
Abstract
Background:
Sensor-augmented pump therapy (SAPT) with a predictive algorithm to suspend insulin delivery has the potential to reduce hypoglycemia, a known obstacle in improving physical activity in patients with type 1 diabetes. The predictive low glucose management (PLGM) system employs a predictive algorithm that suspends basal insulin when hypoglycemia is predicted. The aim of this study was to determine the efficacy of this algorithm in the prevention of exercise-induced hypoglycemia under in-clinic conditions.
Methods:
This was a randomized, controlled cross-over study in which 25 participants performed 2 consecutive sessions of 30 min of moderate-intensity exercise while on basal continuous subcutaneous insulin infusion on 2 study days: a control day with SAPT alone and an intervention day with SAPT and PLGM. The predictive algorithm suspended basal insulin when sensor glucose was predicted to be below the preset hypoglycemic threshold in 30 min. We tested preset hypoglycemic thresholds of 70 and 80 mg/dL. The primary outcome was the requirement for hypoglycemia treatment (symptomatic hypoglycemia with plasma glucose <63 mg/dL or plasma glucose <50 mg/dL) and was compared in both control and intervention arms.
Results:
Results were analyzed in 19 participants. In the intervention arm with both thresholds, only 6 participants (32%) required treatment for hypoglycemia compared with 17 participants (89%) in the control arm (P = 0.003). In participants with a 2-h pump suspension on intervention days, the plasma glucose was 84 ± 12 and 99 ± 24 mg/dL at thresholds of 70 and 80 mg/dL, respectively.
Conclusions:
SAPT with PLGM reduced the need for hypoglycemia treatment after moderate-intensity exercise in an in-clinic setting.
Introduction
I
SAPT with low glucose suspension (Medtronic® Paradigm Veo™ system) suspends basal insulin infusion when the preset sensor hypoglycemic threshold is reached and reduces the depth and duration of nocturnal hypoglycemia 6,7 without an increase in ketosis. 7 The system was also tested with exercise in the In-Clinic ASPIRE study, 8 with a reported reduction in the duration of hypoglycemia after exercise. The development of algorithms that predict impending hypoglycemia based on CGM and suspend basal insulin before sensor glucose falls below the set hypoglycemic threshold offers the additional potential advantage of preventing hypoglycemia. Predictive algorithms were tested earlier on by Buckingham et al. in insulin-induced hypoglycemia and are different from the investigational predictive algorithm tested in our study. 9 –13 We trialled an investigational device with the predictive low glucose management (PLGM) system that has been since incorporated into the Medtronic MiniMed®640G pump (Medtronic MiniMed, Northridge, CA). Despite the commercial availability of the pump, there are only a few studies addressing the effectiveness of predictive algorithms in real clinical situations.
The purpose of this study was to evaluate the efficacy of a predictive algorithm in the prevention of hypoglycemia with moderate-intensity exercise under in-clinic conditions. The need for hypoglycemia treatment was chosen as the primary outcome measure due to its clinical relevance. In patients not requiring hypoglycemia treatment with pump suspension, there was the opportunity to review the safety of the system by monitoring plasma glucose and ketones after pump suspension. We hypothesize that the system will reduce the need for hypoglycemia treatment and will not result in post pump-suspend hyperglycemia or clinical ketosis.
Research Design and Methods
The protocol was designed by the tertiary clinical pediatric diabetes centers involved in the study and was approved by the centers' institutional review board. The exercise studies were conducted at the Children's Clinical Research Facility at Princess Margaret Hospital, Perth as a randomized, controlled cross-over study.
PLGM system
To test the predictive algorithm, an investigational device was used, comprising a commercially available Medtronic Paradigm Veo insulin pump, an Enlite™ glucose sensor with a MiniLink™ REAL-Time transmitter (Medtronic MiniMed) that transmitted sensor glucose at 5 min intervals, a BlackBerry® Storm smartphone (Waterloo, ON, Canada) that contained the PLGM software, and a Medtronic custom-built radiofrequency translator that established communication between the insulin pump and the BlackBerry phone. This is referred to as the PLGM system. 14 The modifiable parameters were the hypoglycemic threshold and the prediction horizon, and these were set by the investigator for the study. The hypoglycemic threshold is the predicted sensor glucose reading at which pump suspension occurs, and the prediction horizon is the time taken to reach the hypoglycemic threshold. In the study, the prediction horizon was set at 30 min, and the sensor hypoglycemic threshold was studied at two values: 70 and 80 mg/dL.
The device suspended basal insulin infusion when the difference between sensor glucose and the hypoglycemic threshold was less than 50 mg/dL, and sensor glucose was predicted to reach the set threshold in 30 min. The insulin delivery was suspended initially for a fixed period of 30 min (Zone 1). Basal insulin remained suspended for up to a maximum period of 90 min based on current and predicted sensor glucose readings (Zone 2) and thereafter resumed insulin delivery (auto-resumption) for a minimum of 30 min after the end of the suspend period (Zone 3). Resumption of insulin delivery occurred after a maximum suspend period of 2 h or earlier if the auto-resumption parameters were met. Auto-resumption occurred once the current sensor reading was 20 mg/dL more than the set hypoglycemic threshold and was predicted to be 40 mg/dL more than the set hypoglycemic threshold in 30 min.
Subjects
Twenty-five participants fulfilling the following criteria were recruited: age 12–25 years, diagnosis of type 1 diabetes for at least 1 year, HbA1c less than 10% (86 mmol/mol), and using continuous subcutaneous insulin pump therapy for at least 6 months. Exclusion criteria included medical conditions predisposing to hypoglycemia, severe hypoglycemia (coma/convulsion) in the preceding 3 months, or a history of known or suspected coronary artery disease. Written informed consent was obtained from participants aged 18 years and older, and written parental consent and participant assent were obtained for those younger than 18 years.
Study protocol
This was a randomized, controlled cross-over study with participants studied on 2 separate days: a control day with SAPT alone and an intervention day with SAPT and PLGM activated. Randomization to the order of study was computer generated using
Preliminary testing
At least 3 days before their first study, the participants completed an exercise test to determine their peak rate of oxygen consumption (VO2 peak). This involved cycling on a stationary bike (Corival; Lode BV, Groningen, The Netherlands) while breathing through a mouthpiece connected to an indirect calorimetry system. The participants cycled against a resistance that increased every 3 min until they could no longer maintain the required workload. The VO2 peak was determined from the calorimetry data.
In the week before the first study day, the participant's glucose profile based on self-monitoring capillary blood glucose testing and/or sensor glucose, if available, was reviewed for optimization of basal rates. This involved skipping breakfast and monitoring hourly blood glucose levels to mid-morning to adjust basal rate as necessary. Participants were advised to maintain a similar diet and activity before both study days. They were instructed to avoid rigorous physical activity in the 24 h period leading to the study. Female participants were studied in the follicular phase of the menstrual cycle. The interval between 2 study days was greater than 72 h. Insulin pump sites were changed on the day before the study. An Enlite sensor was inserted in the gluteal region on the day before the study, and real-time continuous glucose monitoring (RT-CGM) was commenced. The first calibration was after 2 h of sensor insertion, and the second calibration was within 6 h of the initialization. A repeat calibration was performed in the morning before the study.
Testing sessions
The participant was fasted from midnight on the study day to reduce glycemic excursions related to food. The study was cancelled and rescheduled if the participant had capillary blood glucose below 63 mg/dL (3.5 mmol/L) on the morning of the study. The participant arrived at the center at 8 am. Two intravenous catheters were placed in a vein of the forearm or dorsum of the hand for blood sampling and for administration of insulin or glucose if necessary. An intravenous insulin correction bolus was administered if plasma glucose was higher than 126 mg/dL (7 mmol/L), and exercise began after 90 min of insulin administration if plasma glucose remained stable during this period. Similarly, if plasma glucose was <90 mg/dL (5 mmol/L), bolus intravenous glucose was administered and exercise began at least 30 min after infusion with stable glucose levels. Once euglycemia was achieved with plasma glucose between 99 and 117 mg/dL (5.5–6.5 mmol/L) for at least 30 min, only on the participant's basal subcutaneous insulin infusion (with no residual effect of parental insulin or glucose bolus), the participant commenced moderate-intensity exercise.
Moderate-intensity exercise comprised two 30-min sessions of cycling, with a rest phase of 30 min in between the two sessions. The participants cycled on the same ergometer used for VO2 peak testing at 55% of their previously determined VO2 peak which corresponds to moderate-intensity exercise, a known hypoglycemic stimulus. 14 This standardized exercise intensity was reproduced on both study days. This exercise design was chosen over the more prolonged continuous exercise sessions as in real life, many individuals find it difficult to adhere to this exercise regime. Hence, our study was designed to replicate a more real-life scenario to suit the average nonathletic individual but at the same time, based on our previous experience, be rigorous enough to induce hypoglycemia.
Sensor alarms were turned off during the study, and the participants were discouraged from observing the pump screen monitor. During the study, participants were asked to report for symptoms of hypoglycemia and plasma glucose was monitored every 10 min and every 5 min once plasma glucose was <63 mg/dL. Exercise was ceased, and participants were treated with 15–20 g of oral carbohydrate 15 if plasma glucose reached 50 mg/dL (2.8 mmol/L) or if they reported symptoms of hypoglycemia with plasma glucose <63 mg/dL. If the end points mentioned earlier were not met on the control day, the plasma glucose nadir was monitored and the study was stopped once two consecutive plasma glucose values trended upward after completion of exercise. Treatment with oral carbohydrate was provided if plasma glucose was <72 mg/dL (4 mmol/L) at the end of the study.
The hypoglycemic threshold was set at 70 mg/dL (3.9 mmol/L) for the first 10 studies and was set at 80 mg/dL (4.4 mmol/L) for the remaining studies. In the intervention arm, the pump suspended insulin infusion when the algorithm predicted that the sensor glucose would be below the set threshold in 30 min. The plasma glucose profile was monitored during the entire period of pump suspension and for at least 30 min after pump resumption. Plasma glucose >180 mg/dL (10 mmol/L) was defined as hyperglycemia after postpump suspend. Blood ketones were monitored on both control and intervention days. On the control day, ketones were monitored before commencement of exercise and at the end of the study. On the intervention day, ketones were monitored before exercise and every 30 min after pump suspension. Blood was collected at the commencement of exercise and at the plasma glucose nadir on both days, and it was assayed for free plasma insulin. On the intervention day, additional samples for free insulin were also taken at the time of pump suspension and resumption.
The primary outcome was the need for hypoglycemia treatment both with and without PLGM. This was defined as plasma glucose <50 mg/dL with or without symptoms of hypoglycemia, plasma glucose <63 mg/dL with symptoms of hypoglycemia, or plasma glucose <72 mg/dL at the end of the study. The other outcomes measured were ketone levels and the 2-h plasma glucose after pump suspension on the intervention day.
Analysis
During exercise, blood samples were collected at regular intervals for plasma glucose and lactate measurements, and the rates of oxygen consumption and carbon dioxide production were measured using an indirect calorimetry system (VMax Spectra; SensorMedics Corp., Yorba Linda, CA). Plasma glucose and lactate were analyzed during the study using the YSI 2300 STAT PLUS Glucose and Lactate Analyzer (Yellow Springs Instrument, Yellow Springs, OH). Plasma insulin was measured with a noncompetitive chemiluminescent immunoassay (Architect i2000SR; Abbott Laboratories, Abbott Park, IL). Ketones were monitored with an Abbott Diabetes Care Optium Xceed meter with Freestyle ketone test strips.
Dichotomous variables were analyzed using McNemar's test, and continuous variables were analyzed using a two-way (time × treatment) repeated-measures ANOVA with Fisher's least significance difference test for a posteriori analysis using SPSS software (SPSS, Chicago, IL). Statistical significance was accepted at P < 0.05. Results are expressed as mean ± standard deviation (SD).
Results
Twenty-five participants (13 males and 12 females) were studied. The age was 15.7 ± 3.1 years, duration of diabetes was 8.5 ± 4.6 years, BMI was 24 ± 7.7 kg/m2, HbA1c was 7.8% ± 0.7% (62 mmol/mol), and total daily insulin was 0.9 ± 0.2 units/kg/day.
In six participants, the predictive hypoglycemic threshold for the system was not reached after exercise on the intervention day and these participants were excluded from analysis (both study days). In four of these participants, the decline in plasma glucose with exercise was not sufficient to reach the preset hypoglycemic threshold. Although the remaining two participants required hypoglycemia rescue treatment on the control day, problems with the insulin infusion site and an early upper respiratory tract infection caused higher plasma glucose levels on the intervention day and exclusion of these studies. The results provided are, therefore, for the 19 participants who met the hypoglycemic threshold with resultant pump suspension.
Hypoglycemia rescue treatment
The results of the need for hypoglycemic treatment with both thresholds are summarized in Table 1. Evaluating both thresholds together, hypoglycemia treatment was required in 17 of the 19 participants (89%) with SAPT alone compared with 6 of the 19 participants (32%) with SAPT and PLGM activated (P = 0.003). Of these six, four participants (two in each threshold) required treatment as plasma glucose reached <50 mg/dL on the intervention day. On the control day, of the 17 participants who required treatment, 11 participants required treatment after exercise whereas 6 participants required treatment during exercise. On the intervention day, of the six participants who required treatment, three participants required treatment during exercise and three required treatment after exercise.
Seventeen of the 19 participants (89%) with SAPT alone compared with 6 of the 19 participants (32%) with SAPT and PLGM activated (P = 0.003) required treatment for hypoglycemia.
PLGM, predictive low glucose management; SAPT, sensor-augmented pump therapy.
Irrespective of the need for hypoglycemia treatment, with the PLGM threshold of 70 mg/dL, the lowest plasma glucose (nadir) was achieved after 101 ± 53 and 102 ± 41 min after commencement of exercise on the control and intervention days, respectively (P = 0.96). Similarly, with the threshold of 80 mg/dL, the nadir was reached at 134 ± 51 min on the control day and 118 ± 36 min on the intervention day (P = 0.36). A nadir <63 mg/dL was reached in 95% of participants after exercise on the control day. On the intervention day, 90% of participants with the threshold of 70 mg/dL reached <63 mg/dL, whereas only 44% of participants with the threshold of 80 mg/dL had a plasma glucose <63 mg/dL. The plasma glucose profiles of participants on thresholds of 70 and 80 mg/dL are demonstrated in Figure 1, whereas Figure 2 demonstrates the recovery of plasma and sensor glucose after pump suspension in participants on a threshold of 80 mg/dL.

Plasma glucose profile with PLGM on and off. Figure 1A and 1B demonstrate the mean plasma glucose profile on thresholds of 70 mg/dL (n = 7) and 80 mg/dL (n = 6) respectively. Participants who required treatment for hypoglycemia on the intervention day were not included in this analysis. E1 and E2 symbolize the exercise sessions. Plasma glucose was significantly higher at time point 140 min only (*P < 0.05). PLGM, predictive low glucose management.
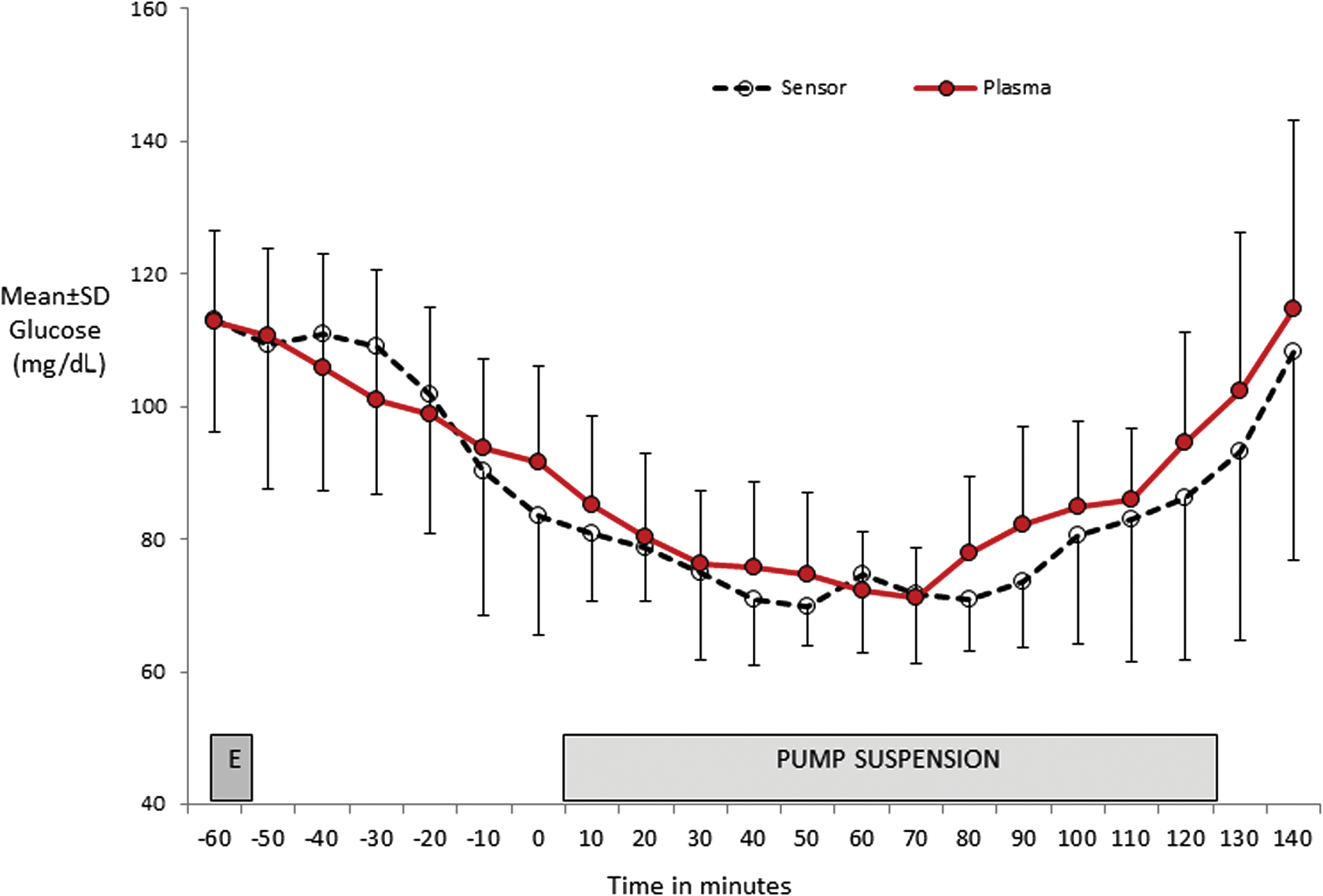
Plasma and sensor glucose profile with PLGM on a threshold of 80 mg/dL. Mean time to pump suspension from commencement of exercise is 62 ± 22 min. Pump suspension is time 0, and the graph shows recovery of plasma and sensor glucose after pump suspension. E, commencement of exercise.
Pump suspension and resumption
The pump resumed basal infusion after a 2-h fixed suspend period in 11 participants. In two participants, the pump resumed before 2 h based on the auto-resumption parameters. The plasma and sensor glucose levels after 2 h of pump suspension are demonstrated in Table 2. The pump suspended at 67 ± 34 min after commencement of exercise with the threshold set at 70 mg/dL. The plasma glucose at suspension was 68 ± 12 mg/dL, resulting in a post-suspension nadir of 56 ± 6 mg/dL. The plasma glucose at pump resumption was 84 ± 12 mg/dL. With the threshold of 80 mg/dL, the pump suspended at 62 ± 22 min after exercise, resulting in a post-suspension nadir of 63 ± 12 mg/dL. Plasma glucose was 99 ± 24 mg/dL at pump resumption.
Pump resumption data are from the 11 participants after the maximum 2-h pump suspend. Glucose values are provided in mean ± SD (range).
*P < 0.05 significant.
Ketonemia
The ketone level [mean ± standard error (range)] at the commencement of exercise on both study days was 0.11 ± 0.04 (0.1–0.2) mmol/L. At the end of the study, the ketone level on the control day was 0.28 ± 0.12 (0.1–0.4) mmol/L (P = 0.002). On the intervention day, the ketone levels at the time of pump suspension and pump resumption were 0.22 ± 0.17 (0–0.6) mmol/L and 0.69 ± 0.41 (0.1–1.4) mmol/L, respectively (P < 0.001). On the intervention day, four subjects had ketonemia between 1 and 1.5 mmol/L at the end of the study, with the corresponding plasma glucose level between 68 and 103 mg/dL. Five subjects had ketonemia between 0.6 and 1 mmol/L, with the corresponding plasma glucose level between 95 and 115 mg/dL. None of these participants had any symptoms of ketosis, and the ketone level was <0.5 mmol/L after 2 h of post-pump resumption and meal bolus.
Pre-exercise plasma glucose
Participants had a similar baseline plasma glucose before commencement of exercise on both control and intervention days with both thresholds (control 70 mg/dL vs. 80 mg/dL; P = 0.09, intervention 70 mg/dL vs. 80 mg/dL; P = 0.15). On a threshold of 70 mg/dL, the plasma glucose was 98 ± 10 and 100 ± 14 mg/dL on the control and intervention days, respectively (P = 0.2); whereas the plasma glucose was 105 ± 11 and 107 ± 13 mg/dL with a threshold of 80 mg/dL (P = 0.17).
Plasma insulin
The plasma insulin levels before the commencement of exercise and at the end of the first and second sessions of exercise on the control day were 227.4 ± 50.4, 260 ± 43.9, and 279.6 ± 73.8 pmol/L; whereas on the intervention day, they were 219.1 ± 46.9, 252 ± 43.4, and 268.2 ± 73.2 pmol/L. There were no differences between plasma insulin levels at any of these time points (P > 0.05). Plasma insulin at pump suspension was 225 ± 153.1 pmol/L and at pump resumption, it was 102.9 ± 98 pmol/L (P < 0.01).
Discussion
The PLGM system reduced the need for hypoglycemia treatment after moderate-intensity exercise in a controlled setting under basal insulin conditions. Under such conditions, the system reduced the need for treatment of hypoglycemia, irrespective of the preset hypoglycemic threshold. Furthermore, the system was not associated with hyperglycemia or clinical ketosis on pump resumption. Although the system reduced exercise-induced hypoglycemia, it did not prevent hypoglycemia in all subjects. If home trials in free-living conditions confirm the same degree of efficacy, then the system has the potential to reduce the fear of hypoglycemia and to enable patients with type 1 diabetes to exercise more safely.
The use of RT-CGM to inform patients on exercise-related glycemic excursions has been promising. Fewer episodes of exercise-induced hypoglycemia were reported with the use of low alerts with RT-CGM 16,17 and the development of an algorithm to guide carbohydrate intake based on CGM readings. 18 Automated insulin suspension with sensor-detected hypoglycemia (≤70 mg/dL) was evaluated in the in-clinic ASPIRE study in adults. The study used the Medtronic Paradigm Veo system with low glucose suspend (LGS) function in the setting of nonstandardized exercise, and reported a 19% reduction in the time spent in hypoglycemia after exercise with LGS-on than with LGS-off. The participants exercised till the plasma glucose was <85 mg/dL and were observed for 4 h (hypoglycemia treatment if plasma glucose was <50 mg/dL) after the study. 8 The PILGRIM study evaluated the PLGM function in virtual patients with subcutaneous insulin bolus and in real-life participants with exercise. 19 The study used computer simulation under in silico conditions and demonstrated a significant reduction in the time spent in hypoglycemia with PLGM than with LGS when virtual participants were administered a manual insulin bolus to induce hypoglycemia. The study also tested the algorithm in real-life patients with exercise and concluded that the system prevented a blood glucose <63 mg/dL in 12 of the 15 patients (80%) after exercise. The limitations of the study were the absence of a control arm, variable exercise duration, and the use of capillary glucose monitoring (Hemocue) as a secondary end point. In the absence of a control arm, it is difficult to determine the efficacy of the algorithm. Hence, our study, which uses the same algorithm, was intended to design an exercise session that could induce hypoglycemia and, therefore, was able to compare the effectiveness of PLGM in reducing hypoglycemia. Our study is the first randomized, controlled study to report the efficacy of the PLGM algorithm in the reduction of exercise-induced hypoglycemia under standardized conditions.
The need for hypoglycemia treatment was reduced with thresholds of both 70 and 80 mg/dL, although prevention of hypoglycemia was more likely with a threshold of 80 mg/dL. This is because even with PLGM, almost all participants had plasma glucose below 63 mg/dL with a threshold of 70 mg/dL as compared with half the participants with a threshold of 80 mg/dL. However, pump suspension prevented a further decline in plasma glucose and the need for hypoglycemia rescue treatment. The PILGRIM study that was published since this study was designed used the threshold of 80 mg/dL after hypoglycemia with rapidly falling glucose levels with a threshold of 70 mg/dL in the first two participants. 19 We found that plasma glucose was already below 70 mg/dL at the time of pump suspension in 60% of participants when the sensor hypoglycemic threshold was set at 70 mg/dL. This could be due to a time delay in equilibrium between interstitial fluid and plasma glucose. 20 The decline in plasma glucose with our standardized exercise regimen occurred in the latter half of the second phase of exercise. Although the sensor and plasma glucose were equivalent at the beginning of exercise, the sensor overestimated plasma glucose levels during the second phase of exercise. Hence, data from this study suggest that setting a threshold of 80 mg/dL is more likely to reduce hypoglycemia with exercise than a threshold of 70 mg/dL.
This study did not demonstrate hyperglycemia after 2 h of pump suspension. Although ketonemia was demonstrated on the intervention days, this was not associated with a high blood glucose level and was more likely to be the effect of starvation and a prolonged duration of study along with insulin suspension. The mild ketonemia occurred after 14–18 h of fasting and 2 h of pump suspension. Ketones cleared post-pump resumption, after meals and meal bolus, when tested after 2–3 h. Beck et al. also demonstrated the overnight safety of the Kalman filter-based predictive algorithm, with no significant increase in morning ketosis after pump suspension. 21 Our study also contributes to the safety of the PLGM system, with no significant hyperglycemia or clinical ketosis after pump suspension.
In this study, exercise was performed under euinsulinemic basal conditions, and most patients reached their glucose nadir either during the second session of exercise or in recovery. On the control day, most participants required treatment when symptomatic with plasma glucose between 50 and 63 mg/dL and were more likely to benefit from PLGM. However, participants who required treatment as plasma glucose was <50 mg/dL were more likely to require treatment even with PLGM on. Although the study was commenced when the participants were euglycemic, some of the participants had a steeper decline, which can be attributed to the exercise along with the possibly higher basal rates during exercise. This difference highlights that the rate of fall in plasma glucose will guide the PLGM efficacy. As this study addresses the efficacy of the algorithm under a controlled in-clinic state, the ability of the system to cope when exercise is performed under hyperinsulinemic conditions will be more challenging and less likely to prevent hypoglycemia, even with higher hypoglycemic thresholds. This can be further explored when the system is tested in home trials. Another limitation of the study is that we were not able to compare the duration of hypoglycemia in both groups, as our study participants were treated for hypoglycemia when end points of the study were met. The study was not blinded to the participant, and there is a potential of bias in reporting symptoms of hypoglycemia. We were not able to comment on the effect of PLGM on late-onset nocturnal hypoglycemia, as this was an in-clinic study but the system has the potential to reduce the risk of these events when used overnight in the real world.
The strength of this study lies in the ability to compare the need for hypoglycemia treatment both with and without the PLGM system under controlled conditions and to provide clinical insights about the potential of its use in free-living conditions. The PLGM system improved plasma glucose profile with standardized moderate-intensity exercise under controlled in-clinic conditions. However, the ability of this system, in the setting of spontaneous exercise and preprandial meal boluses in real-life scenarios, remains to be determined. Larger randomized, controlled home trials will shed further light on the efficacy and safety of this system when used in a real-life setting. The ability to individualize the hypoglycemic threshold for each individual for different hypoglycemic stimuli further enhances the potential of the system.
To conclude, this is the first randomized, controlled trial demonstrating the efficacy of the PLGM system with moderate-intensity exercise as a hypoglycemic stimulus in an in-clinic setting. The system appears promising at this early stage, with the potential to reduce the risk of immediate hypoglycemia when exercise is performed under basal insulin conditions without significant hyperglycemia or ketosis after pump suspension.
Footnotes
Acknowledgments
This study was funded by the Juvenile Diabetes Research Foundation funded Australian Type 1 Diabetes Clinical Research Network. The Jaeb Centre contributed toward the review of study progress, as part of the JDRF Artificial Pancreas Consortium Network. M.B.A. is the recipient of the Channel 7 Telethon Research Fellowship 2014. Insulin pumps, glucose sensors, and the Blackberry phones were provided by Medtronic via an unrestricted grant. Medtronic had no role in the design and conduct of the study; data collection, analysis, and interpretation of the data; the preparation, review, or approval of the article; and the decision to submit the article for publication.
Authors' Contributions
M.B.A. conducted the studies, collected data, completed the analyses, and wrote the article. R.D. supervised exercise. A.R. and B.G. were involved in the algorithm design, and N.K. provided technical support. M.J.O.G., T.T.L., and R.D. contributed to the design of the study, collected data, and reviewed the article. N.P., P.A.F., J.M.F., G.R.A., B.R.K., F.C., T.W.J., and E.A.D. contributed to the design of the study and reviewed the article. E.A.D. is the guarantor of this work, has access to the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis. The authors recognize and thank the participants and their families for their efforts. They also recognize the work of the diabetes research team at PMH (Perth). They acknowledge the support of Grant Smith, Telethon Kids Institute for providing statistical advice. Parts of this study were presented in abstract form at the ATTD and APEG 2013, APEG and ATTD 2014.
Author Disclosure Statement
T.W.J. received a speaker's bureau honorarium from Medtronic.