
Abstract
Background:
Sulfonylureas are widely used to treat type 2 diabetes (T2DM). Although genetic variations are associated with sulfonylurea treatment responses in T2DM patients, whether these variations can be used to predict heterogeneous treatment responses is unclear. In this study, we assessed the potential utility of combining information from multiple variants and phenotypes to predict sulfonylurea response.
Methods:
Using data from the “Glibenclamide” arm (365 patients) of the Xiaoke Pill Trial that evaluated the safety and efficacy of sulfonylurea, we identified genetic variants associated with sulfonylurea treatment response, and we explored their ability to predict drug response when combined with phenotype information.
Results:
The association of 780 single-nucleotide polymorphisms (using Infinium HD iSelect chip) with drug efficacy was evaluated, and four genes identified with drug metabolism (FMO2, FMO3, UGT2B15, and CYP51A1, P < 0.05) were found to be associated with changes in HbA1c. In a clinical model, the baseline values of HbA1c and disposition index (DI) were significantly associated with HbA1c and fasting plasma glucose (FPG) target achievements. Compared with clinical models, the inclusion of genetic markers significantly increased the predictive ability for both HbA1c- and FPG-based outcomes.
Conclusions:
Our findings suggest that altered protein function in multiple pathways may cooperatively contribute to the increased discrimination by area under receiver operating curve for T2DM patients, and it may explain, in part, the relationship between inter-individual variability and the sulfonylurea response.
Introduction
S
Relative to metformin and other anti-diabetes drugs, sulfonylureas have been associated with an increased risk of hypoglycemia and diabetes-related mortality; however, they are prescribed to about 25%–40% of T2DM patients in both developed and developing countries. 4,5 Studies from nationally representative primary care databases suggest that among T2DM patients, ∼35% in the United States and 46% in England use sulfonylurea, and more than 600,000 prescriptions for sulfonylureas are dispensed monthly in England. 4,6
Sulfonylureas stimulate endogenous insulin secretion via their action on the KATP channel in the plasma membrane of pancreatic β-cells. 2 When used either as a monotherapy or in combination with other anti-diabetes drugs, sulfonylureas lowered HbA1c levels by 1.25%–2.24%. 7 However, higher sulfonylurea doses were not associated with a greater reduction of HbA1c, 7 and they had a higher level of heterogeneity in terms of treatment response, such that a significant proportion of T2DM patients do not respond to sulfonylurea treatment. 8 Notably, 5%–7% of patients who initially respond to sulfonylurea therapy did not achieve targeted levels of fasting plasma glucose (FPG) or HbA1c after long-term follow-up. 9
Clinical and genetic factors have been used to predict sulfonylurea responses of T2DM in a number of studies. The HbA1c and FPG levels at treatment initiation were shown to be significant indicators of treatment response to sulfonylurea therapy (Hirst et al., 2013). 7 However, in a homeostatic model analysis of insulin secretion: the Homeostasis Model Assessment of beta cell function (HOMA-β), a model fasting plasma insulin to glucose ratio was a better predictor of secondary sulfonylurea failure than other clinical indices, including HbA1c and the Homeostatis Model Assessment of Insulin Resistance (HOMA-IR). 10
Previous pharmacogenetic studies reported genes that are associated with sulfonylurea efficacy, 8,11 –20 and they also indicated that single-nucleotide polymorphisms (SNPs) within several genes affect pharmacokinetics or β-cell function. Genetic variants, including KCNJ11, ABCC8, IRS1, TCF7L2, KCNQ1, and CDKAL1, were found to affect pharmacokinetics and/or pharmacodynamics of sulfonylureas. Interestingly, diabetes-associated gene loci have modestly sized effects, ranging from 1.37 for SNPs in TCF7L2 21 to 1.09 for SNPs in ADAMTS9. 22 In contrast, the magnitude of effects for pharmacogenetic loci identified to date is much higher, ranging from 3.44 for SNPs in CYP2C9 23 to 1.36 for SNPs in CDKN2A/2B. 15 These results raise the question of whether information regarding genotype would be useful to predict the likelihood of sulfonylurea efficacy.
Although several pharmacogenetic studies have been conducted to identify genetic factors associated with treatment success for sulfonylurea and other anti-diabetes drugs, we are not aware of any study that evaluated whether knowledge of genetic markers can provide value in terms of predicting the glycemic response in patients treated with sulfonylurea.
Since genetic factors are relatively stable throughout an individual's lifetime, identifying genotypes that affect sulfonylurea efficacy and considering them either on their own or in combination with phenotype(s) might improve drug efficacy prediction, particularly if the genotypes highlight differences in the activity of pathways that are not measured in non-genetic risk models. Using 1-year follow-up data from a Phase 3 clinical trial involving Chinese T2DM patients, we (i) screened for SNPs associated with sulfonylurea efficacy using a gene chip method, and we (ii) assessed the potential utility of combining information from multiple variants and phenotypes to predict drug response.
Methods
Study population
Data for this study were obtained from the “Glibenclamide” arm of the Xiaoke Pill Trial, which is described in detail in Ji et al. 24 Briefly, the study was a controlled, double-blind, multicenter, non-inferiority trial that included 800 T2DM patients. The trial compared the safety and efficacy of the Xiaoke Pill (combination of glibenclamide and traditional Chinese Medicine [TCM]) with that of glibenclamide. The enrolled subjects were divided into two arms: Xiaoke Pill arm (n = 400, treated with Xiaoke Pill or Xiaoke Pill plus metformin) and the Glibenclamide arm (n = 400, treated with glibenclamide monotherapy or glibenclamide plus metformin).
All patients from the Glibenclamide arm who completed the 48 week follow-up were selected for this study. The sample size was 365 patients (Metformin group: n = 182, Treatment naïve group: n = 183). The glibenclamide doses were consistent and similar between the two groups during the 48 week follow-up, and the metformin dose was the same for all individual patients throughout the follow-up period. 24
Three outcomes were evaluated for glibenclamide efficacy: (1) HbA1c < 6.5% (48 mmol/mol); (2) FPG <7 mmol/L at 1 year from baseline; and (3) change in FPG at 1 year from baseline in accordance with the trial endpoints.
The protocol was approved by the Ethics Review Committee affiliated with each study center, and it was implemented in accordance with the provisions of the Declaration of Helsinki and Good Clinical Practice guidelines. All participants provided written informed consent to participate in this study.
Phenotype measurements
Details of phenotype measurements during study visits were described in Ji et al. (2013). 24 Patient body weight, blood pressure, and FPG values were measured monthly. Lipid, HbA1c, C-Peptide, C-reactive protein (CRP), adiponectin, and insulin levels were measured during each quarterly visit from the time of randomization. HOMA-IR and HOMA-β were calculated as previously described. 24 The disposition index (DI) was calculated using the formula: HOMA-β × (1/HOMA-IR). 25
Sample analysis for genetic markers
Infinium HD iSelect chips were used for patient genotyping. SNPs were selected according to pharmacokinetics and pharmacodynamics. The selection of SNPs for the pharmacokinetic study was based on a specific chip for pharmacogenetic studies (Drug Metabolizing Enzymes and Transporter, DMET™; Affymetrix) that included 1936 SNPs (
Statistical Methods
Basic statistics on study parameters are presented as number (%), mean (standard deviation), or median (interquartile range), as appropriate. The distributions of changes in FPG and HbA1c (by metformin and drug naïve group) at the 1-year timepoint, along with the baseline distribution of these glycemic parameters are presented as kernel density plots. The outcomes for this study were HbA1c < 6.5% (48 mmol/mol) and FPG <7 mmol/L at 1 year, and change in FPG at 1 year from baseline. The possible association of all SNPs with these three outcomes was initially evaluated using standard statistical techniques, including the statistical feature selection method (based on F-test), with adjustments for multiple testing.
To evaluate the predictive ability of the relevant phenotypes either alone or with the SNPs that were significantly associated with categorical outcomes, multivariate logistic regression models were fitted. The robust multivariate regression model was used for the continuous outcome of change in FPG at 1 year. The phenotypes added in the multivariate models were as follows: age at randomization, sex, metformin use, and baseline values for C-peptide, DI, body weight, and FPG or HbA1c, as appropriate. The DI is the product of insulin secretion and insulin sensitivity and is considered the gold standard for measuring beta-cell function. The significance levels (P values) were estimated using robust estimates of regression coefficient standard errors.
To compare the model fits between the full model (phenotypes+SNPs) and the clinical model (phenotypes only), Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC) were used. Smaller estimates for the information criteria indicated a stronger fit. To compare the predictive ability of the phenotypes alone and the phenotypes plus the genetic markers, the non-parametric area under the receiver operating curve (AROC) was estimated and compared using appropriate statistical tests.
Results
AROC was used to evaluate the predictive ability of SNPs together with the categorical primary outcome phenotypes (HbA1c < 6.5% and FPG <7 mmol/L). The assumptions made were that the AROC under the null hypothesis with phenotypes only was 0.60, and that the addition of SNPs would increase AROC estimates by between 0.1 and 0.2 units. For power calculation, a sample of data for 400 individual patients must achieve 82%–86% power to detect a difference of 0.1–0.2 between the AROC under the null hypothesis of 0.60 and an area under the curve (AUC) under the alternative hypothesis of 0.70 and 0.80 using a two-sided z-test at a significance level of 0.05.
The 365 patients in this study had a mean age of 54 ± 9 years, HbA1c of 7.9% ± 1.6% (63 mmol/mol), and FPG 9.0 ± 1.7 mmol/L, and 54% were male. The basic statistics on study parameters at randomization and the changes in study parameters at 1 year of treatment are presented in Table 1. The distributions of the biochemical study parameters, including the glycemic measures, were similar between the metformin and treatment naïve arms, although the proportion of men was marginally higher in the treatment naïve group (58%) compared with the metformin group (50%) (P = 0.064).
Data are expressed as median (interquartile range).
DI, disposition index; FPG, fasting plasma glucose; HOMA, homeostatic model analysis.
Changes in FPG and HbA1c values at the 1-year point were similar between the groups. The distribution of changes in glycemic measures for the two groups, along with their baseline levels, is presented in Figure 1. A significant (P < 0.01) 42% decrease in the DI was observed for both groups. The 1 kg average increase seen in body weight at 1 year was significant (P < 0.05) compared with the baseline body weight. Starting with a baseline FPG of 9.0 mmol/L, 44% patients achieved FPG <7 mmol/L at 1 year. The proportion of patients with HbA1c values <6.5% (48 mmol/mol) at the 1-year point in the metformin and treatment naïve groups was 19% and 24%, respectively (P = 0.26).
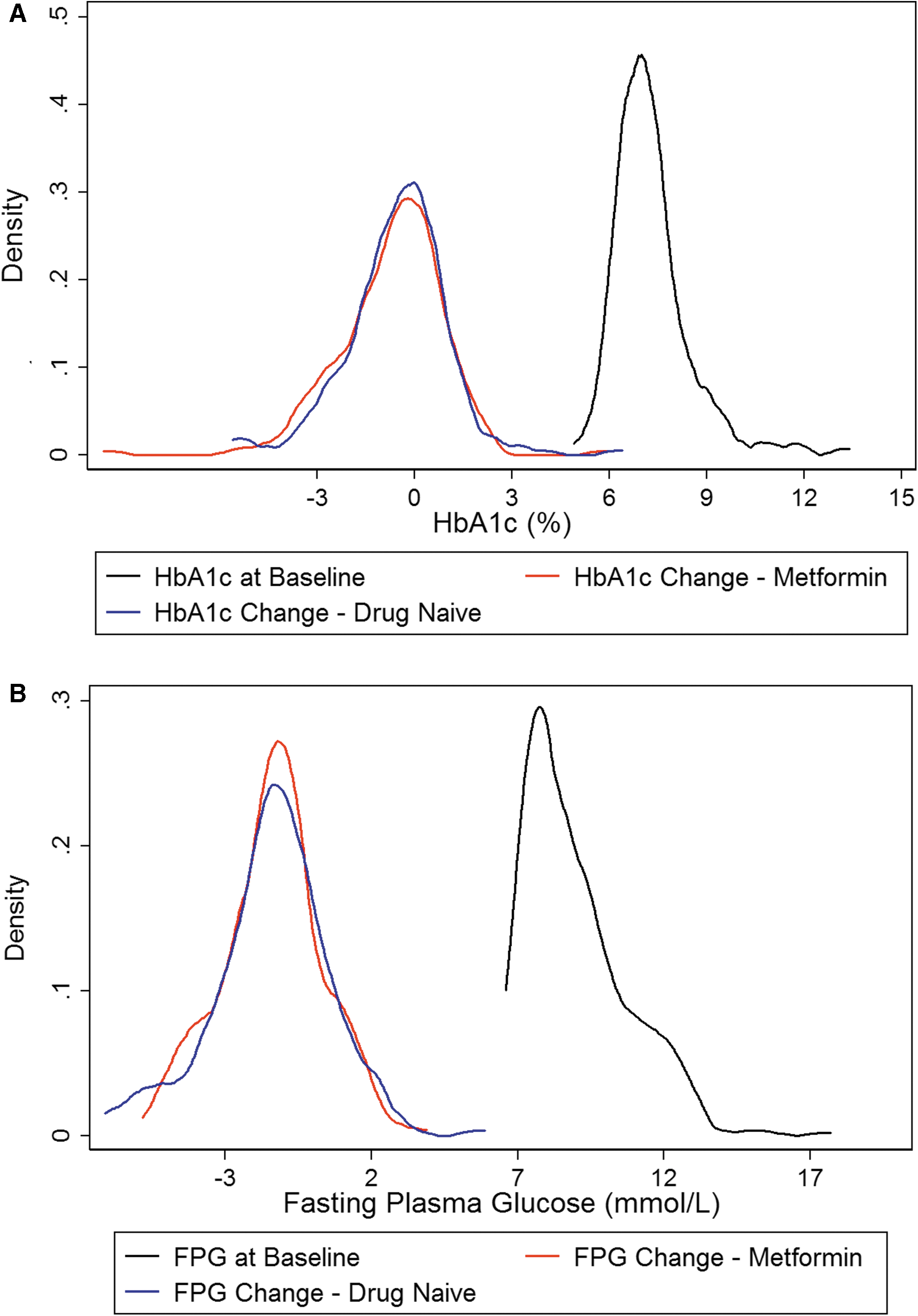
Kernel density plots of
A total of 2372 SNPs were selected for genotyping. Among these, 780 SNPs with a genotyping success rate >90% and minor allele frequency (MAF) >1% were included in the pharmacogenetic study. The statistically significant phenotypes and genes associated with the individual outcomes, along with the measures of their predictive abilities are presented in Table 2.
AROC of Clinical model versus AROC of Clinical+Genetic model.
Adjusted R 2.
AIC, Akaike Information Criteria; AROC, area under receiver operating curve; BIC, Bayesian Information Criteria; CHST13, chondroitin 4 sulfotransferase 13; MAPK1, mitogen-activated protein kinase 1; SNP, single nucleotide polymorphism.
Four genes identified with drug metabolism (FMO2, FMO3, UGT2B15, and CYP51A1, all P < 0.05 after adjustments for multiple testing) were found to be significantly associated with the likelihood of glycemic achievement as measured by HbA1c. The flavin containing monooxygenase (FMO2) was also significantly associated with FPG achievement. The transporter gene ABCC5 26 and mitogen-activated protein kinase 1 (MAPK1) were found to be significantly associated with both change in FPG and achievement of FPG <7 mmol/L. Another transporter gene, ABCB11, was significantly associated with change in the FPG level. Meanwhile, HbA1c and DI baseline values were significantly associated with HbA1c and FPG target achievements, respectively.
Compared with the clinical model, the addition of genetic markers (full model) significantly increased the predictive ability for both HbA1c- and FPG-based outcomes (Table 2). Indeed, the AROC of 0.77 with the full model for HbA1c was significantly higher than the AROC of 0.64 for the clinical model (P < 0.001). The full model also had a higher AIC compared with the clinical model (AIC: 357.36 vs. 380.37). For the outcome of FPG target achievement, the predictive ability of the full model was significantly higher (4%, P = 0.015) than the clinical model (AIC: 463.96 vs. 469.18). For the continuous outcome of change in FPG, the predictive ability of the full model was markedly better than the clinical model (Adjusted R 2: 0.32 vs. 0.25; AIC: 1375.0 vs. 1394.19).
Discussion
In this pharmacogenetic study involving 365 T2DM patients who began sulfonylurea treatment and were followed for a period of 48 weeks, we identified four genes (FMO2, FMO3, UGT2B15, and CYP51A1) related to drug metabolism and two transporter genes (ABCC5 and ABCB11) that could be associated with sulfonylurea efficacy or failure. Moreover, determination of whether T2DM patients carry these variants can significantly increase our ability to make more accurate drug response predictions than those that can be made using possible clinical predictors of drug response(s).
Drug response was closely associated with mechanisms that are involved in disease pathogenesis. In T2DM, the underlying biochemical defects include impairments of both insulin secretion and action, which could also be regarded as decreased beta-cell function and increased insulin resistance. The most important determinant of beta-cell function is the ATP-sensitive potassium channel that is targeted by sulfonylurea drugs. As such, genes associated with ATP-sensitive potassium channels (KCNJ11 and ABCC8) and insulin secretion pathways (TCF7L2) would be logical choices for pharmacogenetic studies of T2DM.
Although this study did not replicate the positive results for TCF7L2, 14 KCNJ11, 13 or ABCC8 11 genes in sulfonylurea efficacy, after evaluating 505 SNPs involved in diabetes or glucose metabolism or lipid metabolism, we did identify new variants in genes that encode receptor proteins and kinases. Interestingly, all of these newly identified genes (ESR1, BDKRB2, and MAPK1) are involved in insulin secretion and/or action.
ESR1 encodes estrogen receptor (ER), a ligand-activated transcription factor that is important for regulating gene expression. 27 Both estrogen and ERs are well-established regulators of glucose homeostasis. 20
BDKRB2 encodes a receptor for bradykinin (BK), a proinflammatory mediator and potent endothelium-dependent vasodilator. 28 Some studies found that the B2 receptor mediates the interaction of BK with pathways that are related to glucose homeostasis through receptor activation. 29 Consistent with this finding, a recent study showed that the BDKRB2 +9/−9 polymorphism reduced the transcriptional activity of the beta-2 adrenergic receptor (B2), which modifies glucose uptake and insulin secretion. 30
MAPK1 (mitogen-activated protein kinase 1) acts as an essential component of the MAP kinase signal transduction pathway that mediates metformin action, 31 and this action would be consistent with several studies documenting that specific modulation of protein kinase signaling can improve glucose homeostasis and protect against acquired insulin resistance and diabetes. 32
Drug response is not only associated with the mechanisms of disease pathogenesis mentioned earlier but also influenced by drug absorption, distribution, metabolism, and excretion. To further evaluate the efficacy of sulfonylurea, we investigated 1867 SNPs found in genes that encode drug transporters and drug-metabolizing enzymes.
To our knowledge there are no reports that focus on the relationship between drug transporters and sulfonylurea efficacy. Here we found that ABCC5, also known as multidrug resistance protein 5 (MRP5), was associated with FPG achievement and FPG changes. ABCC5 functions as an ATP-dependent export pump for cyclic nucleotides, 33 and a previous study reported significant reductions in liver MRP5 protein levels in diabetic rats fed high-fat diets relative to control diets. 34
Previous studies on drug-metabolizing enzymes generally focused on CYP2C9, which is known to influence the sulfonylurea efficacy in European populations. 20 Although the CYP2C9*2 and CYP2C9*3 genotypes can be related to sulfonylurea efficacy, these two genotypes are rare in Asian populations. 20,35 We included 12 CYP2C9 SNPs in this analysis, but the prediction value of CYP2C9 on sulfonylurea efficacy was, nonetheless, limited in this study. This phenomenon is similar to findings of another pharmacogenetic study that involved a Chinese population. 15
We also investigated genes encoding other CYP450 enzymes and found that the CYP51A1 gene significantly increased the predictive ability for HbA1c-based outcomes. CYP51A1 is the major cytochrome P450 enzyme that is involved in cholesterol synthesis and is already a major drug target, 36,37 although its role in sulfonylurea metabolism requires further study.
Several other genes considered in our study encode drug-metabolizing enzymes that significantly increased the predictive ability for both HbA1c- and FPG-based outcomes (FMO2 and UGT2B15). The MAF of these SNPs ranged from 15% to 34% (Supplementary Table S2). Previous studies implicated some of these genes in pathways related to glucose homeostasis, but the role of these genes in sulfonylurea efficacy remains unclear. The flavin-containing monooxygenases (FMO) are a family of drug-metabolizing enzymes that are involved in the oxidative metabolism of a variety of xenobiotics. 38,39 A recent study by Miao et al. (2015) implicated FMOs as insulin targets, and it proposed that FMO3 is necessary for development of the diabetic phenotype. 39 Genetic variants have been identified in FMO2 and FMO3, with many impacting substrate activity through loss of protein function. 40 Interestingly, expression quantitative trait locus (eQTL) analyses using the Genotype-Tissue Expression (GTEx) database identified significant associations between rs7512785 and rs7515157 SNPs and reduced FMO2 expression in pancreas samples (Supplementary Table S3).
Another enzyme, UGT2B15, is a member of the uridine diphosphate-glucuronosyltransferase (UGT) family, and it functions to eliminate substrates from the body through glucuronidation. 41 Notably, UGT polymorphisms are reported to modify clearance of the anti-diabetic agent sipoglitazar. 42
Finally, we identified two genes that have no known role in glucose metabolism. SPINK5 encodes a multidomain serine protease inhibitor that is involved in anti-inflammatory and/or antimicrobial protection of mucous epithelia. 43 Meanwhile, carbohydrate (chondroitin 4) sulfotransferase 13 (CHST13) is reported to localize to the Golgi apparatus membrane, where it catalyzes the transfer of sulfate to chondroitin. 44 Given that several other sulfotransferases participate in glucose metabolism, 45,46 CHST13 may have a similar role, although this possibility must be examined with further studies to confirm the association and identify the functional pathways.
In summary, a broad range of genes involved in pharmacokinetics and pharmacodynamics is a major strength of this study. In total, we included 2372 SNPs using an Infinium HD iSelect chip. Of these, we identified 1867 SNPs (78%) in genes encoding transporter and drug-metabolizing enzymes (pharmacokinetic), and 505 (22%) SNPs in genes involved in diabetes or glucose metabolism or lipid metabolism (pharmacodynamic).
Another strength of this study was the strictly defined phenotype. All participants were enrolled from a clinical trial that had a prospective design. Thus, factors such as diet, exercise, drug treatment compliance, and observer bias, which could obviously influence the judgment of sulfonylurea efficacy, were minimized in this double-blind, double-dummy controlled clinical trial relative to an observational study. These unique trial design features greatly facilitated our investigation of the influence of genetic background on sulfonylurea efficacy.
Our study also has some limitations. First, to exclude the effect of TCM in this pharmacogenetic study, we excluded patients treated with the Xiaoke Pill (glybenclamide+TCM) and analyzed only those patients in the Glybenclamide arm (365 participants). The study power was ∼80% when using the AROC as a guiding factor to evaluate the predictive ability of the SNPs along with the phenotypes. Therefore, an additional replication study with a larger cohort is needed to validate the results. Second, half of our study population was recently diagnosed with diabetes, and most were not obese. These patient characteristics indicate that caution should be taken when interpreting our findings, as they may not be directly generalized to patients with long-standing diabetes and/or obesity.
T2DM is a chronic disease with great genetic heterogeneity; our genetic results suggest that altered protein function in multiple pathways may cooperatively contribute to the increased discrimination by AROC, and perhaps explain, in part, the relationship between inter-individual variability and sulfonylurea response.
Footnotes
Acknowledgments
The authors thank the study participants and the 15 hospitals in China for their contributions to this study. QIMR Berghofer gratefully acknowledges an infrastructure research grant from the Australian Government Department of Education's National Collaborative Research Infrastructure Strategy initiative through Therapeutic Innovation Australia. This study was supported by grants from the National High Technology Research and Development Program (863 program, Nos. 2009AA022704 and 2012AA02A509), Beijing Science and Technology Committee Funding (D131100005313008), and Guangzhou Zhongyi Pharmaceutical. QIMR Berghofer gratefully acknowledges infrastructure research support from the Australian Government's National Collaborative Research Infrastructure Strategy (NCRIS) initiative through Therapeutic Innovation Australia.
Authors' Contributions
Q.R., L.J., S.K.P., X.H., and Z.L. conceived and designed the study. S.K.P. developed the analysis plan and conducted the statistical analyses. S.L.E. contributed to the genetic reference collections and interpretation of genetic variants. The initial draft of the article was prepared by S.K.P. and Q.R., and it was then circulated among all authors for a critical revision.
Author Disclosure Statement
All authors have completed the Unified Competing Interest form at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.