
Abstract
Background:
To find out whether children with type 1 diabetes accept a humanoid robot as an assistant in their diabetes management. In particular, the study aims to determine how the patients feel the robot may contribute to their care and how they respond to advice and education provided by the robot.
Subjects and Methods:
A humanoid robot was used in clinic and its acceptability was tested over 3 months in 37 children (aged 6–16 years) with type 1 diabetes during their clinic visits.
Results:
The obtained result showed that the overall patients' acceptability is 86.7%. However, the level of acceptability varies depending on the age group; patients aged 6–9 years showed the highest acceptability level of 94.8%, while the older age groups, 10–12 and 13–16 years, showed lower acceptability levels of 85.0% and 83.0%, respectively. There was no difference in the overall acceptability of the robot between the male and female patients (87.0% and 86.5%, respectively). Furthermore, features of the robot that were highly desirable include ability of the robot to give advice on high/low blood glucose (BG) levels (92.0%), how much the patients like the robot (91.4%), and ability of the robot to give advice on BG patterns (90.6%). In contrast, some other features were found least acceptable such as how likely patients want the robot as a companion (81.0%) and calculation of insulin doses with meals (82.53%). Analysis of variance across the responses of different age groups showed that P-value = 0.00003.
Conclusion:
Use of robots as a new device to support diabetes self-management in children was well accepted by patients.
Introduction
E
In this article, we report a user evaluation for a humanoid robot, which can support self-management of type 1 diabetes in children by supporting decision-making around insulin therapy and improving glycemic control by means of remote monitoring of physical and psychological health, and provision of education and motivation through an interactive humanoid robot.
Study Materials and Methods
The main device used in this study is a humanoid robot, 5 which integrates Bluetooth and Wi-Fi radio modules that are certified by the European Council of Radio Equipment and Telecommunications Terminal Equipment (R&TTE). The robot is used to collect information from patients (physical activity and carbohydrate and insulin intakes) as well as measurements using their blood glucose (BG) meters and optional blood pressure monitors and weight scales.
Information such as physical activity, well-being, and carbohydrate and insulin intakes is collected throughout an interactive verbal dialogue initiated by the patient. The robot collects this kind of information in various ways, for example: (1) Physical activity and well-being are collected by asking multiple-choice questions, such as “how do you describe your physical activity today, low, mild, or high?” and “how was your day, was it good, bad, or just ok?” In this case, the patient responds by selecting one of the specified keywords or one of its common synonyms. (2) Carbohydrate and insulin intakes are provided to the robot through touch sensors available at the robot's head that provided incremental values with prespecified increments.
The robot is also used to collect measurements from BG meters and other optional devices such as blood pressure monitors and weight scales through wireless Bluetooth connectivity. The measurements are automatically collected from prepaired devices without any user interventions. Once the data collection dialogue completes, the robot summarizes the collected information/measurements to the user and then obtains verbal consent before uploading them to a remote disease management hub (DMH) 6 for further processing and monitoring purposes.
Healthcare professionals can periodically review their patient's data through a user-friendly data-monitoring dashboard at the DMH. On successful login, she or he lands into a page that displays icons/photos for all patient populations in his or her capacity. Once a patient icon is selected, the system navigates to the corresponding dashboard. A sample screenshot for this dashboard is shown in Figure 1. This page displays the most recent data uploaded by the patient's robot, including BG readings, blood pressure, body weight, well-being, physical activity, and carbohydrate and insulin intakes, as illustrated. It should be mentioned here that the data presented in this illustration were only used for pilot test purposes. This page also comprises two menus of access links: main menu and diabetes management menu. The main menu provides access to the patient's vitals, medical profile, recent laboratory tests, and device management (i.e., robot registration and activation/deactivation). Similarly, the diabetes management menu provides access to other key platform applications such as treatment plan setup, dialogue-building wizard, patient advices, BG patterns, and insulin dose calculator. These applications are still open for further developments and refinements throughout further studies.
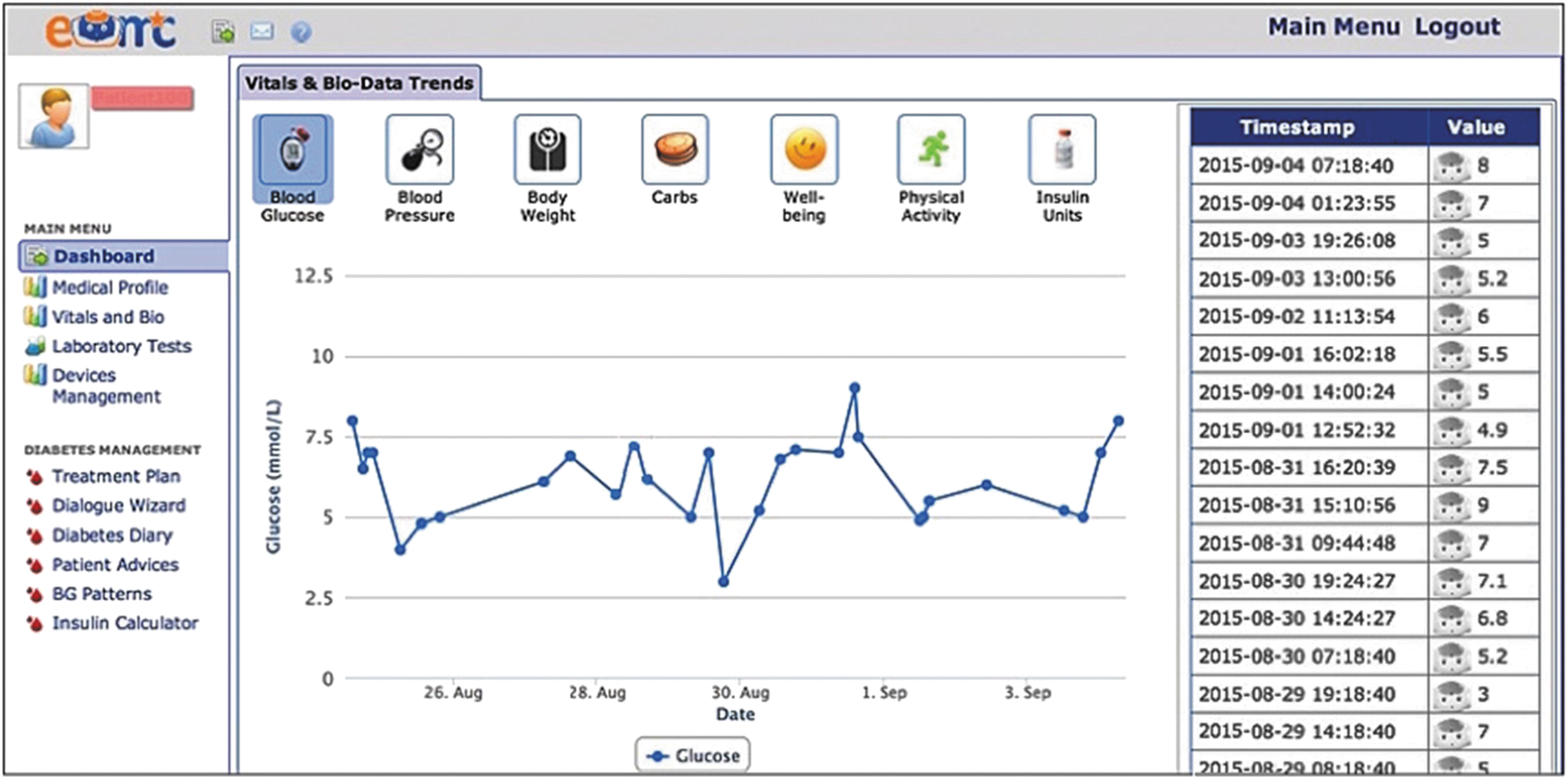
Example screenshot for the DMH dashboard. DMH, disease management hub.
Based on the patient's health profile, the physician can adjust the insulin treatment plan (if necessary) and assign or create appropriate education and motivation dialogues tailored to the individual needs of each patient. A flexible and easy use dialogue-building wizard 7 was developed in the DMH to support creation and delivery of various kinds of dialogues to the patient's robot at home. These changes are automatically downloaded to the robot, which in turn performs the necessary verbal interactions with the patient as specified by the physician. Example of the patient–robot interaction setup is shown in Figure 2.

Patient–robot interaction setup.
A total of 37 children, between 6 and 16 years old, participated in this study. Patients were approached to interact with the robot in the clinic waiting areas and functions were demonstrated by the technical team. Each child interacted with the robot and accessed different data collection and educational modules on one occasion for at least 30 min in the clinic environment in the presence of a clinician and the participant's parent/guardian. Patients then completed a questionnaire assessing the attitudes and acceptance of the system. Data were collected from the children and were analyzed according to demographic characteristics (i.e., age and gender) and age groups. For patients younger than 12 years, the questionnaires were filled with the aid of their parents/guardians, while older children aged 12–16 completed the questionnaires themselves.
Results
Thirty-seven children were included in the study, 10 children younger than 10 years, 10 children between ages 10 and 12 years, and 17 children between ages 13 and 16 years. Mean HBA1c was 9.0% and seven children were using insulin pumps. Mean duration of diabetes was 3.1 years, and 18 were Afro-Caribbean in origin. Boys and girls were evenly split across the age groups.
Overall patients' acceptability of the robot was 86.76%. The acceptability of the robot varied between the age groups with patients aged 6–9 years showing the highest overall acceptability level of 94.8%, with lower overall acceptability in the older age groups: 85.0% (10–12 years) and 83.0% (13–16 years). There was no difference in the overall acceptability of the robot between the male and female patients (87.0% and 86.5%, respectively). Data on acceptability of individual attributes and services offered by the robot are summarized in Table 1. Features of the robot that were highly desirable among all age groups include ability of the robot to provide advice on how to deal with high and low BG levels and ability to relay BG readings to their medical staff. Interestingly, the ability to deliver education around diabetes was significantly less acceptable by the older patients (83.6%) compared with the younger patients, where 100% acceptability was recorded.
BG, blood glucose.
The ability to be a companion and the ability to calculate insulin doses achieved lower acceptance of 74.5% and 77.5%, respectively, in children aged older than 10 years, but both of these features achieved higher acceptance scores of 94% and 88%, respectively, in those aged younger than 10 years. Furthermore, 98.0% of the patients <10 years of age expressed an interest in taking the robot home with them to help with their diabetes, while 83.4% of patients >10 years showed interest in this feature.
Discussion
This brief exploratory study showed that a humanoid robot was well accepted by patients and parents of children with type 1 diabetes and added a personal dimension to the interaction with technology. Many of the children expressed a desire to take the robot home and thought it would be helpful in managing their diabetes. Interestingly, patients >12 years of age were significantly less keen (77.6%) to use the robot to help them make decisions about insulin than patients <10 years of age (88.0%). This may indicate that although patients were quickly convinced of the supportive benefits of the robot, children in different age groups may use the robot in different ways, with older children wanting to assert their independence and declining the offer of help. Some features, such as the bolus advice feature, may not be valuable to children using insulin pumps that have this facility built in.
The HbA1c levels of our patients highlight the challenges faced in achieving tight control and, in particular, engaging and encouraging interaction between children and their diabetes, especially in ethnic inner city populations that have known associations with higher HbA1c. Unlike other chronic diseases, self-management of diabetes requires continued self-monitoring with titration of treatment to diet and exercise. Real-time decisions are necessary through interpretation of data measured in the home. Robots as children companions have a promising role in supporting various care aspects of diabetes, including continuous BG monitoring, education, health advice and alert messages tailored to individual needs. In addition, psychological and behavioral monitoring is another dimension of diabetes care that can be supported by continuous robot interactivity with the patient at home. Patients could become more emotionally and psychologically involved in their diabetes through interacting with a robot. These health services could be managed and delivered to patients at home under remote supervision of healthcare professionals.
As remote technology has been increasingly used to obtain data and support patients at home, solutions that facilitate the transfer of data from the home to the healthcare professional are valuable. Cloud computing allows for real-time data management and can be used to identify glucose trends to the patient or provide notifications to healthcare teams about patients. For many patients, systems such as this can offer support to the patient at home.
Decision-support algorithms can be delivered through the remote DMH. The authors have developed a bolus advisor 8 using a feed-forward multi-perceptron artificial neural network to incorporate parameters, including carbohydrate, insulin, and activity, to provide bolus advice. Collection of data will allow a sequential data-mining algorithm 9 to identify common patterns and we aim to be able to use the robot to help link these patterns with an educational interaction between the robot and the child. The physician activates these algorithms depending on the individual needs of each child. For the physician, the system also supports decision-making through remote monitoring of physical and psychological health of the patients, allowing timely interventions and care prioritization.
The e-health platform also supports integrating long-term behavioral change management within the routine care of the disease in a single platform rather than dealing with these psychological aspects separately. In addition, the developed prototype is still open for further improvements; for example, increasing the speed and response of dialogue and keeping the conversation flexible to maintain interest for the child. The results of this early pilot study support further developments and larger studies, which are part of on-going work by the authors.
Footnotes
Acknowledgments
This research was partially executed at Kingston University London and supported by the seventh European Community Framework Programme—Marie Curie Actions, under Grant No. 275571.
Author Disclosure Statement
No competing financial interests exist.