
Abstract
Background:
Fibroblast growth factor (FGF)-21 is an important regulator of glucose metabolism. In the present study, we investigated whether plasma levels of FGF-21 changed in patients with newly diagnosed type 2 diabetes mellitus (T2DM) and assessed the effects of metformin treatment on plasma FGF-21 levels.
Materials and Methods:
The plasma FGF-21 levels and the metabolic parameters of 226 patients with newly diagnosed T2DM and 100 sex- and age-matched normal glycemic tolerant (NGT) controls were measured. Seventy-four patients among of the 226 patients with T2DM were treated with metformin throughout the 12-week study period. The fasting plasma FGF-21 and high-sensitivity C-reactive protein (hs-CRP) levels were measured using enzyme-linked immunosorbent assay kits.
Results:
The patients with T2DM had significantly higher fasting plasma FGF-21 levels (302.2 pg/mL [range, 201.3–454.4 pg/mL] vs. 104.5 pg/mL [range, 71.6–185.6 pg/mL]; P < 0.00) and hs-CRP levels (2.63 ± 2.81 mg/L vs. 1.58 ± 2.16 mg/L; P < 0.00) than the NGT subjects. The fasting plasma hs-CRP and FGF-21 levels were significantly decreased in the T2DM group after metformin treatment compared with pretreatment (respectively, 2.56 ± 1.75 mg/L vs. 3.28 ± 1.89 mg/L [P < 0.05] and 232.6 pg/mL [range, 154.3–307.8 pg/mL] vs. 313.9 pg/mL [range, 227.7–474.2 pg/mL] [P < 0.01]).
Conclusions:
In patients with T2DM, the plasma FGF-21 levels are increased but are significantly decreased after metformin treatment. Metformin may play a role in reducing the FGF-21 levels in patients with T2DM, likely through the amelioration of glucose-lipid metabolism and inflammation.
Introduction
F
Although FGF-21 is important as a metabolic regulator and research has been conducted in animals, the exact role of FGF-21 in human physiology remains to be elucidated, and the effect of common antidiabetes treatment on the plasma levels of FGF-21 is not well known. Impaired insulin-stimulated glucose turnover in insulin-dependent peripheral tissues, such as liver, muscle, and adipocytes, is a major characteristic of T2DM. With respect to diabetes therapy, the addition of thiazolidinedione and exenatide therapy in patients with T2DM as well as the use of mitiglinide or short-term continuous subcutaneous insulin infusion in patients with newly diagnosed T2DM was followed by a significant reduction in circulating FGF-21 levels. These studies suggest that FGF-21 decreases as insulin sensitivity improves. 10 –13
However, the effect of metformin on FGF-21 remains unclear. Metformin, the widely used antihyperglycemic agent, decreases plasma levels of low-density lipoprotein cholesterol (LDL-C) and triglycerides (TG) and improves insulin sensitivity. 14,15 A study has shown a strong dose-dependent increase in FGF-21 expression in rat and human hepatocytes treated with metformin; this effect was blocked by the addition of the AMP-activated protein kinase inhibitor compound C. The study reported that metformin is a potent inducer of hepatic FGF-21 expression and that the effect of metformin seems to be mediated through AMP-activated protein kinase activation. 16 Because FGF-21 therapy normalizes blood glucose in animal models of T2DM, the induction of hepatic FGF-21 by metformin might play an important role in metformin's antidiabetes effect.
The present study demonstrated that metformin increases the expression of FGF-21 and that the effect of metformin on FGF-21 expression seems to be mediated through AMP-activated protein kinase activation. Our study evaluated the effects of metformin on the plasma FGF-21 levels in patients with newly diagnosed T2DM.
Materials and Methods
Subjects
In total, 336 Chinese volunteers who participated in this study were categorized into two groups. The first group comprised 226 individuals with newly diagnosed T2DM, and the second group comprised 100 sex- and age-matched normal glycemic tolerance (NGT) controls. That these individuals did not have diabetes was confirmed using a normal oral glucose tolerance test. The diagnostic criteria for diabetes mellitus were based on a 75-g oral glucose tolerance test as recommended by World Health Organization criteria. We tested fasting C-peptide level and diabetes antibodies, including glutamic acid decarboxylase. Patients with a normal C-peptide level and who were glutamic acid decarboxylase negative were diagnosed as having T2DM. These patients had received neither diabetes medications nor diet therapy before the present study. In total, 74 individuals with newly diagnosed T2DM were treated with metformin. The selection criteria included the following: individuals ranging in age between 18 years and 80 years without the presence of major diabetes complications and major organ diseases. The exclusion criteria were as follows: abnormal kidney function, serum creatinine level of ≥133 μmol/L, presence of diseases affecting blood glucose levels (such as hyperthyroidism and hypercortisolism), treatments affecting blood glucose levels (such as steroid hormones), pregnancy, breast-feeding, and patients with a history of excessive alcohol consumption.
This study was conducted in accordance with the recommendations of the Declaration of Helsinki. The study was approved by the Human Research Ethics Committee of Beijing Chaoyang Hospital affiliated with Capital Medical University. Informed consent was obtained from all of the participants in this study.
Study design
In total, 74 patients with newly diagnosed diabetes were treated with metformin (1.0–2.0 g/day) throughout the 12-week study period. The dose of metformin was adjusted to a maximum of 2.0 g/day on the basis of fasting blood glucose (FBG) and 2-h postprandial blood glucose (2hPBG).
The NGT control group did not receive any medication.
No subject dropped out of the study.
Anthropometric measurements were obtained before and after metformin treatment. The anthropometric measurements were obtained in the morning, before breakfast, and with the subject wearing light clothing and without shoes.
The blood samples were obtained before and after 12 weeks of metformin treatment for measuring metabolic parameters and plasma FGF-21 levels. Plasma glucose, serum lipid, liver enzymology, fasting insulin level (FINS), adiponectin, high-sensitivity C-reactive protein (hs-CRP), and FGF-21 were evaluated. After 75 g of glucose was administered as a 20% glucose solution, a venous blood sample was obtained at baseline and at 120 min. The plasma glucose level and glycated hemoglobin (HbA1c) were immediately measured using the glucose-oxidase technique or anion-exchange high-performance liquid chromatography, respectively, to avoid anaerobic glucose consumption. TG, total cholesterol (TCH-C), high-density lipoprotein cholesterol, and LDL-C concentrations were enzymatically determined. The plasma insulin concentration was measured using a chemiluminescence immunoassay (Beckman Coulter, Inc., Brea, CA). The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated from FINS, and the glucose levels were determined using the following equations: HOMA-IR = FINS (mU/L) × FBG (mmol/L)/22.5.
Plasma was subsequently stored at −80°C for assessing plasma fasting adiponectin and FGF-21. The fasting plasma FGF-21 levels were determined using an enzyme-linked immunosorbent assay (EMD Millipore, Inc., Billerica, MA). The human FGF-21 linear range of the assay was 10–2,000 pg/mL. The appropriate range of this assay is 31.25–2,000 pg/mL. The inter- and intra-assay coefficients of variation were 1.2% and 9%, respectively.
Statistical analyses
We performed the statistical analyses using SPSS version 21.0 software (SPSS, Inc., Chicago, IL). Because the plasma insulin, FGF-21, and HOMA-IR values were skewed distributions in the patients, logarithmically transformed values were used in the statistical analyses. The baseline characteristics of the case and control subjects were compared using a t test or the Mann–Whitney U test. The paired t test or Mann–Whitney U test was used to compare the differences in the biochemical characteristics and FGF-21 levels between pre- and posttreatment with metformin in the T2DM group. All of the statistical analyses were two-sided. All of the data are presented as the mean ± SD values or medians (interquartile ranges). P < 0.05 was considered to be statistically significant.
Results
Clinical characteristics fasting plasma FGF-21 levels of the study participants
The characteristics of the study subjects are summarized in Table 1. The clinical characteristics of the two groups did not show any differences in gender distribution. The T2DM group demonstrated higher body mass index (BMI) as well as systolic and diastolic blood pressures (P < 0.05). The T2DM group exhibited higher FBG, 2hPBG, FINS, HOMA-IR, γ-glutamyl transferase, TCH-C, TG, and apolipoprotein B levels but lower apolipoprotein A and high-density lipoprotein cholesterol levels than the NGT groups (P < 0.05) (Table 1). The fasting plasma FGF-21 levels and hs-CRP levels were significantly higher in the patients with T2DM than in the NGT subjects (P < 0.05) (Fig. 1).
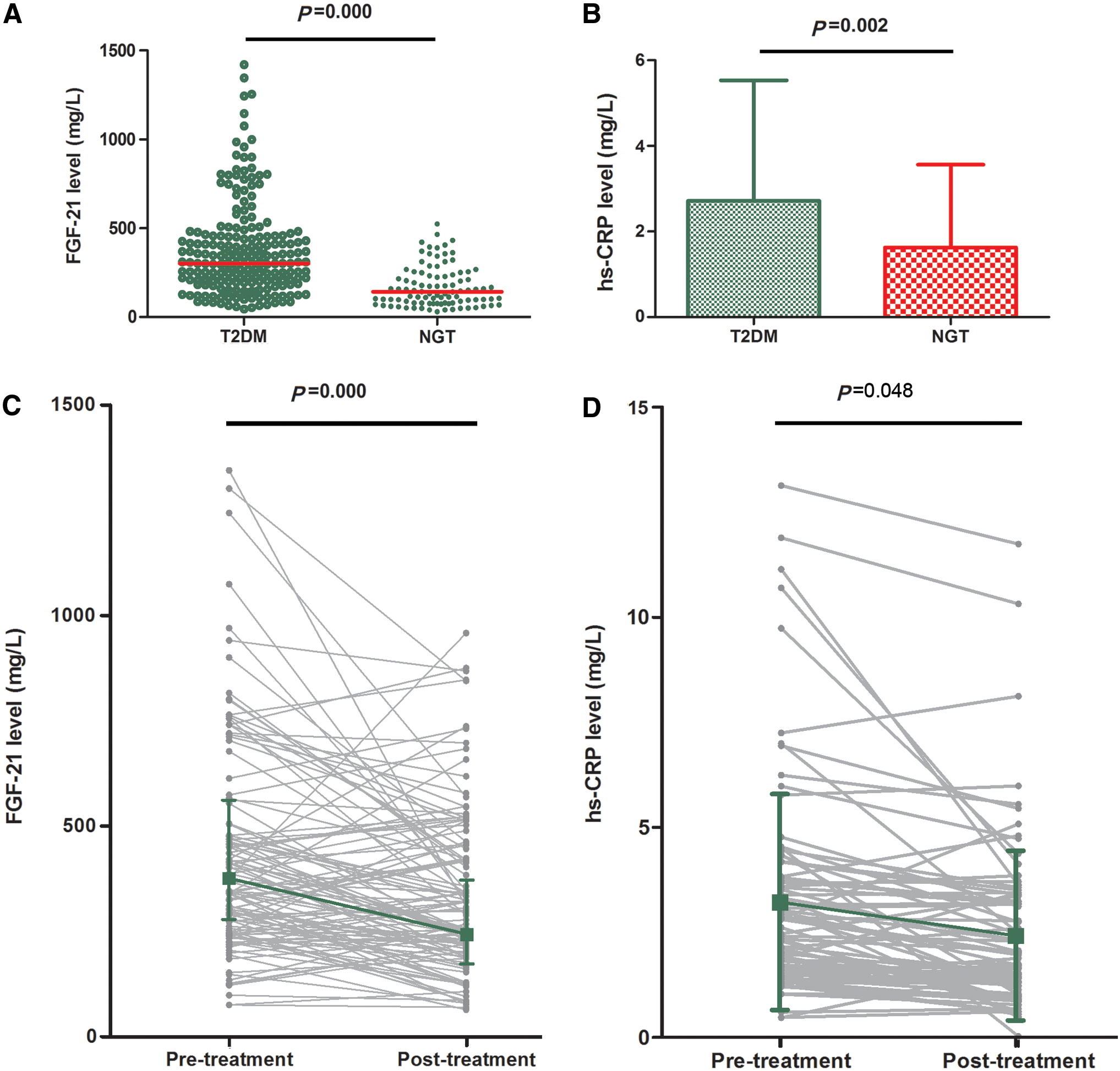
Data are mean ± SD values or median (interquartile ranges), as indicated. The clinical characteristics of the two groups did not show significant difference in gender distribution. The type 2 diabetes mellitus (T2DM) group had higher body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP) (P < 0.05). The T2DM group also had higher fasting blood glucose (FBG), 2-h postprandial blood glucose (2hPBG), fasting insulin (FINS), homeostasis model assessment of insulin resistance (HOMA-IR), γ-glutamyl transferase (γ-GT), total cholesterol (TCH-C), triglyceride (TG), and apolipoprotein B (APO-B) but lower apolipoprotein A (APO-A) and high-density lipoprotein cholesterol (HDL-C) than the normal glycemic tolerance (NGT) group (P < 0.05). Fasting plasma fibroblast growth factor (FGF)-21 levels and high-sensitivity C-reactive protein (hs-CRP) levels were higher significantly in patients with T2DM than in NGT subjects (P < 0.05). The continuous variables were compared by t test. Proportions were compared by a χ2 test.
P < 0.05, b P < 0.01 versus control group.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; F, female; HbA1c, glycated hemoglobin; LDL-C, low-density lipoprotein cholesterol; M, male.
Effects of metformin on clinical characteristics and FGF-21 levels in the T2DM group
The clinical characteristics and FGF-21 levels in the T2DM group before and after metformin treatment (1.0–2.0 g/day for 12 weeks) are summarized in Table 2.
Data are mean ± SD values or median (interquartile ranges), as indicated. After 12 weeks of treatment with metformin, body weight, body mass index (BMI), glycated hemoglobin (HbA1c), fasting blood glucose (FBG), 2-h postprandial blood glucose (2hPBG), aspartate aminotransferase (AST), alanine aminotransferase (ALT), fasting insulin (FINS), and homeostasis model assessment of insulin resistance (HOMA-IR) in type 2 diabetes mellitus patients showed significant declines. Dyslipidemia was improved after treatment with metformin. The fasting levels of total cholesterol (TCH-C), triglyceride (TG), and low-density lipoprotein cholesterol (LDL-C) were decreased. Fasting plasma fibroblast growth factor (FGF)-21 levels were also significantly decreased (P < 0.01). There was a remarkably reduced high-sensitivity C-reactive protein (hs-CRP) level (P < 0.05) after addition of metformin therapy in the type 2 diabetes mellitus group. The continuous variables were compared by t test.
P < 0.05, b P < 0.01 versus before treatment.
APO-A, apolipoprotein A; APO-B, apolipoprotein B; DBP, diastolic blood pressure; γ-GT, γ-glutamyl transferase; HDL-C, high-density lipoprotein cholesterol; SBP, systolic blood pressure.
The major side effects of the metformin treatment included nausea, upper abdominal discomfort, and decreased appetite. Three patients treated with metformin developed diarrhea. The patients were tolerant to these side effects within 2–3 weeks.
After 12 weeks of metformin treatment, the body weight, BMI, HbA1c, FBG, 2hPBG, aspartate aminotransferase, alanine aminotransferase, FINS, and HOMA-IR in patients with T2DM were significantly decreased (Table 2). Dyslipidemia was improved after metformin treatment. The fasting levels of TCH-C, TG, and LDL-C were decreased. It is interesting that the fasting plasma FGF-21 levels were also significantly decreased (232.6 pg/mL [154.3, 307.8 pg/mL] vs. 313.9 pg/mL [227.7, 474.2 pg/mL]; P < 0.01). Meanwhile, the hs-CRP level was remarkably reduced (2.56 ± 1.75 mgl/L vs. 3.28 ± 1.89 mgl/L; P < 0.05) after the addition of metformin in the T2DM group (Fig. 1).
Discussion
Previous studies in humans showed that the plasma FGF-21 levels were significantly associated with BMI, waist circumference, and markers of insulin resistance and were elevated in subjects with metabolic syndrome as well as with fatty liver diseases, thus suggesting that FGF-21 resistance may play a role in the pathogenesis of these diseases. 17,18
In the present study we measured the plasma FGF-21 levels and assessed the association between the plasma FGF-21 levels and BMI as well as several metabolic parameters in newly diagnosed T2DM patients and controls without diabetes. Our results demonstrated that the plasma FGF-21 levels were elevated in T2DM patients and were positively correlated with TG and HOMA-IR. The multiple regression analysis showed that TG and HOMA-IR were independently related to the fasting plasma FGF-21 levels. This finding was, in part, consistent with three other reports in humans that demonstrated elevated plasma FGF-21 concentrations in obesity and T2DM. 17 –19 The elevated plasma FGF-21 levels in insulin-resistant states might reflect a compensatory response to offset the peripheral and hepatic insulin resistance and might not be a cause for insulin resistance. Because this observation was cross-sectional in nature, it was not possible to establish a cause-and-effect relationship. These findings suggested a likely interaction between the homeostasis of glucose and lipids and the secretion of FGF-21 in humans.
In the present study we observed the effect of metformin on the plasma FGF-21 levels. Our study showed a significant decrease in plasma FGF-21 as well as in the BMI, TCH-C, LDL-C, TG, HbA1c, FBG, 2hPBG, FINS, and HOMA-IR after metformin treatment. Additionally, we observed that significantly decreased plasma FGF-21 levels were correlated with the amelioration of glucose and lipid metabolism in patients with T2DM after metformin treatment. The likely implication was that the changes in the FGF-21 levels associated with metformin treatment observed in our T2DM subjects were more strongly linked to the changes in glucose-lowering parameters rather than in other metabolic parameters. In other diabetes therapies, the addition of thiazolidinediones and glucagon-like peptide-1 therapy in T2DM patients and the use of mitiglinide or insulin infusion in patients with newly diagnosed T2DM were followed by a significant reduction in the circulating FGF-21 levels. 10 –13 However, in our study metformin treatment ameliorated dyslipidemia (e.g., TCH-C, LDL-C, and TG), except for decreased HbA1c and FINS. Therefore, except for glucose, ameliorated dyslipidemia may play a partial role in decreasing the circulating FGF-21 levels. 20
Mai et al. 21 studied the effects of free fatty acids and insulin on FGF-21 under physiological conditions. These results from two independent human randomized controlled trials suggested that free fatty acids increase the circulating FGF-21, whereas insulin is only of minor importance under physiological conditions. This mechanism might explain the apparent paradox of increased FGF-21 levels in obesity, insulin resistance, and starvation. 21
FGF-21 has previously been shown to lower blood glucose, thus improving peripheral insulin sensitivity, enhancing glucose transportation in adipocytes, and preventing pancreatic β-cells from apoptosis. It is preferentially expressed in the liver and has been identified as a potent regulator of glucose and lipid homeostasis. 22 However, at present, an exact knowledge of FGF-21 bioactivity and its physiological function is lacking.
We observed a decrease in the fasting plasma FGF-21 levels after treatment with metformin in patients with T2DM, which was inconsistent with the results in hepatocytes reported by Nygaard et al. 16 The study in hepatocytes with metformin showed that metformin is a potent inducer of hepatic FGF-21 expression and that the effect of metformin appears to be mediated through AMP-activated protein kinase activation. 16 This discrepancy could be caused by the improved insulin sensitivity, including relieving glucotoxicity and lipotoxicity, as shown in our study. The augmented expression of hepatic FGF-21 may consequently alleviate FGF-21 resistance, improve the physiological hypoglycemic effect of FGF-21, and reduce the plasma FGF-21 levels; however, this observation requires additional investigation. As FGF-21 therapy normalizes blood glucose in animal models of T2DM, the induction of hepatic FGF-21 by metformin might play an important role in metformin's antidiabetes effect. 16 Additionally, because diet and lifestyle modifications were only subjectively assessed, the changes in FGF-21 levels may be in part attributable to diet and lifestyle modifications. To our knowledge, few articles related to orally antidiabetes drugs and FGF-21 relations. Zhang et al. 23 found that in newly diagnosed T2DM patients, metformin significantly decreased the FGF-21 level. Li et al. 10 discovered that rosiglitazone treatment made a significant decrease on FGF-21.
However, the effect of metformin on FGF-21 levels could be regulated via an anti-inflammation effect. As an inflammatory marker, hs-CRP can reflect the severity of metabolic syndrome in the chronic inflammatory state. Considerable numbers of studies support the beneficial effects of metformin on the metabolic syndrome, diabetes, and inflammation. 24,25 To determine whether the change in FGF-21 alleviated inflammation, we measured the plasma hs-CRP levels at the same time. Our study showed that the plasma hs-CRP level declined significantly after metformin treatment. These results were consistent with our previous research, in which we found that glucagon-like peptide-1 receptor agonist treatment can relieve nonalcohol fatty livers. 26 However, in this study we could not determine whether hs-CRP or inflammation played a role in reducing FGF-21 and whether reduced FGF-21 levels were responsible for ameliorating glucose-lipid metabolism after metformin treatment. Several studies have suggested that the potential of FGF-21 for promoting adiponectin production is significantly decreased in mice with obesity and T2DM. The capability of FGF-21 for decreasing the plasma levels of fatty acids, TG, and glucose is also restricted in diet-induced obese mice. 27,28 Therefore more accurate and meaningful animal studies and clinical randomized clinical trial research for assessing the interaction between inflammation and FGF-21 are warranted.
In conclusion, for the first time, our study found that metformin treatment significantly decreased the plasma FGF-21 levels in patients with T2DM. The reduction of plasma FGF-21 levels was found to be associated with the amelioration of glucose-lipid metabolism and inflammation. Considering these findings, our results supported the hypothesis that FGF-21 may be related to insulin resistance, dyslipidemia, and inflammation in humans. The biological mechanism of FGF-21 action and its interaction with insulin resistance and inflammation in humans warrant additional investigation. Our findings suggested that metformin might be an important factor for the FGF-21 levels and that the FGF-21 pathway might be a compensatory mechanism for insulin resistance. The administration of metformin therapy decreases FGF-21 levels, likely by relieving inflammation, ameliorating glucose-lipid metabolism, and improving insulin sensitivity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.