
Abstract
Background:
Exercise helps individuals with prediabetes or type 2 diabetes (T2D) manage their blood glucose (BG); however, exercise adherence in this population is dismal. In this pilot study we tested the efficacy of a self-monitoring group-based intervention using continuous glucose monitors (CGMs) at increasing exercise adherence in individuals with impaired BG.
Materials and Methods:
Thirteen participants with prediabetes or T2D were randomized to an 8-week standard care exercise program (CON condition) (n = 7) or self-monitoring exercise intervention (SM condition) (n = 6). Participants in the SM condition were taught how to self-monitor their exercise and BG, to goal set, and to use CGM to observe how exercise influences BG. We hypothesized that compared with the CON condition, using a real-time CGM would facilitate self-monitoring behavior, resulting in increased exercise adherence.
Results:
Repeated-measures analysis of variance revealed significant Condition × Time interactions for self-monitoring (P < 0.01), goal setting (P = 0.01), and self-efficacy to self-monitor (P = 0.01), such that the SM condition showed greater increases in these outcomes immediately after the program and at the 1-month follow-up compared with the CON condition. The SM condition had higher program attendance rates (P = 0.03), and a greater proportion of participants reregistered for additional exercise programs (P = 0.048) compared with the CON condition. Participants in both conditions experienced improvements in health-related quality of life, waist circumference, and fitness (P values <0.05).
Conclusions:
These findings provide promising initial support for the use of a real-time CGM to foster self-monitoring and exercise behavior in individuals living with prediabetes or T2D.
Background
I
Acute bouts of aerobic exercise increase uptake of glucose into muscles, glucose tolerance, and insulin action, all of which lead to better control of BG levels for up to 72 h. 4 –8 In addition to these acute benefits, regular participation in exercise is associated with improvement in insulin sensitivity, even after the residual benefits of a single exercise bout on insulin sensitivity have worn off. 9,10 For people with prediabetes, participation in regular aerobic exercise can delay or even prevent the onset of T2D. 11 –13 Exercise as part of a lifestyle modification program has been found to reduce the risk of developing T2D by 58%. 14 Despite the summative evidence that individuals with T2D or prediabetes can manage and prevent their disease through exercise, individuals with diabetes are 19% less physically active than those without diabetes. 15
Of the few exercise interventions aiming to increase long-term adherence that have been conducted in people with T2D, those that included components of social cognitive theory 16 –18 (SCT) were more successful at increasing exercise adherence than interventions grounded in other theories 19,20 and atheoretical interventions. 21 Group-mediated cognitive–behavioral (GMCB) interventions, which are interventions rooted in SCT, have proven particularly successful at increasing exercise adherence rates in people facing similar exercise barriers to those faced by people with T2D and prediabetes. 22 –25
GMCB interventions target behavior change by teaching self-regulatory skills in a group setting. 22 –25 “Self-regulation” is a key component of SCT, involving a set of acquired skills that enables an individual to exert control over his or her thoughts, feelings, motivation, and actions. With respect to exercise, use of self-regulatory skills is an integral component to adherence. 26 –28 GMCB interventions utilize social processes, motivation, and support derived from the group to foster commitment to exercise from all group members. 22 Through the gradual transition of participants from the group physical activity setting to independent physical activity, the GMCB intervention model ensures participants do not become dependent on peers or staff. The primary goal of GMCB interventions is to produce individuals who engage in long-term exercise behavior without the help of the group or interventionists (i.e., independent exercisers).
Self-monitoring is a self-regulatory skill that is particularly relevant to individuals with prediabetes or T2D, as self-monitoring blood glucose (SMBG) is essential in the management of these conditions. Self-monitoring and observing discrepancies in one's behavior in comparison with a personal standard are believed to motivate corrective changes in behavior. 29 In this way, goal setting is inescapably intertwined with the skill of self-monitoring. To ensure consistent self-monitoring behavior, it is furthermore important that individuals feel confident in their ability to self-monitor (i.e., they hold high self-efficacy beliefs). Self-efficacy beliefs predict whether goals are set and how challenging these goals are 30 and are considered the most robust predictor of future exercise behavior. 31 –33 The two most influential sources of self-efficacy are performance accomplishments and vicarious experiences. 31 Providing opportunities for participants to experience successful self-monitoring events, as well as providing accounts of others' self-monitoring experiences, will serve to bolster individuals' self-efficacy to self-monitor. Given the generalizability of self-efficacy to similar tasks, providing self-monitoring practice through SMBG should promote mastery of how to self-monitor exercise behavior (SMEB), although this has yet to be tested.
Exercise is highly effective at decreasing variability and blunting the magnitude of BG “spikes” and “dips,” but traditional point-in-time fingertip BG assessments are not able to pick up these improvements. With the advent of real-time feedback continuous glucose monitors (CGMs), individuals are able to observe their BG every 5 min through a linked monitor and thus observe the extended benefits that a single bout of exercise has on BG control. 34 –36 As mastery experience is hypothesized to be the strongest source of self-efficacy, observing the benefits of exercise in oneself is likely to be more powerful than merely being shown hypothetical data. 31 Using a real-time CGM to teach participants how to SMBG and how to recognize patterns in BG following exercise may be an effective means for increasing exercise levels and improving exercise adherence.
The purpose of this pilot study was to test the feasibility of an 8-week GMCB structured intervention to teach people with prediabetes and T2D how to SMEB and SMBG using real-time CGMs. In conjunction with SMEB, participants were taught how to set exercise-related goals.
When compared with a standard care exercise program (CON condition), it was expected that participants in the self-monitoring exercise intervention (SM condition) would report greater increases in SMEB and SMBG, as well as goal-setting behaviors across time. Furthermore, it was hypothesized that participants in the SM condition would experience greater increases in self-efficacy to SMEB compared with participants in the CON condition. Consequently, as a result of increased self-monitoring and goal-setting behaviors and self-efficacy to SMEB, it was hypothesized that the SM participants would experience greater increases in exercise behavior and intentions to exercise at (1) the end of the 8-week intervention and (2) after 1 month with no contact from the researcher. Lastly, it was hypothesized that as a result of the 8-week exercise program all participants, regardless of condition, would experience improvements in health-related quality of life (HRQL), body mass index, waist circumference, and fitness immediately postprogram.
Materials and Methods
Participants
Thirteen participants were recruited from two sessions of a community exercise program. Using a quasi-experimental design, separate sessions were assigned as the CON condition (n = 7; mean age, 61.14 ± 8.38 years) and the SM condition (n = 6; mean age, 63.50 ± 4.32 years). In each condition participants were primarily female (CON, 71%; SM, 83%), mainly identified as white (CON, 71%; SM, 83%), had completed some form of postsecondary education (CON, 71%; SM, 67%), and were not working at the time of the study (CON, 86%; SM, 83%). The inclusion criteria included the following: (1) between the ages of 18 and 75 years old, (2) having prediabetes (a glycosylated hemoglobin score between 5.7% and 6.4% 37 ) or T2D (a glycosylated hemoglobin score above 6.4% 37 ), (3) ability to read and write English at a grade 6 level or higher, and (4) score at least 24 on the Mini Mental State Examination. Diabetes status was either physician diagnosed or, if unknown, determined using a glycosylated hemoglobin test. In both conditions the majority of participants had T2D (CON, n = 5; SM, n = 5).
Measures
Self-monitoring and goal setting
An exercise-specific self-regulation measure was selected to assess participants' use of (1) SMEB and (2) goal-setting strategies. 38,39 Responses were reported on a 5-point Likert scale ranging from 1 (“never”) to 5 (“very often”). Cronbach α values for prescores were as low as 0.19, and therefore for analytic purposes Week 2 scores were substituted for baseline. 40 Internal consistencies have been demonstrated to be acceptable in previous research with Cronbach's α values ranging from 0.74 to 0.87. 39
Additional questions were devised to assess the frequency that participants self-monitored in the past week. Specifically, separate questions relating to SMEB and SMBG asked participants: “In the past 7 days how many times did you self-monitor your behavior?” Self-monitoring and goal setting were assessed at seven time points. The first six time points coincided with before and after participants in the SM group wore the CGM, and the last measurement was at the 1-month follow-up.
Self-efficacy
To measure self-efficacy to SMEB, two context-specific items were developed. Participants were asked the following: “In the next 7 days how confident are you that you can (1) record your exercise bouts and (2) keep track of how many times you exercise and adjust your behavior accordingly.” Confidence was rated on an 11-point Likert scale with anchors ranging from 0% (“not at all confident”) to 100% (“extremely confident”). Self-efficacy was assessed at pre-, mid-, and postexercise program and at the 1-month follow-up.
Exercise attendance and reregistration for an exercise program
Participant attendance was recorded each class by the researcher and calculated as a percentage of classes attended. At the end of the 8-week program the proportion of participants from each condition who registered for a new exercise program at the same facility, on their own accord, was also recorded.
7-Day Physical Activity Recall Questionnaire
Exercise behavior was measured using the 7-day Physical Activity Recall Questionnaire 41 (7-day PAR) at pre-, mid-, and postprogram and at the 1-month follow-up. Participants reported all purposeful exercise within the past week that was sustained for a minimum of 10 continuous min. For the purpose of this study only minutes of exercise spent in moderate or higher intensities were analyzed. Total exercise and independent exercise were separated, with independent exercise referring to exercise only performed outside of the exercise classes. Data collected from this questionnaire have demonstrated evidence of validity and reliability. 42,43
HRQL
The Short Form 36 Health Survey 44 (SF-36) is designed to assess HRQL. It is divided into a physical component summary and a mental component summary. Extensive data have been published verifying the psychometric and clinical validity of this instrument and its utility for assessing HRQL following physical activity interventions. 45 –47 We assessed HRQL before and directly postprogram, as well as at the 1-month follow-up, using the SF-36.
Physical outcomes
Body mass index and waist circumference were assessed by certified staff at the fitness facility at pre-, mid-, and postprogram. Waist circumference was taken following the CPAFLA protocol. 48 To test for cardiovascular fitness, participants performed the 6-min walk test pre- and postprogram. 49 The 6-min walk test is a validated test often used in samples of elderly adults with multiple comorbidities. 50 –53
Follow-up interview
A follow-up interview consisting of open-ended questions was administered to each participant by phone 1 week after the last class of the exercise program. During the interview all participants were asked about what they learned during the 8-week exercise program. For participants in the SM condition there were additional questions about the feasibility of wearing a CGM and its utility for SMBG.
Procedures
Ethical approval for this study was obtained through the University of British Columbia's Clinical Research Ethics Board (protocol H13-00648).
Exercise program
Participants in both conditions (CON, SM) attended the same exercise program two times per week for 8 weeks. Each class lasted approximately 90 min. The first 45 min consisted of a guided exercise session (30 min of aerobic activity, 10 min of resistance training, 5 min of stretching), and the last 45 min consisted of an educational tutorial. In both sessions the researcher led six of the tutorials to ensure equal researcher contact time between the two conditions. Exercise facility staff or healthcare professionals led all other tutorials, and similar content was covered between conditions. Questionnaires were administered following the tutorials with the exception of the 1-month follow-up questionnaire, which was mailed or hand-delivered to participants depending on their preference 1 month after the last exercise class.
Standard care (CON) condition
Throughout the CON session, the researcher discussed an assortment of general health topics, including the impact of stress on health, abdominal adiposity, dietary fiber, the importance of sleep, mental health, and flu vaccinations.
Self-monitoring intervention (SM) condition
Participants in the SM condition wore the CGM at three time points throughout the 8-week program—specifically, Week 1, Week 4, and Week 7—for 5 consecutive days on each occasion. A “Real-time” CGM with a Sof-sensor® and MiniLink™ transmitter was used (Guardian® REAL-Time continuous glucose monitoring system; Medtronic MiniMed, Inc., Northridge, CA), which provided each participant with an electronic monitor showing his or her current estimated BG and a visual graph of the estimated BG over the past 24 h.
Educational tutorials
The six tutorials led by the researcher in the SM condition focused on teaching participants two self-regulatory skills: self-monitoring and goal setting. Participants were taught about BG and the importance of controlling BG levels. Specifically, participants were informed of the adverse health effects that might result from uncontrolled BG levels. Each time participants wore the CGM they were instructed to monitor and record their BG levels four times a day in a logbook provided by the researcher. Next, setting exercise goals was taught following the “SMART” principle (Specific, Measurable, Attainable, Realistic, Time-frame oriented). The logbooks provided by the researcher had sections for participants to record their exercise goals. In an attempt to foster greater group cohesion, the researcher also helped participants collectively decide on a group exercise goal that was tracked throughout the program. Participants were instructed to record all of their exercise bouts in their logbooks and taught how SMEB could help them adhere to an exercise routine. To further demonstrate the relationship between exercise and BG control, participants were supplied with a printout of their own CGM graph to highlight how exercise improved their BG control. Tutorials also included group discussions about participants' experiences SMEB and SMBG. At the end of the 8-week program, participants were provided with a new logbook where they could continue to make exercise goals and record their exercise bouts for the following month independently.
Statistical analyses
For the main analyses we used mixed model multiple analyses of variances (MANOVAs) and analyses of variance (ANOVAs) to test the effect of condition by time on each outcome variable: self-monitoring, goal setting, self-monitoring frequency, self-efficacy to self-monitor, and exercise minutes. For HRQL and physical variables, repeated-measures ANOVAs and t tests were used to test for changes across time; these variables were not tested between conditions. All effects were tested as significant at P < 0.05. However, in light of the small sample size and exploratory nature of this feasibility study, we chose a priori to allow for further analysis of all effects at the P ≤ 0.10 level, in conjunction with a heavier reliance on interpretation of effect sizes rather than significance levels.
Follow-up interviews were recorded by audiotape and transcribed verbatim. The transcripts were coded into categories, and emerging themes within categories were identified by K.J.B. and confirmed by M.E.J. The transcripts were analyzed for content and frequency of responses.
Results
There were no statistical differences between conditions regarding demographic or baseline variables.
Intervention fidelity
In the SM condition logbooks were analyzed as a manipulation check. Participants demonstrated high compliance with recording BG levels (mean, 90.43% complete; SD, 12.14%). SM participants were also required to create new exercise goals weekly. An exercise goal was considered complete if it specified a measurement of volume of exercise per week. On average, during the intervention participants recorded their exercise goals 75.00% (SD, 22.36%) of the weeks, but at the 1-month follow-up the percentage of weekly goals completed decreased to 37.50% (SD, 37.91%). Lastly, at the end of each week SM participants were instructed to tally their exercise minutes. During the intervention and the 1-month follow-up participants recorded a tally of their exercise minutes: means of 60.00% (SD, 28.28%) and 50.00% (SD, 41.83%) of the weeks, respectively.
Self-monitoring and goal setting
To examine differences in SMEB and goal setting between conditions, a 2 (condition: CON, SM) ×6 (time: Week 2, Week 4, Week 5, Week 7, post, follow-up) repeated-measures MANOVA was performed for the outcome variables SMEB and goal setting. The overall multivariate effect for the Condition × Time interaction (F 15, 150 = 1.63, P = 0.07) was not significant, but as it was associated with a P value of ≤0.10, further exploration was warranted. Follow-up univariate analyses revealed a significant Condition × Time interaction for SMEB scores (F 5, 50 = 4.63, P < 0.01, partial η 2 = 0.32) and goal setting scores (F 5, 50 = 3.29, P = 0.01, partial η 2 = 0.25). These represent large effects, and examination of the means revealed that the SM condition showed greater increases in SMEB and goal setting than the CON condition (Table 1).
Data are mean (SD) values.
Significant difference between conditions (P < 0.05) at indicated time point.
Conditions were combined for health-related quality of life (HRQL) scores.
CON, standard care exercise program; SM, self-monitoring exercise program.
To examine differences in the frequency that participants self-monitored between conditions, a 2 (condition: CON, SM) ×7 (time: pre, Week 2, Week 4, Week 5, Week 7, post, follow-up) repeated-measures MANOVA was performed for frequency of (1) SMEB and (2) SMBG. There was an overall significant Condition × Time interaction (F 12, 120 = 3.48, P < 0.01). Univariate follow-up analyses revealed interaction effects for frequency of SMEB (F 1.97, 19.68 = 4.07, P = 0.03, partial η 2 = 0.29) but not frequency of SMBG (F 2.01, 20.05 = 3.29, P = 0.06, partial η 2 = 0.25). These effect sizes are interpreted as large effects. Comparison of means indicates that the SM condition reported greater increases in frequency of SMEB compared with the CON condition (Table 1).
Self-efficacy to self-monitor exercise
To examine changes in self-efficacy to SMEB, a 2 (condition: CON, SM) ×4 (time: pre, mid, post, follow-up) repeated-measures ANOVA was conducted. Results revealed a significant Condition × Time interaction (F 3, 27 = 4.42, P = 0.01, partial η 2 = 0.33). This effect size is indicative of a large effect, and similar to previous results, examination of the means revealed that the SM condition had greater increases than the CON condition (Table 1).
Exercise
Attendance and future registration for an exercise program
An independent-samples t test was used to compare the mean attendance rate between conditions. On average, participants in the SM condition attended a significantly greater percentage of classes (mean, 96.88%; SD, 5.23) than those in the CON condition (mean, 84.70%; SD, 11.22) (t 11 = 2.43, P = 0.03, d = 1.39). This effect size is suggestive of a very large effect. A χ2 test was used to assess the relationship between study condition and reregistering for a new exercise program at cessation of the 8-week exercise program. There was a significant association between condition and whether participants reregistered [χ2(1) = 3.90, P = 0.048]. The odds of reregistering were 12.50 times higher if participants were in the SM condition compared with the CON condition.
7-day PAR
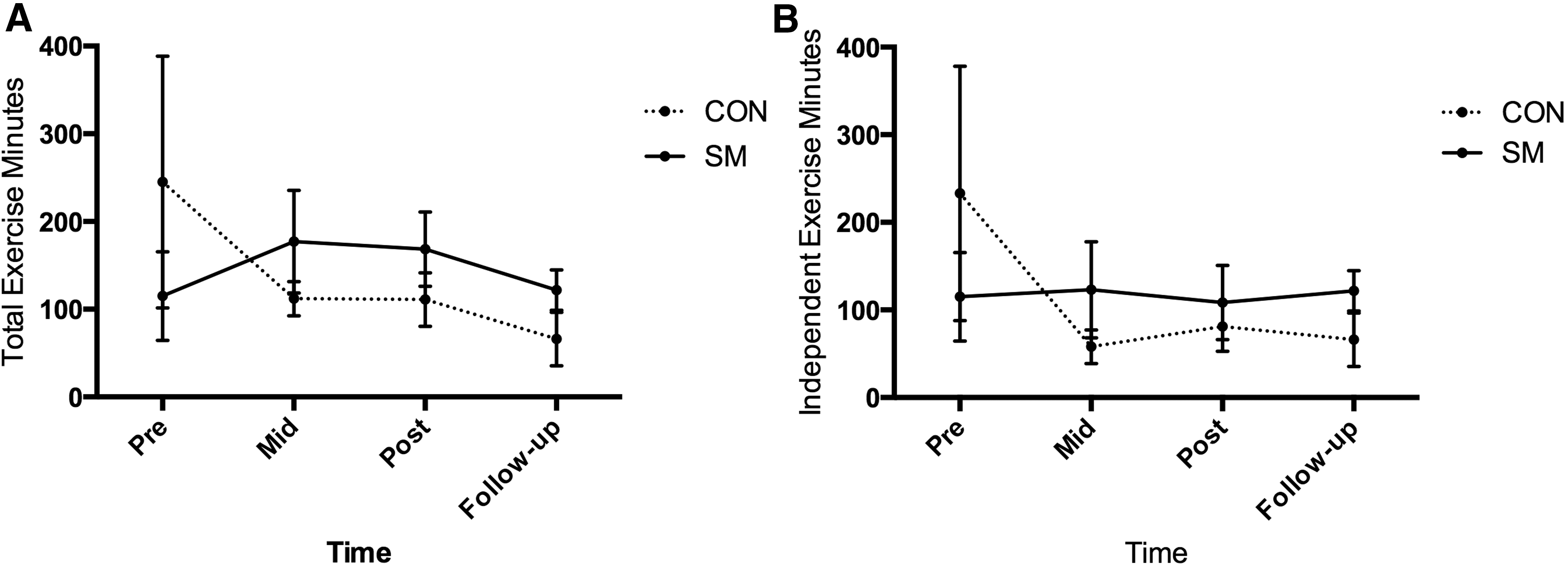
A series of 2 (condition: CON, SM) ×2 (time) repeated-measures ANOVAs were conducted to assess differences between conditions for minutes of exercise pre- to postprogram and preprogram to follow-up. Cohen's d was calculated using the difference score from pre- to postprogram and preprogram to follow-up. These analyses were run separately for total exercise and independent exercise. Figure 1 gives a visual depiction of changes in exercise levels over time.
1. Total exercise. There were no significant Condition × Time interactions for total exercise minutes from pre- to postprogram (F 1, 7 = 0.42, P = 0.54, d = 0.411) or preprogram to 1-month follow-up (F 1, 7 = 0.85, P = 0.39, d = 0.59). However, interpretation of the effect sizes suggests there were small- to medium-sized effects with greater increases in exercise levels observed in the SM condition compared with the CON condition.
2. Independent exercise. There were no significant Condition × Time interactions for independent exercise minutes from pre- to postprogram (F 1, 7 = 0.04, P = 0.84, d = 0.13) or preprogram to 1-month follow-up (F 1, 7 = 0.47, P = 0.52, d = 0.44). The effect size for pre- to postprogram suggests that there was no effect. However, for preprogram to follow-up there was a small- to medium-sized effect with a greater increase in exercise observed in the SM condition compared with the CON condition.
Mean changes between conditions in
HRQL
A repeated-measures (time: pre, post, follow-up) MANOVA was conducted to examine the physical and mental subscales of HRQL. The overall multivariate effect for time was not significant (F 4, 48 = 2.06, P = 0.10). However, as outlined in our statistical plan, analyses associated with a P value of ≤0.10 were worthy of further exploration. Univariate analyses revealed a significant main effect of time for the mental summary scale (F 2, 24 = 3.51, P = 0.046, partial η 2 = 0.23) but not the physical summary scale (F 2, 24 = 2.42, P = 0.11, partial η 2 = 0.17). Despite a P value of >0.05 for the physical summary score, effect sizes are indicative of large effects for both the mental and physical summary scores, and observation of the means suggests HRQL increased over time in both conditions (Table 1).
Physical outcomes
A repeated-measures (pre, mid, post) ANOVA revealed no significant decreases in body mass index over time (F 1.23, 12.25 = 3.83, P = 0.07, partial η 2 = 0.28); however, with a P value of <0.10, further exploration was conducted. Post hoc tests revealed no significant differences in body mass index across time (pre- to midprogram, P = 0.08; pre- to postprogram, P = 0.07). An additional repeated-measures (pre, mid, post) ANOVA examining waist circumference revealed a significant main effect of time (F 2, 20 = 5.74, P = 0.01, partial η 2 = 0.37). Post hoc analyses found that waist circumference decreased from pre- (mean, 109.73 cm; SD, 18.86) to midprogram (mean, 107.21 cm; SD, 16.58) (t 11 = 3.04, P = 0.010), as well as from pre- to postprogram (mean, 106.69 cm; SD, 16.71) (t 11 = 2.64, P = 0.02). Lastly, a paired-samples t test was used to examine changes in meters walked during the 6-min walk test, revealing a significant increase from pre- (mean, 375.23 m; SD, 118.65) to postprogram (mean, 478.53 m; SD, 126.84) (t 12 = 1.78, P = 0.01).
Follow-up interview
Emerging themes elicited from the exit interview are detailed below:
“What I have learned…”
Within the CON condition, one participant revealed how he came to recognize an association between exercise and blood sugar, stating “I go to exercise and my blood sugar goes up,” whereas another recalled learning about sleep. These were the only two outcomes that CON participants reported learning during the program. Conversely, in the SM condition, multiple themes emerged from participants' responses. The importance of exercise in lowering BG was the most frequently reported outcome learned in the intervention (n = 3): “the learning of wearing that monitor, and how exercise can bring down the diabetes.” In addition, participants recalled learning how to plan for exercise (n = 1), patterns of BG fluctuation (n = 1), and the importance of eating a healthy diet (n = 2).
“What I incorporated into my life…”
Participants in both conditions commonly cited exercise as something that they have incorporated into their own lives (CON, n = 3; SM, n = 4). In contrast, only participants in the SM condition spoke specifically about trying to exercise most days of the week. For example, one participant in SM described, “I try to do something everyday…. I'm at the pool three times a week but not on the weekends so I try and go out for a 20-minute pole walk.”
CGM feasibility and utility for SMBG
In addition to specific topics covered during the program, SM participants were asked to report on the experience of wearing the CGM. Three participants said they would wear the CGM again, two participants said they would wear it again if the device could be inserted completely subcutaneously, and one participant said he would not wear the device again.
Benefits
All participants were in agreement that this was important to be able to view their BG levels constantly throughout the day. Participants reported that being able to see their BG was convenient, informative, and reassuring; “It took away a lot of my anxiety… it gave me reassurance, especially because my [glucose] levels are all over the place and so it helped me realize if I was high or low.” Participants reported preferring the CGM to traditional BG monitoring methods because they did not have to perform as many painful finger prick blood samples.
Interference with daily living and ease of use
Issues identified as interfering with normal activities of daily life included interrupted sleep (n = 1), difficulty showering (n = 1), and not being able to go in the hot tub (n = 1). Participants had no trouble understanding the BG graphs created by the CGM devices or difficulty using the CGM (e.g., knowing which buttons to press).
Value for behavior change
A recurring theme that emerged was that the BG feedback from the CGM was a valuable tool for influencing decisions regarding diet and exercise. The majority of participants said that seeing the BG graphs in response to what they were eating impacted the foods they chose to eat (n = 5). One participant explained, “It was good to see it right in front of you, you couldn't deny it, the evidence was right there… don't eat gummy bears.” Two participants said observing improvement in their own BG control following exercise made them consider exercising more days of the week: “On the weekend when I have 2 days off from exercising I did know my BG went up a bit… I could have gone out for a walk.”
Discussion
Few past exercise interventions have isolated and targeted individual self-regulatory skills. 19,20,54 This is problematic as we are not able to tease apart which skills are most effective at changing behavior. The purpose of this pilot study was to isolate and teach participants self-monitoring and goal-setting skills as a means of increasing exercise behavior and exercise adherence. We found significant increases in the use of both skills for individuals who received the self-monitoring intervention compared with the standard care condition, and these increases were evident after a single, brief 45-min tutorial. We also found that individuals in the SM condition reported greater frequency of SMEB compared with those in the CON condition at all assessment points following baseline. This is a promising finding given that the frequency that an individual self-monitors his or her behavior has been highlighted as the most important aspect of self-monitoring for behavior change. 55
Despite increases in SMEB frequency during the intervention, the frequency of SMEB in the SM condition decreased from an average of six times per week to fewer than three times per week at the 1-month follow-up. This is in line with previous research that assessed SMEB frequency within a pedometer intervention in which participants were required to record their daily step count. 21 Tudor-Locke et al. 21 reported that the percentage of days participants reported their step count dropped from 100% during the intervention to 58% during the last 4 weeks of an adherence phase. Previous GMCB interventions emphasize a need for the number of group exercise sessions to be gradually reduced as participants begin to attempt to engage in independent exercise. Unfortunately, we did not have control over the exercise class schedule; however, including a transition period may improve adherence during follow-up, and this should be considered for future interventions.
Self-efficacy is theorized to be one of the strongest predictors of future behavior, and in order to maintain increases in self-monitoring behavior, it is therefore necessary that participants' self-efficacy to self-monitor is high. 31 Our findings supported our hypothesis with individuals in the SM condition reporting greater increases in self-efficacy to self-monitor exercise compared with those in the CON condition.
Self-regulatory efficacy (such as self-monitoring self-efficacy) has consistently been shown to be a better predictor of future exercise behavior than task self-efficacy. 33,56 –59 For example, a study assessing different types of self-efficacy during a cardiac rehabilitation program found that self-regulatory self-efficacy accounted for more variance in attendance to the exercise program than task self-efficacy (i.e., walking self-efficacy). 28 In line with the study of Woodgate et al., 28 the current findings revealed that participants in the SM condition, who reported greater use of self-regulatory skills and higher levels of self-regulatory self-efficacy, attended a greater percentage of the exercise classes. Dropout rates for exercise programs in populations with chronic disease typically range from 40% to 50% within the first 6–12 months. 60 Intervention models that promote high attendance rates are therefore quite valuable.
Unique to the present study was our measurement of registration for future exercise programs as an indirect measure of an intention to continue exercising. We found that the odds of registering for a future exercise program were approximately 12 times higher if participants were in the SM condition compared with the CON condition.
With respect to exercise findings from the 7-day PAR questionnaire, because of the small study sample size and large SDs common in exercise, a heavy reliance was placed on the interpretation of effect sizes. Although not statistically significant, the magnitude of difference between conditions for changes in total exercise from pre- to postprogram and preprogram to 1-month follow-up were consistent with Cohen's definition of small- to medium-sized effects. 61 In both cases, participants in the SM condition reported greater positive changes in exercise than those in the CON condition. More predominant effects of condition for exercise minutes were evident at follow-up than directly postintervention, consistent with previous GMCB interventions. 22,23 One of the biggest advantages of GMCB interventions is their ability to help participants maintain exercise levels once the structured exercise program has ended.
There are only a few exercise interventions that have used cognitive–behavioral strategies in an attempt to improve exercise adherence in individuals with T2D or prediabetes postintervention. The few previous interventions that have successfully led to increases in exercise adherence were conducted using one-on-one counseling sessions. 17,19 Group-based interventions may be more time- and cost-efficient. As well, through the opportunity for social interactions a group setting may provide mental health benefits in addition to physical benefits. In the present study participants' perceived mental health improved in both conditions, in line with findings from previous studies assessing group exercise programs. 62,63 Rates of depression are especially high in people with diabetes (24% vs. 17% in the general population 64 ), and an exercise program that can improve perceived mental health therefore has meaningful implications. There were not significant changes in physical HRQL; however, there was a large corresponding effect size (partial η 2 = 0.17). There is support in the literature for the proposal that higher levels of physical activity are associated with higher HRQL scores, for both the physical and mental components. 65 –67
Regarding changes in anthropometrics and fitness, in support of our hypotheses we noted improvements in waist circumference and fitness following the 8-week exercise program. Decreases in waist circumference are largely in contrast with previous studies that have found only modest to nonsignificant changes following an exercise intervention. 68,69 It has been speculated that without the addition of dietary or drug interventions, exercise alone cannot create enough of an energy deficit to lead to anthropometric changes. 70 Our results suggest otherwise and are a testament that the exercise classes provided must have been led at a relatively high intensity for participants. These changes in anthropometrics, in combination with the positive increases in fitness, provide strong support that participants in both conditions were engaging in increased levels of exercise from pre- to postprogram.
The current study had several strengths. It was the first study to test the usability of a real-time CGM as a tool to change exercise behavior in individuals with T2D and prediabetes. Overall, participants strongly valued the BG information that the CGM provided and reported that it had a positive impact on their exercise and diet choices. It was also the first study to use a GMCB structured intervention in an attempt to change exercise behavior in people with T2D and prediabetes. This is a population in desperate need of interventions that are successful at helping them maintain changes in exercise behavior. Lastly, this intervention has high external validity as it was implemented within an established community exercise center for people with chronic disease. The setting and sample were both highly representative of a typical beginner exercise program in North America. As a result, the intervention can be easily translated into practice in similar settings with a high likelihood of success.
In addition to the strengths, there were also limitations to the present study. First, this study was a priori designed and funded as a feasibility study. As a result, the most predominant limitation was that the small sample size precluded advanced statistical analyses, such as testing for mediating variables. Second, despite the promising effect sizes, use of the 7-day PAR as the primary assessment of exercise behavior change may have been a limitation in this sample due to floor effects. 71 For example, one participant who had not increased her exercise levels according to the 7-day PAR assessment still felt that she had been exercising more because she had been using canes instead of her walker when moving. Future research could make use of motion sensors as a means of assessing physical activity behavior. 71 Despite their own drawbacks, including cost, motion sensors may be more sensitive to minor changes in exercise behavior.
Findings from the present research support the hypothesized relationship that Bandura 16 posited in SCT for the use of self-regulatory skills and behavior change. Findings also provide preliminary evidence that, for individuals with T2D and prediabetes, a GMCB intervention that teaches how to self-monitor can be beneficial for increasing and maintaining exercise behavior. With regard to CGM usage we demonstrated that a real-time CGM may be useful for motivating lifestyle changes in people with prediabetes and T2D.
Considering the epidemic proportions of Canadians living with T2D or prediabetes, as well as the vast benefits that exercise can provide in managing these conditions, implementation of self-monitoring interventions that utilize self-monitoring tools in group-based exercise programs may be a promising avenue to explore in communities across North America.
Footnotes
Author Disclosure Statement
No competing financial interests exist.