; SMBG, self-monitoring of blood glucose.
Cohort with increased risk for hypoglycemia
In the analysis in the cohort with high risk for severe hypoglycemic events due to impaired awareness of hypoglycemia, SAP + LGS was associated with an incremental gain in discounted QALE of 1.44 QALYs compared with CSII alone, although lifetime direct costs were €31,583 higher with SAP + LGS than with CSII alone (Table 3). This resulted in an ICER of €22,005 per QALY gained for SAP + LGS versus CSII (Fig. 2).
Cost-effectiveness acceptability curve for sensor-augmented pump + low glucose suspend versus continuous subcutaneous insulin infusion alone in the cohort at increased risk for hypoglycemia. QALY, quality-adjusted life-years.
Sensitivity analyses in the cohort with increased risk for hypoglycemia were performed around discount rates, time horizon, and rates of severe hypoglycemic events (Table 5). In the base case analysis, the rate of severe hypoglycemic events in the CSII alone arm was 2.2 per 100 patient-months; rates of one and eight events per 100 patient-months were used in sensitivity analyses. This was found to be a key driver of outcomes, with a rate of one event per 100 patient months in the CSII arm leading to an ICER of €26,521 per QALY gained (versus €22,005 per QALY gained in the base case). Similarly, increasing the rate to eight events per 100 patient-months resulted in an ICER of €8,028 per QALY gained.
Discussion
Guidelines for the French setting state that continuous glucose monitoring is indicated in type 1 diabetes patients not meeting HbA1c targets and/or having frequent or undetected mild hypoglycemic events (particularly nocturnal events) and/or frequent severe hypoglycemic events. 48 The findings of the long-term cost-effectiveness analysis showed that in the French setting for patients with chronic hyperglycemia (baseline HbA1c of 9%), the use of SAP + LGS versus CSII alone was associated with a gain in QALE of 1.19 QALYs, leading to an ICER of approximately €30,000 per QALY gained, which is generally considered as very good value for money in France. The incremental benefit of SAP + LGS use was greater in the analysis in the cohort with elevated risk of hypoglycemia. Here, the reduction in the incidence of severe hypoglycemic events, which can only be achieved with LGS, resulted in a gain of over 1.44 QALYs and an ICER of €22,005 per QALY gained relative to CSII alone.
The results of the analyses suggest that the cost-effectiveness profile of SAP + LGS versus CSII in patients with elevated risk of hypoglycemic events is better than in the cohort with uncontrolled HbA1c at baseline. The phenomenon of impaired hypoglycemia awareness is common in patients with type 1 diabetes of long-standing duration, whereby the patient's ability to perceive the early symptoms of a hypoglycemic event diminishes over time, resulting in an increased risk of severe hypoglycemic events. An estimated 20–25% patients with type 1 diabetes have impaired hypoglycemia awareness, 49,50 and in one small-scale study it was associated with a sixfold increase in the risk of severe hypoglycemia. 51 The reduction in the incidence of severe hypoglycemic events associated with SAP + LGS is associated with not only clinical benefits from the patient perspective, but also a substantial economic benefit from the payer perspective owing to the substantial cost and health resource utilization associated with the treatment of severe hypoglycemic events.
The current analysis may also be conservative with respect to benefits in this population as it only considered severe hypoglycemic events and not minor hypoglycemic events. Although the majority of minor hypoglycemic events are associated with no or minimal healthcare costs, they have been shown to have a negative impact on health-related quality of life. Additionally, in the base case analysis cost-effectiveness improved when the analysis was performed from a societal perspective. Indeed, the benefits of SAP + LGS are larger when considered from a societal perspective owing to the impact of hypoglycemic events on lost productivity. A recent multicountry analysis indicated that even nonsevere hypoglycemic events were associated with a productivity loss of 8.3–15.9 h/month in patients with self-reported type 1 or type 2 diabetes. 52
Findings from one-way sensitivity analyses in the cohort with uncontrolled HbA1c showed that a key driver of cost-effectiveness was the positive impact of SAP + LGS in terms of reducing fear of hypoglycemia. Fear of hypoglycemia is common in adult patients with type 1 diabetes and also in the parents of pediatric patients. It can represent a major barrier to optimal glycemic control and have a negative impact on quality of life, particularly in patients with a history of severe hypoglycemic events. 53 Fear of hypoglycemia may also lead to patients reducing insulin doses or altering eating patterns to raise glucose levels, which can in turn negatively influence glycemic control and increase the risk of long-term diabetes-related complications. In the sensitivity analysis in which the fear of hypoglycemia benefit was negated, the ICER increased to a level that would no longer be considered cost-effective. However, improved glycemic control was also an important driver of cost-effectiveness, with the improved glycemic control associated with SAP + LGS resulting in long-term clinical benefits manifest in terms of delayed onset and reduced incidence of long-term complications as well as economic benefits due to lower mean long-term complication costs.
The present study is the first to assess the long-term cost-effectiveness of SAP + LGS versus CSII alone in patients with type 1 diabetes in France who have uncontrolled HbA1c or who have an elevated risk for hypoglycemic events. A previous analysis by Ly et al. 54 conducted in the Australian setting investigated the cost-effectiveness of SAP + LGS versus CSII alone in a population with impaired hypoglycemia awareness over a period of 6 months and also used clinical input data from the randomized controlled trial by Ly et al. 8 As the Australian cost-effectiveness analysis was based on the same clinical input data as the secondary analysis presented here, as expected, the findings of the two analyses largely concur.
Ly et al. 54 reported that the use of SAP + LGS versus CSII alone was associated with an ICER of $40,803 Australian (€28,531) per QALY gained for patients ≥12 years of age (September 5, 2014 exchange rate). However, caution should be attached to comparison between the Ly et al. 54 analysis and the base case analysis presented here owing to different cohort characteristics and country settings. Additionally, it should also be noted that in the randomized controlled trial by Ly et al. 8 the authors noted two outliers (both children ≤10 years of age) who had a high number of hypoglycemic events. In the overall cohort, at end point the rate of severe hypoglycemic events was 2.2 per 100 patient-months for CSII and 0 for the SAP + LGS group. In a sensitivity analysis in which the two outlier patients were excluded, the incidence rate ratio for severe hypoglycemic events was reduced to 1.5 (range, 0.2–2.7) in favor of SAP + LGS for severe events only, but remained statistically significant (P = 0.02).
In the present cost-effectiveness analysis a sensitivity analysis was performed in which the incidence of severe events in the CSII group was reduced to one event per 100 patient-months in the CSII group and zero in the SAP + LGS group (compared with 2.2 events per 100 patient-months in the CSII group in the base case analysis). In this scenario the ICER increased to €26,521 per QALY gained (versus €22,005 per QALY gained in the base case), showing that although cost-effectiveness is reduced SAP + LGS is still likely to be considered cost-effective.
In France, the proportion of patients with type 1 diabetes on CSII is estimated at 19%. 4 In this setting, the use of SAP + LGS could be particularly beneficial in both pediatric and adult patients who have an inability to achieve good glycemic control or are at risk of severe hypoglycemia. A limitation of the current analysis is that it did not consider cost-effectiveness separately within a pediatric population; cohort characteristics for the hyperglycemic cohort were sourced from Riveline et al., 9 which included patients 8–60 years of age and with a mean age of 36 years. Similarly, cohort characteristics for the cohort at increased risk for hypoglycemia were sourced from a study by Ly et al., 8 which also enrolled a mixed population of children and adults with an age range of 4–50 years, although the mean age was 18.6 years, suggesting that the cohort was predominantly children and young adults. However, the CORE Diabetes Model is largely based on long-term data from adult patients; therefore the validity of an analysis conducted in an exclusively pediatric population may be limited.
A further limitation of the analysis in the cohort at risk of hypoglycemia is the small-scale nature of the randomized control trial from which clinical input data were sourced and also the nature of the population. The population for this analysis was patients with increased risk for hypoglycemic events primarily due to impaired hypoglycemia awareness rather than patients with a documented history of frequent severe hypoglycemic events. As one of the key benefits of SAP + LGS is the reduced risk of severe hypoglycemic events, SAP + LGS is also likely to be cost-effective in patients with a history of severe hypoglycemia. A final limitation of the current analysis is that in the absence of data it was assumed that healthcare provider/training time would be the same for both the CSII-alone and SAP + LGS arms. In routine clinical practice it is possible that more healthcare provider time would be required for SAP + LGS. However, additional training time is likely to be small and is a one-time only cost and unlikely to have significantly influenced the overall conclusion of the analysis. Additionally, additional training costs associated with SAP may have been offset by the benefits of improved glycemic control and potentially less frequent follow-up visits.
In conclusion, the results of the analysis suggest that adding continuous glucose monitoring (SAP + LGS) in patients already using insulin pump therapy is cost-effective in the French setting, assuming a willingness-to-pay threshold of €30,000 per QALY gained. The cost-effectiveness of SAP + LGS versus CSII is largely driven by reduced fear of hypoglycemia, improvements in life expectancy, and the gain in QALE associated with this, as well as a reduction in the incidence of severe hypoglycemic events in those patients with impaired hypoglycemia awareness.
Footnotes
Acknowledgments
This study was supported by funding from Medtronic International Trading Sàrl.
Author Disclosure Statement
M.C. and H.H. have received consulting fees from Medtronic. J.S.-P. and W.V. are current employees of Ossian Health Economics and Communications, which has received consulting fees from Medtronic International Sàrl. S.R. is a current employee of HEVA HEOR, which has received consulting fees from Medtronic International Sàrl. S.P. and N.P are current employees of Medtronic International Trading Sàrl. V.P. is a current employee of Medtronic France SAS.