
Abstract
Background:
Improved insulin infusion set survival and faster insulin action are important issues for pump users and for the development of an artificial pancreas. The current recommendation is to change infusion sets every 3 days. Our objectives were to determine the effect of lipohypertrophy (LH) on infusion set survival and continuous glucose monitoring glucose levels.
Research Design and Methods:
In this multicenter crossover trial, we recruited 20 subjects (age 28.1 ± 9.0 years) with type 1 diabetes (duration 17.5 ± 8.8 years) and an area of lipohypertrophied tissue >3 cm. Subjects alternated weekly wearing a Teflon infusion set in an area of either LH or non-LH for 4 weeks. Sets were changed after (a) failure or (b) surviving 7 days of use.
Results:
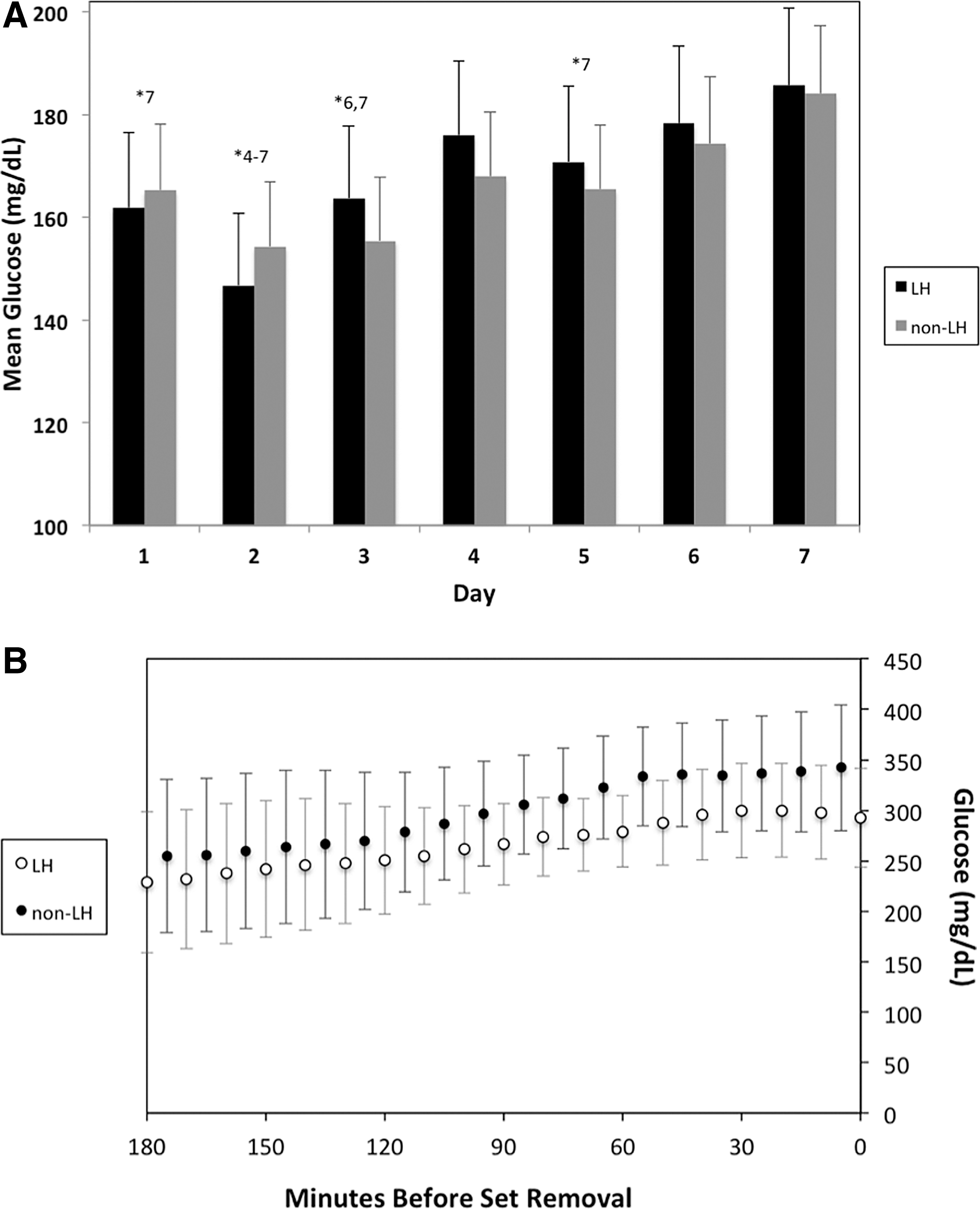
The least-squares mean duration of infusion set survival for sets that lasted <7 days in lipohypertrophied tissue was 4.31 days compared with 4.12 days in nonlipohypertrophied tissue (P = 0.71). The average duration of set survival for individual subjects ranged from 2.2 to 7.0 days. Infusion sets in lipohypertrophied tissue failed due to hyperglycemia in 35% of subjects compared with 23% in nonlipohypertrophied tissue (P = 0.22). Both lipohypertrophied and nonlipohypertrophied tissues displayed a general increase in mean daily glucose after the third day of infusion set wear, but daily mean glucose did not differ by tissue type (P > 0.38 on each day).
Conclusion:
LH did not significantly affect infusion set survival or mean glucose. Achieving optimal infusion set performance requires research into factors affecting set survival. Additionally, the recommendation for duration of set change may need to be individualized.
Introduction
I
Lipohypertrophy (LH) is a local growth of adipose tissue, which is common in regions that receive insulin injections. It occurs primarily due to a hypertrophic effect of insulin on adipose cells. 2,3 Studies evaluating dermatological effects due to infusion sets have measured the prevalence of LH in diabetic youth to be 42%–47%, although lower in older diabetic populations. 4,5 There are other known dermatological complications from frequent insulin injections, such as erythema and subcutaneous nodules. However, LH is especially problematic as it is more common and associated with poor glycemic control. 2 Specifically, LH has been shown to hinder diabetes management by delaying insulin absorption. Becton Dickinson and Profil, Germany, recently presented in abstract form the impact of LH on insulin pharmacokinetics. 6,7 A glucose clamp study indicated that least-squares (LS) mean insulin exposure and insulin pharmacodynamics were lower in LH tissue. 6 Mean postprandial blood glucose was more pronounced in LH sites compared with non-LH. 7 –9
Research into infusion set performance in LH tissue is limited, especially in infusion sets used for longer than 3 days of use. In this crossover study, we generated infusion set failure data by extending site use up to 7 days and studied the duration of infusion set survival in the presence of LH. We hypothesized that LH would decrease the duration of infusion set survival and increase continuous glucose monitoring (CGM) glucose levels when compared with non-LH tissue.
Research Design and Methods
Subjects were enrolled in a prospective, multicenter crossover study at Stanford University and the Barbara Davis Center at the University of Colorado. The institutional review boards of both centers approved the protocol.
Subjects were eligible to participate if they were 12 to 45 years old with clinical diagnosis of having T1D for at least 1 year, on insulin pump therapy for at least 3 months with hemoglobin A1c ≤10%, and had two areas of moderate LH each measuring at least 3 cm in diameter. 3,10 Patients with a history of hypoglycemia unawareness, adhesive allergies, or currently using furosemide, benzodiazepines, phenytoin, dopamine, or alpha agonist drugs were excluded from enrollment. Females were required to have a negative serum pregnancy test before enrollment. All subjects provided written informed consent and assent for minors before enrollment.
At the enrollment visit, subjects were provided with study supplies, including Dexcom G4® Platinum CGM systems, Bayer Contour® Next glucometer, and Precision Xtra® ketone meters. Subjects used their personal insulin pump and insulin (Humalog®, NovoLog®, or Apidra®) as usual with Silhouette® or Comfort™ Short 13 mm Teflon infusion sets inserted at 20–45° angle. Subjects wore each pump infusion set for 1 week or until infusion set failure, defined by (a) the presence of serum ketones >0.6 mg/dL with glucose >250 mg/dL (in the absence of illness); (b) failure of a correction dose to lower the glucose by 50 mg/dL for meter glucose >250 mg/dL; or (c) signs of infection at the infusion site (i.e., erythema or induration >1 cm in diameter). After the initial enrollment visit, subjects returned weekly for 4 weeks.
Two unblinded Dexcom G4P CGMs were worn simultaneously: one in an area of LH, the second in normal tissue for up to 2 weeks. Subjects were educated on CGM use, including calibrating twice daily (before breakfast and before bed), and using only fingerstick glucose readings for all diabetes treatment decisions. Threshold alarms were set at 70 and 250 mg/dL, and rate-of-change alarms were deactivated. Subjects were required to check blood glucose through Bayer Contour Next meters a minimum of four times daily and to check blood ketones for any meter glucose >250 mg/dL.
Sixty-eight subjects were initially approached for this study. There were seven screening failures where investigators did not find LH measuring at least 3 cm. Of the remaining 61 subjects, 29 patients were enrolled in a primary study evaluating CGM performance that only required one area LH.
3
Only 20 of these subjects had two areas of LH and were therefore included in this present study of infusion set performance. Subjects had at least two areas of LH and participated for a total of 4 weeks. To account for intrasubject variability, each subject had two standard and two LH weeks of infusion set wear (Supplementary Fig. S1; Supplementary Data are available at
Subjects maintained a description log of the infusion set, detailing any pain, redness, or swelling. Erythema and induration were measured in millimeters with a ruler. For any meter blood glucose >250 mg/dL more than 2 h since last meal bolus, subjects were asked to assess for infusion set failure by (a) checking blood ketones, (b) giving a correction bolus and refraining from eating carbs for the next hour, and (c) rechecking meter blood glucose in 1 h. Subjects changed the infusion set if the ketones were >0.6 mmol/L, the meter blood glucose failed to decrease by at least 50 mg/dL 1 h after the correction bolus, or if there was evidence of infection at the infusion site (≥1 cm of redness, swelling, or firmness).
At each weekly study visit, infusion and CGM insertion sites were examined by study staff, erythema and induration measured, and photographs taken for any significant changes. Insulin pump, blood glucose meter, ketone meter, and CGM readings were downloaded at each visit. The subjects then had a new infusion set inserted into either LH or non-LH tissue on alternating weeks.
Statistical analysis
The main goal of this study was to evaluate whether the use of LH tissue for infusion set placement affects duration of infusion set wear and daily glucose levels. Survival curves in the two groups (LH and non-LH) were initially compared using the nonparametric log-rank test. However, because the log-rank test assumes that observations are independent, a sensitivity analysis was performed (Fig. 1) using a marginal model approach, 11 which allows correlated survival times. Next, we compared duration of infusion set survival in sets that failed before 7 days of wear.

Each infusion set week was categorized into one of the following reasons for removal: (a) Survival after 7 days of wear, (b) Hyperglycemia with failure to correct by 50 mg/dL, (c) Mechanical failure (site pulled out, leaking insulin, or adhesive failure), (d) Pain, irritation, bleeding, or suspected infection, and (e) Unknown. We used the chi-square test to compare reasons for removal in the two tissue conditions.
The secondary goal of this study was to evaluate the effect of LH on control of blood glucose. Subjects had two CGMs inserted per study protocol. In this data analysis, we chose the CGM with the most recorded data. We have previously published that CGM function is not adversely affected by being inserted in LH tissue. 3 We determined daily mean glucose. To evaluate glucose variability, we calculated the coefficient of variation (CV), % time spent with glucose <70, 70–180, and >180 mg/dL (Supplementary Table S1). Additionally, MAGE was calculated using an SAS program provided by Gregory Jenkins at The Mayo Clinic. 12 For these outcomes, we only included data from infusion sets that survived all 7 days to get an accurate representation of glycemic control in functioning sets (n = 30) and to exclude days where there was hyperglycemia due to an infusion set failure. Daily mean glucose and glucose variability values were calculated for each day after infusion set insertion. Day 1 refers to hours 0–24 after infusion set insertion; day 2 refers to hours 24–48; etc. Differences between LS means for mean daily glucose were determined for each pair of days (day 1 vs. day 2, day 1 vs. day 7, etc.).
Finally, we evaluated the characteristics of the glucose profiles leading up to infusion set failure, specifically due to hyperglycemia (>250 mg/dL) with failure to correct by at least 50 mg/dL in 1-h (n = 23). CGM data were obtained for the time period immediately before instances of infusion set removal due to hyperglycemia. To characterize glucose curves immediately before infusion set failure, we calculated mean glucose, slope, and peak glucose for CGM readings in both the 1- and 3-h time periods before infusion set removal.
Because each subject participated in both the LH and non-LH groups, mixed-effects models were fit to the data. Therefore, we report LS means from the repeated-measures models. For duration of infusion set survival and MAGE, the unit of analysis was infusion set, and the model contained a fixed effect for LH and a random effect for subject. For glucose profiles and daily mean glucose, CGM was the unit of analysis, and the model contained a fixed effect for LH and random effects of infusion set nested within subject. Mixed-effects models were not completed for the remaining glucose variability values (CV, % time in <70, 70–180, and >180 mg/dL).
The study was powered based on an earlier study involving 20 subjects who were asked to wear four infusion sets for 7 days. 13 The mean duration of wear was 5.5 days with a standard deviation (SD) of 1.9 days. We considered a 1-day difference in infusion set wear to be clinically significant, and using a paired t test with a power of 0.8 and α of 0.05, we would require a sample size of 31 weeks. We therefore planned on 40 weeks of wear for each infusion set to account for dropouts. In our previous study, we had detected a propensity for some subjects to be able to wear infusion sets longer than other subjects. To account for this subject effect, we asked each subject to wear each infusion set twice, so there would be 80 weeks to evaluate.
Results
Twenty subjects (8 at Barbara Davis Center and 12 at Stanford University) completed the 4-week study, leading to 40 weeks with sites in LH tissue and 40 weeks with sites in non-LH tissue for 80 total weeks of infusion set wear. Mean subject age ± SD was 28.1 ± 9.0 years, body mass index was 26.3 ± 4.8, duration of diabetes was 17.5 ± 8.8 years, HbA1C was 7.3% ± 0.8%, insulin dose was 0.7 ± 0.3 μ/kg/day, and diameter of LH was 8.0 ± 4.6 cm.
In 40 weeks of LH set wear and 40 weeks of non-LH set wear, 13 (33%) and 17 (45%) sets survived a full 7 days, respectively (P = 0.36, Table 1). The LS mean duration of infusion set wear before failure in LH tissue was 4.31 days and in non-LH tissue was 4.12 days (P = 0.47 with log-rank test, P = 0.45 with marginal model approach). Figure 1 shows the estimated survival curves in the two groups. While the mean duration of set survival did not depend on the presence or absence of LH, duration of survival varied greatly between individual subjects (Fig. 1B).
Shown above is the distribution of results from infusion set weeks. The reason for removal of each site was categorized into (a) Surviving 7 days of wear, (b) Failure to correct hyperglycemia (>250 mg/dL) by at least 50 mg/dL in 1 h, (c) Mechanical cause, (d) Pain, irritation, bleeding, or infection, and (e) Unknown. With 20 patients participating for 4 weeks each, n = 40 for LH and n = 40 for non-LH. For each of the frequency distributions, P-values were calculated using a chi-square statistic with one degree of freedom.
LH, lipohypertrophy.
We only included data from infusion sets that lasted the full 7 days for our analysis of daily mean glucose and glucose variability (Fig. 2, Supplementary Table S1). In a model with interaction between LH and day, the interaction term was not significant (P = 0.90), indicating that the tissue types did not have a significantly different trend in mean glucose over time. Independent of tissue type, the LS mean of daily glucose was significantly lower on day 1 than 7 (P = 0.003), 2 than 4 (P = 0.0026), 2 than 5 (P = 0.014), 2 than 6 (P = 0.0003), 2 than 7 (P < .0001), 3 than 6 (P = 0.014), 3 than 7 (P = 0.0002), and 5 than 7 (P = 0.015). Figure 2 shows this effect of day of wear on mean glucose.
The analysis of daily MAGE was also done on only the infusion sets that survived the full 7 days, with the exception of one non-LH week in which there were not enough CGM readings to run the MAGE program (n = 13 for LH and n = 16 for non-LH). The P-values on days 1 through 7 were 0.66, 0.63, 0.59, 0.29, 0.31, 0.60, and 0.37. In a model with interaction between LH and day, the interaction term was not significant (P = 0.86), indicating that LH did not result in a significantly different trend in mean MAGE over time. There were no significant differences in MAGE between days.
Of the 50 sets that failed, 23 (14 in LH tissue and 9 in non-LH tissue) failed specifically due to hyperglycemia as defined in the protocol (glucose >250 mg/dL with failure to correct by 50 mg/dL 1 h after correction dose). After failure, these sets were immediately removed. Glycemic profiles were determined from these instances in both 1- and 3-h periods before infusion set removal (Fig. 2B, Supplementary Table S2). We had to remove one non-LH instance from the 1-h period because CGM output was insufficient. During hyperglycemic set failure, the LH was significantly different from non-LH in terms of mean glucose (P = 0.0004) and max glucose (P = 0.0005) in the 1-h period, but not the 3-h period. Although there were more hyperglycemic set failures in LH compared with non-LH tissue, hyperglycemia was significantly less severe in these instances.
Discussion
Our goal in this study was to capture infusion set failure data by having subjects wear infusion sets for up to 7 days. It is possible that with a larger sample size statistical significance could have been achieved between the two groups, but we question whether this statistical significance would be clinically relevant. We expected duration of set survival to be lower in LH tissue, but our data did not support this hypothesis. The survival curves of LH and non-LH tissues (Fig. 1) were not significantly different.
LH tissue has been considered a factor affecting infusion set performance due to its tendency to slow insulin absorption. 6,7,14 It has also been reported that LH may cause inconsistent insulin pharmacokinetics. 15 We did not find a significant difference for either daily mean glucose or MAGE in functional infusion sets that were inserted into LH compared with non-LH tissue. Independent of tissue, there were significant mean glucose differences based on the day of wear (Fig. 2). These results were generally consistent with the finding that local blood flow at an infusion site increases in the first 3 days (leading to accelerated insulin pharmacokinetics), but decreases after that. 16 Our results agree with the past literature that on average, day 3 is an appropriate recommendation for changing infusion sets, 16 –20 although individual variations exist.
Our study protocol defined failure to correct hyperglycemia as a meter blood glucose reading of >250 mg/dL with corresponding failure of an insulin correction dose to reduce blood glucose by >50 mg/dL in the following hour. With a 1-h time constraint before set failure, we anticipated that slow rates of insulin absorption would reduce the ability to correct. Based on the evidence for slower insulin absorption in LH tissue, 6,7,14 we hypothesized that there would be more infusion set failures in LH tissue due to hyperglycemia compared with non-LH tissue, but this was not observed. Remarkably, the glucose profiles during infusion set failures showed significantly more hyperglycemia in non-LH infused tissue (Supplementary Table S2). One potential explanation for this is a greater depot of insulin in LH tissue, which blunted a rapid rise in glucose levels when there was an infusion set failure. This residual depot insulin in LH tissue may have also decreased the peak glucose levels observed during an infusion set failure.
Research into duration of infusion set life to support the 48–72-h recommendation initially stemmed from multiple cases of serious infection due to prolonged infusion set wear. 1 The first involved an 11-year-old female who developed toxic shock syndrome from a Staphylococcus aureus infection after leaving her infusion set in for up to 10 days. 21 Another was a case of death due to bacterial endocarditis that started at the site of infusion set insertion. 22 We expected increased infusion set life to increase the risk for site infection. There was a higher occurrence of infections in the LH group compared with the non-LH group (3 vs. 1). This difference was not significant (P = 0.30), but this study was underpowered to assess the relative risk of this endpoint. Additionally, small nodularities were palpated in LH tissue of some of the subjects with larger LH, raising the possibility of scar tissue or abscesses as a source of infection.
A recent study of infusion set wear for 5 days found that site intolerance, such as itching, bruising, swelling, and pain, appears to happen on or after the third day of infusion set use. 17 Additionally, mean daily blood glucose has been documented to increase with the number of days of infusion set use. 16 –20 We have found that there is considerable variability in the duration of set survival for individual subjects in this study (Fig. 1B). Seven of our 20 subjects had all four sets survive at least 4 days. In a previous study, 13 the recommendation for duration of set change may need to be individualized for each patient.
Engineering into preserving infusion set life has investigated tube kinking 23,24 and Gendine coating to prevent infection. 25 Part of the reduction of patient burden in the closed-loop AP project involves increasing the life span of both infusion set and CGM sites. 26 One possibility is that diabetes care in the future will involve a single site that contains an infusion catheter and a CGM. 27 In fact, the MiniMed Duo combined system achieved adequate clinical CGM accuracy on subjects in a home setting. 28 CGM survival is minimally affected by LH tissue, and CGM sites last longer than infusion sets. 3,28 Thus, a major limiting factor for patient use of a combined device will be the life span of infusion catheters.
Conclusion
In this study, LH did not have a significant effect on mean duration of infusion set survival or the frequency of infusion set failure due to hyperglycemia. Previous research has documented slower insulin pharmacokinetics in LH tissue, and avoiding placement of infusion sets in LH tissue is standard clinic advice. We did not see a difference in mean glucose values when subjects were using an infusion set in LH or non-LH tissue. The insulin absorption may have been slower in LH tissue, but the multiple factors affecting daily glucose levels, such as meal composition, carbohydrate counting, and exercise, may have masked the effect of insulin pharmacodynamics in LH tissue. The daily mean glucose measurements of subjects supported the recommendation of changing the infusion site every 3 days, but we found significant variability between subjects and the time gap between site changes may need to be adjusted for each individual patient.
Footnotes
Acknowledgments
The authors would like to acknowledge the JDRF (Grant 17–2013-471) and the CTSA program, funded by the National Center for Advancing Translational Sciences (Grant Number UL1 TR000093) at NIH. For his postdoctoral research, Dr. DeSalvo received grant support from Stanford's Child Health Research Institute (CHRI) and JDRF Postdoctoral Fellowship (Grant 2-PDF-2014–114-A-N). Finally, Andrew Karlin received grant support from the NIDDK Medical Student Research Training Supplement (Grant T32).
Author Disclosure Statement
R.P.W. is a consultant for Medtronic and receives research support from Novo Nordisk. D.M.M. is on the advisory board for Insulet and consults for Abbott and both R.P.W.'s and D.M.M.'s institution has received research support from Medtronic, Dexcom, and Roche. B.A.B. is on medical advisory boards for Sanofi, Novo-Nordisk, BD, UnoMedical, and Medtronic and has received research grant and/or material support from Medtronic, Dexcom, Bayer, UnoMedical, and Tandem. Greg Forlenza has received research support from Medtronic. A.W.K., T.T.L., L.P., L.M., D.J.D., S.L.P., S.H., and P. C. have no conflicts to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.