
Abstract

A
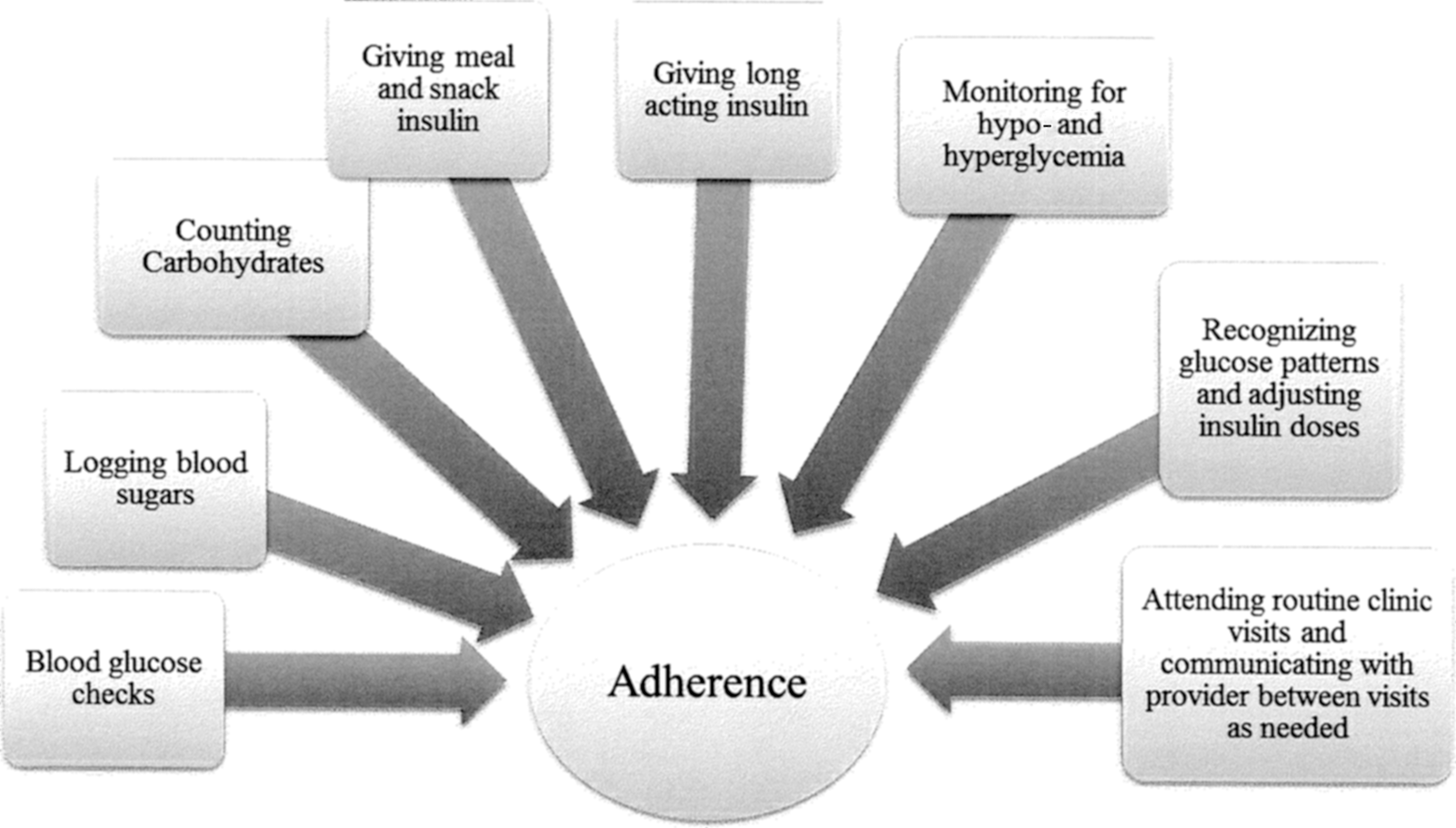
Type 1 diabetes treatment regimen tasks associated with adherence.
The BOLUS score described by Clements et al. 6 is an objective measure of adherence that has the advantage of addressing some of these problems. First, the BOLUS measure captures mealtime insulin administration, which Clements et al. demonstrate is more closely linked to glycemic control than BGM. In their sample, every one-point increase in BOLUS score was associated with a 1.5% decrease in HbA1c level. 6 Similarly, a small study conducted in youth with insulin pumps demonstrated that missing one or more meal boluses per week was related to a 0.8% increase in HbA1c. 7 Further support for the importance of mealtime dosing was revealed in a large sample, comparing youth in excellent glycemic control with those in poor control, in which those who reported never missing insulin boluses were 24.5 times more likely to be in excellent control than poor control. 8 Second, it is unlikely that patients will forget to bring insulin pumps to clinic. Third, the BOLUS is relatively easy to obtain and interpret, making it more likely providers will use it during clinic visits when they are pressed for time.
However, additional research is needed to identify potential problems/pitfalls with the BOLUS measure of adherence. Findings from the Clements et al. article need to be replicated and extended to more diverse samples, as their study sample was 93% white, non-Hispanic. Furthermore, clinical experience suggests that patients may manually calculate their insulin dose, rather than enter the number of carbohydrates consumed into their insulin pump, which would not be captured as a mealtime dose. Similarly, as noted by the authors, adolescents commonly “guesstimate” carbohydrate values, either over- or underestimating carbohydrate grams in a given meal, 9 so that the bolus does not match actual intake, making it a less perfect measure of adherence. Another potential pitfall of the BOLUS measure is that adolescents and young adults may eat more erratically, or snack more often than younger children, especially in the evenings. The BOLUS score is determined by assigning 1 point for each meal that is eaten and dosed with insulin between the hours of 6–10am, 11–3pm, and 4–10pm (three total points can be given per day). Thus, if a patient skips breakfast but appropriately gives meal insulin for lunch and dinner, or skips breakfast and then snacks after 11pm, he/she would never receive >2 points per day, giving an appearance of relative nonadherence. Finally, given the rates of disordered eating behavior in adolescents and young adults with T1D—a recent meta-analytic review found these behaviors to be evident in 39.3% of adolescents with T1D 10 —it is important to consider that some patients may be intentionally withholding insulin. Although the BOLUS score would indicate nonadherence in these patients, the reasoning behind the nonadherence is quite complicated in these cases, and providers should be mindful of the high rates of disordered eating behaviors in this population.
We should also note that the BOLUS measure is only available from insulin pump downloads, which excludes some of the most high-risk populations. Data from national samples have highlighted racial/ethnic disparities in the use of insulin pumps, with insulin pump use higher in white participants (61%) than black or Hispanic patients (26% and 39%, respectively). 11 Furthermore, insurance companies are increasingly requiring documentation of regular BGM (i.e., four times/day) before approving insulin pumps, meaning that those patients who are less adherent are less likely to be prescribed a pump. For patients who do not use insulin pumps, “smart” pens, diabetes apps, and advanced meter technologies are emerging, but these require the user to input blood glucose values and/or carbohydrates, so they do not give reliable and objective evidence of mealtime insulin administration. More work is needed to determine the best measures of adherence for these populations, who may be those at the highest risk for problems with adherence!
Despite these limitations, the BOLUS measure offers promise as a measure of adherence that may be easily interpreted and may provide opportunities for provider-based interventions to improve adherence during clinic visits. 12 Ultimately, the BOLUS score would give providers a tool to assess adherence to therapy, focus on the importance of mealtime insulin administration, and potentially improve the glycemic control of their patients using insulin pumps.
Footnotes
Author Disclosure Statement
No competing financial interests exist.