
Abstract
Objective:
This study determined the feasibility and efficacy of an automated proportional-integral-derivative with insulin feedback (PID-IFB) controller in overnight closed-loop (OCL) control of children and adolescents with type 1 diabetes over multiple days in a diabetes camp setting.
Research Design and Methods:
The Medtronic (Northridge, CA) Android™ (Google, Mountain View, CA)-based PID-IFB system consists of the Medtronic Minimed Revel™ 2.0 pump and Enlite™ sensor, a control algorithm residing on an Android phone, a translator, and remote monitoring capabilities. An inpatient study was completed for 16 participants to determine feasibility. For the camp study, subjects with type 1 diabetes were randomized to either OCL or sensor-augmented pump therapy (control conditions) per night for up to 6 nights at diabetes camp.
Results:
During the camp study, 21 subjects completed 50 OCL nights and 52 control nights. Based on intention to treat, the median time spent in range, from 70 to 150 mg/dL, was greater during OCL at 66.4% (n = 55) versus 50.6% (n = 52) during the control period (P = 0.004). A per-protocol analysis allowed for assessment of algorithm performance with the median percentage time in range, 70–150 mg/dL, being 75.5% (n = 37) for OCL versus 47.6% (n = 32) for the control period (P < 0.001). There was less time spent in the hypoglycemic ranges <60 mg/dL and <70 mg/dL during OCL compared with the control period (P = 0.003 and P < 0.001, respectively).
Conclusions:
The PID-IFB controller is effective in improving time spent in range as well as reducing nocturnal hypoglycemia during the overnight period in children and adolescents with type 1 diabetes in a diabetes camp setting.
Introduction
T
The emphasis with system development has been to develop and test fully automated, portable systems with safety parameters and remote monitoring capabilities to proceed with home studies. 9,13 The move to outpatient, ambulatory studies requires a robust system demonstrating not only efficacy but also safety parameters such as maximum insulin delivery, fault detection algorithms for sensor error and failure of individual system components, and flawless communication between devices. The opportunity to improve glucose control during the overnight period would have a substantial impact on the enormous burden of care of children with type 1 diabetes. Prolonged, nocturnal hypoglycemia remains a significant concern with up to 75% of all hypoglycemic seizures occurring during sleep. 14
The Medtronic (Northridge, CA) Android™ (Google, Mountain View, CA)-based system using a proportional-integral-derivative with insulin feedback (PID-IFB) algorithm is an investigational device designed for physician-supervised OCL control in patients with type 1 diabetes. The automated system consists of an insulin pump and glucose sensor, a controller algorithm residing on an Android phone platform, and a translator to allow communication between the pump and phone, as well as remote monitoring capabilities. The current PID-IFB algorithm utilizes conventional proportional-integral-derivative concepts emulating β-cell function 15,16 with the added sophistication of safety modules, an important consideration as clinical studies move into the home environment.
The diabetes camp environment is a challenging opportunity for optimizing glucose control. Children and adolescents with type 1 diabetes are encouraged to participate in physical activities that increase the risk for severe, nocturnal hypoglycemia. 17 The camp setting allows multiple subjects to be studied simultaneously and allows testing of closed-loop system performance in a rugged, real-world setting.
The objective of this study was to evaluate the feasibility and efficacy of the PID-IFB controller in overnight glucose control in children and adolescents with type 1 diabetes over multiple days in a diabetes camp setting. The primary outcome was defined as time spent in range, from 70 to 150 mg/dL, during the overnight period.
Research Design and Methods
Closed-loop system
The closed-loop system consists of the Medtronic Minimed Paradigm Revel™ 2.0 pump used together with the Medtronic Minimed Enlite™ sensor and MiniLink™ transmitter. Sensor glucose values were updated on the pump every 5 min, and this signal was transmitted to the controller via the translator. The translator converts the Medtronic proprietary radiofrequency signal to Bluetooth® (Bluetooth SIG, Kirkland, WA) format to allow communication between the pump and the phone. During closed-loop mode, the controller uses the PID-IFB algorithm to calculate and command insulin delivery every 5 min via the translator.
The controller is also connected to a remote server via wireless wide area network to provide data on sensor glucose and insulin delivery and to accept external controls, when necessary. The system is illustrated in Figure 1.
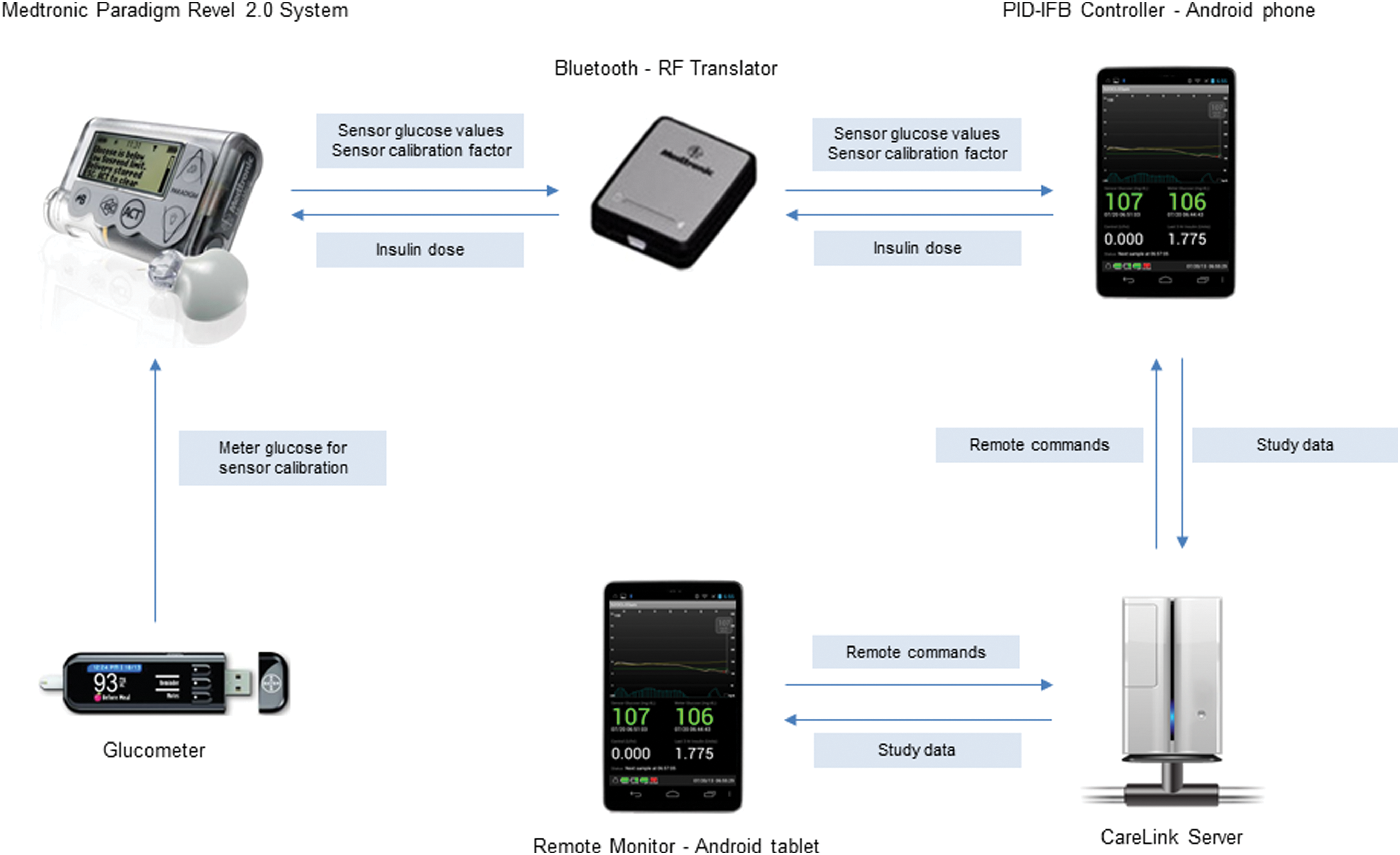
Medtronic Android-based proportional-integral-derivative controller with insulin feedback (PID-IFB) system. RF, radiofrequency.
PID-IFB algorithm
Initial attempts to model the pancreatic β-cell were led by the observation that the β-cell response to an acute elevation in plasma glucose level could be well described by a proportional-integral-derivative control algorithm. 18,19 Insulin feedback was later added to emulate the effect of insulin inhibiting insulin secretion. This was subsequently evaluated in a clinical study of adults with type 1 diabetes 16 and resulted in the current closed-loop controller, the PID-IFB algorithm.
Several safeguards have been incorporated into the nocturnal control algorithm, including assessing the accuracy of sensor performance prior to initiation of closed-loop control, an individualized constraint on the maximal insulin delivery rate, and a gradual lowering of the glucose set-point when the glucose level is above a preset threshold on initiation of closed-loop control.
Closed-loop initiation algorithm
The closed-loop initiation algorithm determines if the system can enter closed-loop mode by first assessing the magnitude and stability of the most recent calibration factor compared with previous calibration factors. If there is hyperglycemia at commencement of closed-loop control, a target glucose level safeguard allows for a smoother transition between open-loop and closed-loop mode by gradually lowering the target glucose over approximately 2 h until the adjusted target glucose converges to the set-point of 120 mg/dL. A correction bolus is calculated if the glucose level is >180 mg/dL at the start of closed-loop control. The correction bolus is calculated based on the patient's average total daily dose of insulin and insulin on board and is targeted for a glucose level of 120 mg/dL. A correction bolus is only calculated and delivered at the start of closed-loop control.
Insulin delivery safeguards
The insulin limit constrains the maximum amount of insulin delivered to the patient at any time in order to avoid overdelivery of insulin by the algorithm due to potential sensor error. The insulin limit is a value that is specific to each patient and is calculated from his or her previous overnight basal rates and overnight glucose control over approximately 3–5 days of standard pump therapy.
Study procedures
Participants were eligible to participate if they were between 10 and 35 years of age, diagnosed with type 1 diabetes for at least 12 months, using an insulin pump for at least 3 months, and attending diabetes camp. The protocol was approved by the Stanford University Institutional Review Board.
Exclusion criteria included diabetes ketoacidosis in the preceding 30 days, hypoglycemic seizure or loss of consciousness in the preceding 3 months, pregnancy, or medical or psychiatric conditions considered to interfere with completion of the protocol. There were no glycated hemoglobin (A1C) exclusion criteria.
An initial inpatient study was completed to evaluate the feasibility and safety of the system in 16 participants with type 1 diabetes. Participants were admitted for one 22-h period in the hospital for OCL control. The inpatient phase was designed to mimic the first day of camp. An Enlite glucose sensor was inserted. A Paradigm Revel 2.0 pump was programmed with each subject's current pump settings and used for insulin delivery. All calibrations were performed using fingerstick meter blood glucose measured by the Bayer Contour® Next USB glucometer (Bayer HealthCare, Leverkusen, Germany). The first calibration was entered approximately 2 h after sensor insertion, prior to lunch. Additional calibrations were entered prior to dinner and the bedtime snack.
Participants engaged in two periods of exercise: in the afternoon and after dinner. An intravenous cannula was inserted at 2000 h to allow for overnight venous blood sampling every 30 min for the duration of closed-loop control. Plasma glucose values were measured using the YSI 2300 Stat Plus™ glucose analyzer (Yellow Springs Instrument, Life Sciences, Yellow Springs, OH). The methodology for these studies is discussed further in Supplementary Data (Supplementary Data are available online at
For the main camp sessions, eligible subjects were screened in the week prior to attending camp. Participants were sent a Contour Next USB glucometer and advised to obtain two fasting glucose values, 20 min apart, on at least 3 days in the week preceding camp. This information was used to calculate the maximum basal insulin infusion rate overnight during closed-loop control.
On the subject's arrival at camp, an Enlite sensor was inserted and connected to a Minilink transmitter. Subjects were switched to a Paradigm Revel 2.0 pump programmed with their current pump settings, and the sensor was started. All calibrations were performed using the fingerstick meter blood glucose level measured by the Contour Next USB glucometer. Following the initial calibration at 2 h following insertion, patients were instructed to calibrate prior to breakfast, dinner, and the bedtime snack.
Participants were randomized to either OCL or sensor-augmented pump therapy for the first night and then crossed over on alternate nights to the other treatment arm over the course of the 5–6-day camp session. All subjects participated in the camp activity program during the day and evening, and therefore exercise intensity was similar regardless of the overnight intervention assignment.
Control conditions
During the control nights, subjects continued on sensor-augmented pump therapy only. Low and high glucose alerts were set at 70 mg/dL and 250 mg/dL, respectively. Subjects were not remotely monitored and were under the care of camp medical staff. Overnight glucose monitoring included routine meter glucose testing at 0000 and 0300 h if clinically indicated.
Data from each closed-loop night were shared with the clinical team in order to facilitate changes to insulin therapy as required for subsequent nights. Changes to overnight basal rates on control nights were incorporated into the closed-loop algorithm the following night.
Closed-loop initiation
OCL was commenced in the evening as participants prepared for sleep, generally between 2200 and 2300 h. Specific patient parameters were calculated based on patient weight, total daily dose, insulin delivery rates, and fasting glucose levels in the preceding week.
Closed-loop control was commenced if sensor glucose values were between 70 and 350 mg/dL and sensor error was ≤20%.
Meter glucose values were obtained at 0000, 0300, and 0600 h. If the sensor glucose value differed from the meter glucose value by more than 20%, the meter glucose was entered as a calibration value, and a repeat meter glucose reading was obtained after 1 h. If the second reading differed from the sensor glucose by >20%, closed-loop control was stopped.
Hypoglycemia
Closed-loop control proceeded uninterrupted when sensor glucose values were between 70 and 250 mg/dL. When sensor glucose values decreased below 70 mg/dL via remote monitoring, a meter glucose value was obtained. If meter glucose values were <50 mg/dL, oral glucose treatment would be given, and closed-loop control would be suspended for the patient that night. If the meter glucose value was between 50 and 70 mg/dL, hypoglycemia treatment was given in the form of 15 g of fast-acting carbohydrate (juice or glucose tablets). If the meter glucose obtained 15 min later was >70 mg/dL, then 15 g of complex carbohydrate was given, and closed-loop control was continued.
Hyperglycemia
If sensor glucose values were >250 mg/dL, a meter glucose value was obtained, and if the finding was verified, blood ketone levels were obtained. If blood ketone levels were ≤0.6 mmol/L, closed-loop control was continued. If ketone levels were >0.6 mmol/L, closed-loop control was stopped, patients received a subcutaneous insulin correction dose, a new insulin infusion set was inserted, and closed-loop control was suspended for a minimum of 2 h.
Closed-loop control would be suspended for the individual patient if meter or plasma glucose values were <50 mg/dL or >400 mg/dL. Ketone levels were measured daily at 0700 h.
Sample size
The sample size for the main camp study was calculated based on the percentage of time in range, between 70 and 150 mg/dL. For a similar cohort 20 of children and adolescents with type 1 diabetes on sensor-augmented pump therapy, subjects spent 51 ± 30% of the time in range. We assumed a 20% absolute improvement in the time in range with closed-loop control would be clinically significant. At a significance level of 0.05 and 90% power, we would require 48 nights of closed-loop therapy and 48 control nights to detect a 20% improvement using a paired t test. Twenty subjects were recruited with the anticipation that each subject would be studied in up to 6 nights and to allow for sensor error that would prevent initiation of closed-loop control.
Data analysis
For the intention-to-treat analysis, all sensor values from 2300 to 0700 h from both the OCL and control groups were compared, regardless of system status.
For the per-protocol analysis, data from OCL nights during which there were technical problems such as infusion set failure, sensor error >20%, or pump failure resulting in a >60-min interruption to closed-loop control were removed to allow for analysis of algorithm performance. Only nights with a minimum of 5 h of OCL were included, and all glucose data were included in the analysis. For comparison, only nights during which sensor error was <20% with a minimum of 5 h of data were included in the control group.
Depending on distribution, data are expressed as mean ± SD values, mean ± 95% confidence interval, or median and interquartile range (25th–75th percentile). The data were analyzed as a crossover design where each patient was randomized to one of the two treatment groups and crossed over to the other group after each night for a total of 6 nights. The number of events during the OCL nights and the number of events during the control nights were analyzed in a Poisson regression analysis.
Given that there was remote monitoring in place during closed-loop control, we assessed nights during which the threshold for intervention was potentially reached in both groups, being <70 mg/dL or >250 mg/dL. An event was described as having at least 10 min of sensor glucose within the described range.
Results
Inpatient studies
During the inpatient phase, 16 subjects (nine males) were admitted for 1 night of overnight glucose control. The mean age was 15.2 ± 2.5 years, duration of diabetes was 7.7 ± 4.6 years, and A1C was 9.0 ± 1.0%.
Closed-loop control was commenced in 13 (81%) of 16 participants and did not start in three participants because of sensor error. For patients who entered closed-loop control, the median interval of closed-loop control per night was 9.2 (8.0, 9.6) h.
The median percentage of time spent between 70 and 150 mg/dL was 63% (41, 89), and that for time spent <70 mg/dL was 0% (0, 0). Plasma glucose values decreased <70 mg/dL on three occasions, all within 2 h of starting closed-loop control, and carbohydrate treatment was given in all cases. The overall Day 1 mean absolute accuracy of the Enlite sensor was 14.1 ± 11.6% with a median of 11.3% (4.7, 20.0) (n = 247). For the 10 patients in whom closed-loop control was initiated, the mean absolute relative difference (ARD) was 11.4 ± 9.1% with a median ARD of 9.6% (4.3, 16.3) (n = 192).
Camp sessions
During the camp sessions, 21 subjects (10 males) were enrolled and studied over 107 nights. The mean age was 14.7 ± 3.9 years (range, 10.1–24.8 years), weight was 55.6 ± 16.4 kg, total daily dose of insulin was 0.8 ± 0.2 unit/kg/day, duration of diabetes was 7.9 ± 5.3 years, and A1C level was 7.9 ± 1.4% (range, 6.4–12.5%).
Intention-to-treat analysis
OCL was commenced in 50 of 55 potential nights (91%). Closed-loop control did not start in 5 nights because of the sensor failing to pass the sensor performance requirements on initialization. There were 52 nights of sensor-augmented pump use for comparison.
On an intention-to-treat basis, the percentage time in range, from 70 to 150 mg/dL, was greater during OCL at 66.4% (n = 55) versus 50.6% (n = 52) during the sensor-augmented pump period (P = 0.004), as shown in Table 1. For the range 70–180 mg/dL, the percentage of time was 79.9% in OCL versus 60.0% for sensor-augmented pump use (P < 0.001). The OCL period was also associated with less percentage of time spent <50 mg/dL, 60 mg/dL, 70 mg/dL, and 250 mg/dL compared with sensor-augmented pump therapy.
Data are least means square ± standard error values.
ITT, intention-to-treat; PP, per-protocol.
The average overnight glucose values were no different for both conditions with 132 (119, 144) mg/dL for OCL and 128 (115, 141) mg/dL for sensor-augmented pump conditions (P = 0.6494). There was also no difference in the glucose variability as measured by SD of glucose values, with a median of 27 mg/dL for OCL and 28 mg/dL for control nights (P = 0.665). The mean fasting meter glucose was 139 (120, 157) mg/dL following OCL nights and 148 (128, 165) mg/dL following control nights (P = 0.389). We examined for the effect of order for the first night, and no effect was seen.
During OCL, there were no glucose events <50 mg/dL or >400 mg/dL. There was one session suspended because of an event with a glucose level of >250 mg/dL with ketone levels of ≥0.6 mmol/L attributed to infusion set failure.
There were eight episodes of hypoglycemia detected as sensor glucose values fell below 70 mg/dL and verified by meter glucose values during OCL. Four of these episodes occurred within 3 h of starting OCL and were attributed to prebedtime snack boluses given prior to initiation of OCL. An example is included in Supplementary Data. There was minimal delivery of insulin by the system prior to these hypoglycemic events. The remaining four episodes occurred later during the course of the night. In all cases, oral glucose treatment was given, and OCL was continued; there were no glucose readings <50 mg/dL.
During sensor-augmented pump therapy, there were 12 episodes with a confirmed meter glucose level of <70 mg/dL, requiring treatment with oral glucose. There were a further five episodes with a meter glucose level of >70 mg/dL during which the patient was symptomatic and requested hypoglycemia treatment. The incident rate during the OCL night is 0.38 times lower than the incident rate during the control nights (P = 0.0299).
In terms of sensor performance over the camp sessions, mean ARD for the Enlite sensor was 19.2%, and median ARD was 14.2% (n = 798). There were fewer calibrations during control nights with an average of 0.2 versus 2.6 calibrations during closed-loop nights (P < 0.001).
Ketone levels at the end of closed-loop nights were similar to those following sensor-augmented pump nights, with a mean of 0.2 (0.1, 0.3) mmol/L versus 0.3 (0.2, 0.3) mmol/L, respectively (P = 0.07).
There was no difference in the total overnight insulin doses (2300–0700 h) with an average of 7.2 ± 3.8 units during OCL and 7.1 ± 3.4 during control conditions (P = 0.796).
Duration of closed-loop control and technical interventions
The median duration for closed-loop control during nights when it was operational was 7.7 (5.8, 8.4) h. Closed-loop control proceeded through the night without technical intervention in 23 nights (42%). Closed-loop control was interrupted in 27 nights. In 14 of these 27 nights, we were able to resume closed-loop control after resolving the following: loss of communication between devices (seven events), minimum 2-h insulin limit reached (five events), pump error (one event), and reviewing algorithm parameters (one event). The median duration of interruptions during active closed-loop control was 19 (10, 34) min. Closed-loop control was started and stopped prematurely during 13 nights (26%) for the following reasons: sensor error being >20% (9 nights, 18%), loss of connectivity giving rise to a greater than 60-min interruption of OCL (2 nights, 4%), infusion set failure (1 night, 2%), and a sensor failing to meet algorithm calibration standards during a system restart (1 night, 2%).
Per-protocol analysis
The per-protocol analysis included 37 OCL nights compared with 32 sensor-augmented pump nights, and glucose outcomes are shown in Table 1. The percentage time in range, from 70 to 150 mg/dL, was greater during OCL at 75.5% versus 47.6% during the sensor-augmented pump period (P < 0.001), as shown in Table 1. For the range 70–180 mg/dL, the percentage of time was 88.1% in OCL versus 60.5% for sensor-augmented pump use (P < 0.001). The OCL period was also associated with a lower percentage of time spent <60 mg/dL and 70 mg/dL, as well as less time spent >150 mg/dL and 180 mg/dL, compared with sensor-augmented pump use.
Figure 2 demonstrates the mean ± SD glucose values per protocol over the duration of the night for both conditions with data from the per-protocol analysis.
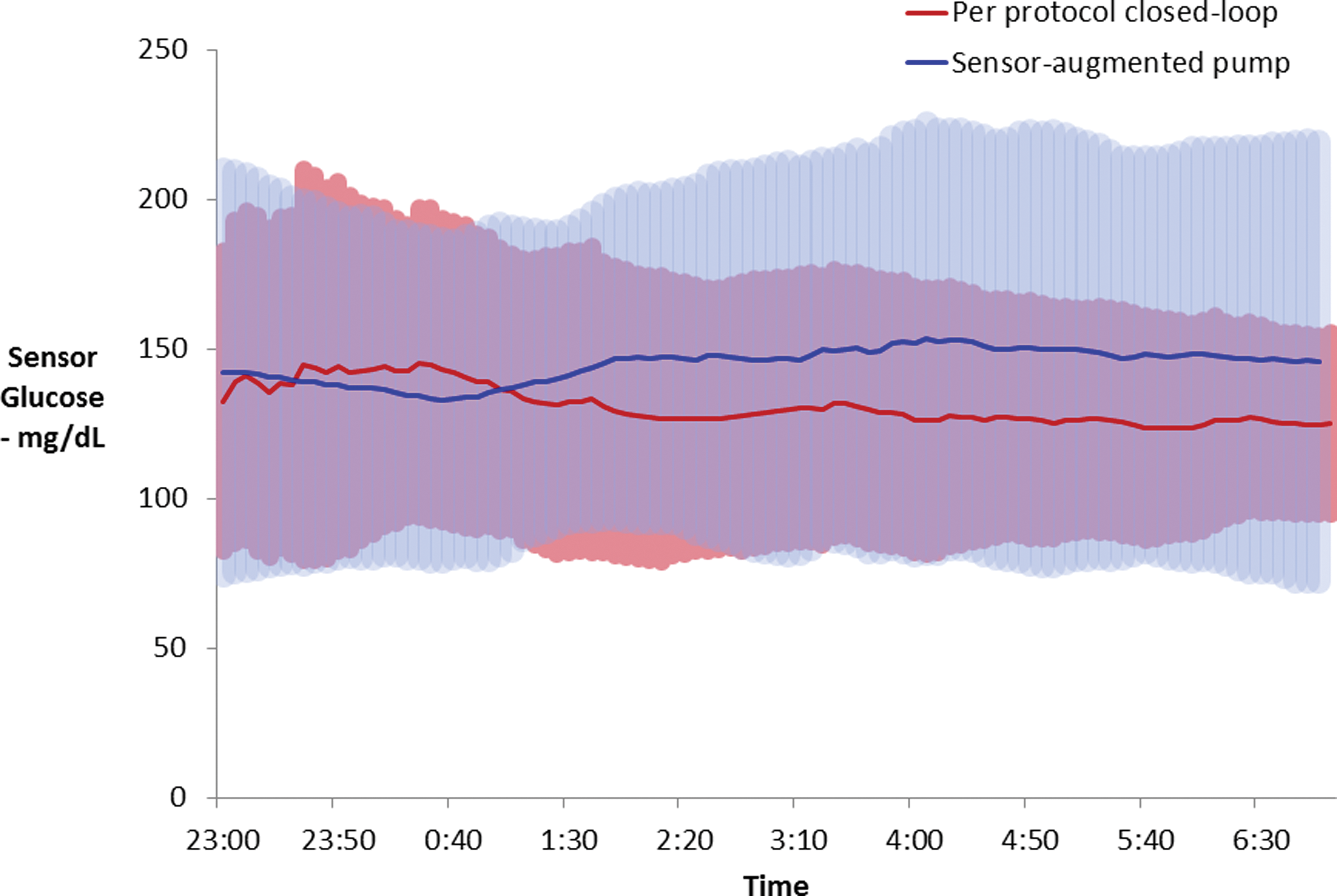
Per-protocol analysis of sensor glucose values during the overnight period (8 h) of closed-loop control (n = 37) versus sensor-augmented pump nights (n = 32). Data are mean ± SD values.
Mean glucose values were also calculated per night under both conditions for individual patients. These values were similar for both conditions, with a mean of 132 ± 24 mg/dL for OCL nights versus 140 ± 42 mg/dL for control nights (P = 0.483) (n = 17 subjects). There was, however, less glucose variability during OCL conditions, with a mean ± SD level of 28 ± 12 mg/dL versus 42 ± 18 mg/dL for control conditions (P = 0.014).
The number of nights with one or more events <70 mg/dL was 6 for OCL versus 14 for control conditions (P = 0.027). The number of nights with one or more events >250 mg/dL was 2 for OCL versus 11 for control conditions (P = 0.039).
Discussion
OCL control with the Android-based PID-IFB controller was successful in reducing nocturnal hypoglycemia and increasing the time spent in range compared with sensor-augmented pump therapy. This was achieved in a cohort of children and adolescents with variable glucose control, as measured by A1C, over multiple nights in a diabetes camp setting. This occurred outside of a controlled, hospital setting with a portable, automated system. In addition to reducing hypoglycemia, we demonstrated less glucose variability during the overnight period.
The main limiting factor during this series was sensor performance. Closed-loop control either did not start or was stopped prematurely because of poor sensor performance in 27% of nights. At the initiation of closed-loop control, sensor performance was evaluated by the initiation algorithm to ensure that only reasonably accurate sensors were used for closed-loop control. Sensor performance in the camp environment was less accurate (median ARD of 14.2%) compared with our inpatient experience (median ARD of 9.6%) despite all inpatient sensors being less than 12 h old when closed-loop control was initiated. In this protocol, sensor accuracy was also evaluated with frequent overnight glucose testing at 0000, 0300, and 0600 h as a safety feature, and if a sensor was not able to be calibrated within 20% of the meter reading, then closed-loop control was stopped. More sophisticated algorithms designed to detect sensor error or failure will be an important future safety feature of closed-loop systems.
We were not able to eliminate hypoglycemia with this closed-loop system. Half of the overnight hypoglycemia events occurred within the first 3 h of starting the system and were secondary to active insulin on board given prior to the start of closed-loop control. As we move to the home environment, patient behavior and decisions regarding insulin doses during open-loop control will impact the transition from open-loop to closed-loop control. Patients may rely on the controller to compensate for their decisions, with either under- or overdelivery of insulin during open-loop control, and this will impact glucose control in the few hours after initiation of closed-loop control. Changes in patient behavior observed with the use of closed-loop systems will need to be evaluated and considered as the user interface evolves.
The mean glucose values were not different during OCL and control nights. This was not unexpected because subjects used the closed-loop system on alternate nights. Any changes made to basal infusion rates on nights using sensor-augmented pump were incorporated into the PID-IFB algorithm, and likewise patterns of insulin delivery observed during closed-loop control were incorporated into control nights. This was built into the study design to ensure safety of the campers. We have used a similar study design and found similar results using overnight glucose control with the Diabetes Assistant (DiAs) developed by the University of Virginia artificial pancreas group. 13
OCL control has also been tested in a diabetes camp setting using the MD-Logic system. 9 Both the MD-Logic and the current PID-IFB systems were studied in a similar number of nights in a diabetes camp setting. There were, however, several differences in study design. The PID-IFB system was tested in multiple nights on each subject with up to 3 nights per subject compared with 1 night per subject in the MD-Logic study. The MD-Logic system was initialized before dinner, between 1600 to 1700 h, whereas our subjects were connected at bedtime, between 2200 to 2300 h. As an important step forward, this group has recently completed a 6-week study of OCL in home with remote monitoring. During the 6 weeks of closed-loop control, the time in target (70–140 mg/dL) increased from 36% to 47% when compared with the 6 weeks of control nights. 8
Hovorka and co-workers 1,2,21,22 have completed several landmark studies examining closed-loop control in adolescents and children. In a study 21 involving both day and night closed-loop control over a 32-h period in hospital in 12 adolescents, plasma glucose levels were in the range of 71–145 mg/dL for 76% on the first night and 95% on the second night. We achieved similar results in our studies in the camp setting with a median of 86% for time spent between 70 and 150 mg/dL. In their study of in-home OCL control for 3 weeks in 16 adolescents without the use of remote monitoring, 23 they demonstrated increased time in target (70–144 mg/dL) from 47% on control nights to 64% on intervention nights. Most recently, the group reported results from their 3-month crossover trial, and for their adolescent cohort, time in range was improved from 34% to 60% with closed-loop control. 24
The closed-loop platform used in this study was designed to be investigational only, and connectivity was certainly not sufficiently robust for longer outpatient studies. Device issues that reduced time in closed-loop control included loss of sensor signal as well as loss of connectivity between devices. These issues have been largely improved in later systems, such as the Medtronic 670G hybrid closed-loop system, designed for ambulatory closed-loop control, where the algorithm is housed inside the pump, and sensor signal has been noticeably improved compared with the Enlite sensor.
In conclusion, the PID-IFB controller was effective in increasing the time spent in range during the overnight period and reduced nocturnal hypoglycemia compared with sensor-augmented pump therapy in children and adolescents with type 1 diabetes at a diabetes camp setting. The results from this study provide promising data in moving toward outpatient studies in the home environment to further evaluate safety and efficacy as well as refinements to the safety parameters and fault detection algorithms that are intrinsic to an automated closed-loop system.
Footnotes
Acknowledgments
This work is supported by a grant from Medtronic Diabetes. T.T.L. is supported by the University of Western Australia F.A. Hadley Overseas Medical Fellowship. We thank the participants and their families for taking part in this study. We also thank the medical staff, directed by Dr. Kevin Kaiserman at Camp Conrad-Chinnock, and camp staff, directed by Dr. Rocky Wilson at Camp Conrad-Chinnock, for making this study possible.
Author Disclosure Statement
D.B.K., A.R., J.H., B.G., M.C., and N.K. are employees of Medtronic Minimed and are Medtronic shareholders. B.A.B. is on medical advisory boards for Sanofi, Novo-Nordisk, BD, UnoMedical, and Medtronic and has received research grant and/or material support from Medtronic, Dexcom, LifeScan, Insulet, Bayer, UnoMedical, and Tandem. T.T.L. has received honoraria from Medtronic. R.vE., P.C., and D.M.W. declare no competing financial interests exist.
T.T.L. and B.A.B. designed the study, researched data, and wrote the manuscript. D.B.K, A.R., J.H., B.G, M.C., N.K., R.vE., P.C., and D.M.W. reviewed the manuscript. B.A.B. is the guarantor of this work and, as such, had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.