
Abstract
Background:
No previous studies have investigated the use of a premixed insulin analogue in a hospital setting.
Objective:
To compare the efficacy and safety of treatment with premixed insulin analogue (insulin lispro mix 75/25, LM75/25) with the basal-plus regimen with insulin glargine in hospitalized patients with type 2 diabetes (T2D).
Materials and Methods:
A randomized clinical trial in hospitalized patients with T2D and glucose >140 mg/dL on admission was performed. A total of 54 patients were randomized to receive insulin LM75/25 or glargine. In both groups, a correction dose of lispro was administered before meals. Insulin dose was adjusted to obtain a mean blood glucose (BG) between 100 and 140 mg/dL.
Results:
Improvement in the mean BG after the first day of treatment was similar in both groups (P = 0.470). Glycemic control at the end of follow-up was similar between the group with insulin LM75/25 (131.3 ± 28.4 mg/dL) and insulin glargine (143.8 ± 32.5 mg/dL, P = 0.153). The aim of a BG concentration of <140 mg/dL was obtained in 72% of the patients in the premixed insulin analogue group and 56% of patients in the basal-plus group (P = 0.239). There was no difference in the frequency of hypoglycemia between groups (7 vs. 10, P = 0.529).
Conclusion:
Results of this trial indicate that the use of a premixed insulin analogue is as effective and safe as the basal-plus regimen to achieve glycemic control.
Introduction
D
Despite the benefits of a basal-bolus regimen in improving glycemic control in noncritically ill patients, many healthcare providers are reluctant to integrate this approach into their clinical practice, possibly due to its complexity and the fear of hypoglycemia. 26 –29 Umpierrez et al. compared the basal-bolus scheme with a basal-plus regimen, which consists of a single daily dose of basal insulin with supplemental (corrective) doses of rapid-acting insulin analogues before meals. 30 The basal-plus regimen results in improvement in glycemic control and frequency of hypoglycemic events similar to those seen with a standard basal-bolus insulin regimen. 30,31 However, the basal-plus scheme does not provide prandial coverage of insulin. Therefore, it is necessary to test additional schemes with better basal and prandial insulin coverage and with easy application. One way to achieve this is the use of premixed insulin analogues. Premixed insulin analogues such as insulin lispro mix 25 (75% insulin lispro protamine suspension, 25% lispro, insulin LM75/25) have shown efficacy and safety in the treatment of outpatients with T2D 32 –35 ; however, at this time, no previous studies investigated the use of these agents in a hospital setting. Accordingly, we conducted a prospective, randomized clinical trial to determine the safety and efficacy of insulin LM75/25 with a basal-plus insulin regimen with glargine once daily plus corrective doses with lispro administered according to a sliding scale in the management of hospitalized noncritically ill patients with T2D.
Materials and Methods
In this prospective, open-label, randomized study, we recruited 54 adult patients admitted to the Department of Cardiology of a tertiary-level public hospital in Mexico City. This study was approved by the institutional research ethics committee (registration No. R-2014-3501-35) and was conducted in accordance with the Declaration of Helsinki (2013 version). From March to September 2014, written informed consent was obtained from patients with acute or chronic medical illness who were eligible for the study.
We included patients with a known history of T2D for >3 months and with a BG before randomization between 140 and 400 mg/dL. Subjects were required to eat at least 75% of the indicated diet. Ages were between 30 and 70 years and subjects were being treated at home with diet alone, any combination of oral antidiabetic agents, or low-dose insulin therapy at a daily dose ≤0.4 Us/kg before admission. We excluded patients when BG was >400 mg/dL before randomization, patients admitted to or expected to require intensive care unit (ICU) admission, patients undergoing cardiac surgery, patients receiving corticosteroid therapy, patients with clinically relevant hepatic disease (Child–Pugh score B or C) or impaired renal function (serum creatinine ≥2.0 mg/dL), patients with a history of diabetic ketoacidosis, pregnant patients, and patients with any mental condition rendering them unable to provide informed consent.
The medical problem of all patients in the study was managed by the primary admitting team, and the insulin regimen was managed by the study team. Patients were randomly assigned to receive either insulin LM75/25 regimen or basal-plus regimen with insulin glargine. After randomization, all medications for diabetes were suspended. Patients treated with insulin LM75/25 were started at a total daily dose of 0.2 U/kg for BG concentration between 140 and 200 mg/dL or 0.3 U/kg for those between 201 and 400 mg/dL. Two-thirds of the total daily dose was given before breakfast and one-third before dinner. Total daily dose of insulin LM75/25 was adjusted based on the mean BG to maintain BG between 100 and 140 mg/dL. Supplemental insulin with insulin lispro was given according to a sliding scale before meals for BG >140 mg/dL (Table 1).
Insulin LM75/25, insulin lispro mix 75/25.
BG, blood glucose; TDD, total daily dose.
Patients randomized to basal-plus regimen received insulin glargine at a total daily dose of 0.15 U/kg for a BG between 140 and 200 mg/dL or 0.2 U/kg for a BG between 201 and 400 mg/dL plus corrective doses of lispro before meals for BG >140 mg/dL according to the sliding scale. Insulin glargine dosage was adjusted daily according to BG values to maintain a mean BG between 100 and 140 mg/dL (Table 1).
All patients received a diet calculated to 25 calories/kg per day and distributed as follows: carbohydrates 45%, fat 37%, protein 18%, and sodium <2300 mg/day.
In both groups, BG was measured before each meal and at bedtime using a point-of-care glucose meter (ACCU-CHEK® Performa; Roche, Mannheim, Germany). In addition, glucose was measured at any time if a patient experienced symptoms of hypoglycemia or if requested by the treating physician. Hypoglycemia was defined as BG <70 mg/dL, and severe hypoglycemia was defined as BG <40 mg/dL and treated by standard protocol (Table 1). Patients were excluded from the study if they denied consent, were discharged within <24 h, were transferred to the ICU, or were started on glucocorticoids.
The primary outcome of the study was a difference in glycemic control as measured by mean daily BG concentration among patients treated with insulin LM75/25 or basal-plus regimen. Secondary outcomes included number of patients with BG between 70 and 140 mg/dL, number of patients with mild hypoglycemia (BG <70 mg/dL) and severe hypoglycemia (BG <40 mg/dL), total daily dose of insulin, and length of hospital stay.
The primary endpoint was to assess the differences in mean daily BG between groups. Sample size was calculated based on data from the RABBIT-2 study, 21 from which we hypothesized a mean daily BG difference >30 mg/dL between the basal-plus group versus the insulin LM75/25 regimen in hospitalized patients with T2D. Assuming a within-group standard deviation (SD) of 40 mg/dL with an alpha error rate of 0.05 (one sided) and assuming a 15% dropout rate, we estimated that 25 subjects per group (50 total) will be needed to achieve 80% power.
We compared baseline and clinical characteristics and outcomes between treatment groups. The Shapiro–Wilk test was used to assess the distribution of continuous variables. Continuous variables were compared using Student's t test or Mann–Whitney U test as appropriate. Multiple comparisons of BG concentrations across different times of the day in the study subjects were performed using repeated-measures analysis of variance. Categorical variables were compared using the χ2 or Fisher exact test; P value <0.05 was considered significant. Data are presented as mean ± SD for continuous variables and n (%) for categorical variables. Statistical analysis was performed with SPSS Statistics software, version 21. Graphics were prepared with SigmaPlot software, version 11.0.
Results
From March 25, 2014, to September 26, 2014, a total of 2670 patients were hospitalized in the Department of Cardiology. Of these, 54 patients who met the inclusion criteria provided consent. From this group, 27 patients were randomized to receive insulin LM75/25 and 27 patients to receive basal-plus regimen with glargine. After randomization, two patients from each group were excluded because they received <24 h of insulin treatment. A total of 25 patients in the insulin LM75/25 group and 25 patients in the basal-plus group were included in the final analysis. Clinical characteristics of the study patients are shown in Table 2. There were no significant differences between groups in mean age, sex, body mass index, duration of diabetes, glycated hemoglobin (HbA1c), and length of hospital stay. In both groups, each patient had an average of two comorbid conditions with similar distribution. The admitting diagnoses in the insulin LM75/25 group were ischemic heart disease (80%) and valvular heart disease (20%), whereas the basal-plus regimen diagnoses included ischemic heart disease (72%), cardiac arrhythmia (12%), auricular myxoma (8%), valvular heart disease (4%), and heart failure (4%). None of the patients had a history of nephropathy, neuropathy, or retinopathy.
Comparison of proportions by χ2 test.
Comparison between medians by Mann–Whitney U test.
Comparison between means by Student's t test for independent samples.
Comparison of proportions by Fisher exact test.
BMI, body mass index; HbA1c, glycated hemoglobin.
The mean admission glucose for the insulin LM75/25 group was 233.4 ± 63.1 mg/dL and in the basal-plus group was 214.5 ± 46.6 mg/dL (P = 0.235). Changes in glycemic control during the hospital stay are shown in Table 3. Both treatment regimens resulted in prompt and sustained improvement in mean daily BG concentration during the hospital stay, showing similar improvement in daily BG after the first day of therapy but without significant difference (Fig. 1). The percentage of subjects who achieved a mean BG between 70 and 140 mg/dL was higher in the insulin LM75/25 group (72%) than in the basal-plus group (56%); however, the difference was not statistically significant (P = 0.239). The mean BG concentration at the end of follow-up was 131.3 ± 28.4 mg/dL in the insulin LM75/25 group and 143.8 ± 32.5 mg/dL in the basal-plus group, but without significant difference (P = 0.153). The difference between the mean admission glucose and the mean BG at follow-up was 102.1 ± 61.5 mg/dL in the insulin LM75/25 regimen and 70.7 ± 65.4 mg/dL in the basal-plus regimen. These results were significant for each group (both groups with P < 0.001) but not when compared between groups (P = 0.086).
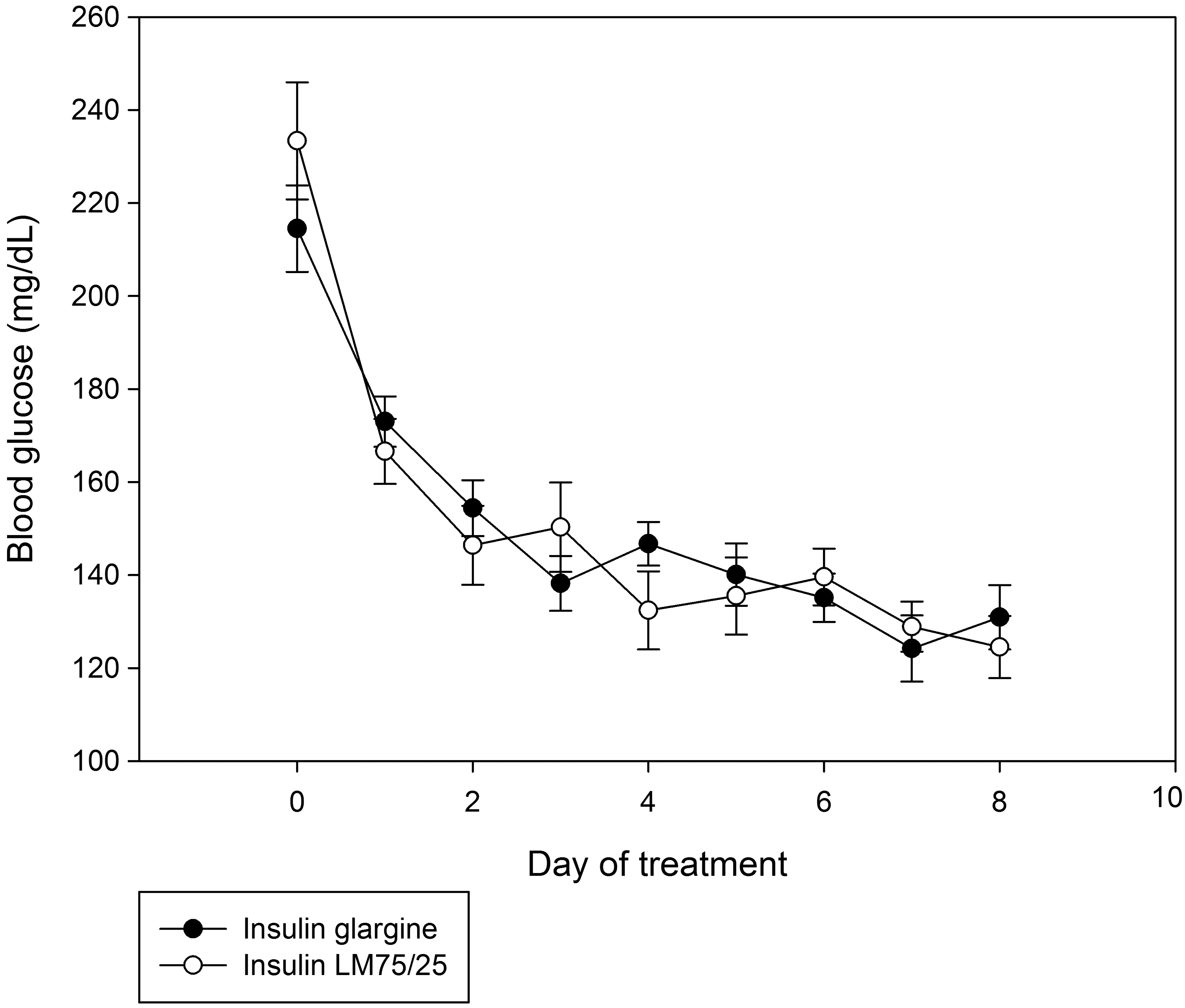
Changes in mean daily blood glucose concentration between patients treated with insulin lispro mix 75/25 (LM75/25) and basal-plus regimen with glargine (mean ± standard error).
Comparison between means by Student's t test for independent samples.
Comparison of proportions by χ2 test.
Value with significance level (P = 0.05).
Comparison of proportions by Fisher exact test.
According to the BG registered at different times of the day, when analyzing each of the groups, there was no difference in mean glucose in the group treated with insulin LM75/25, whereas in the group treated with insulin glargine, the glucose reported at breakfast was lower than that recorded before lunch and bedtime (Fig. 2). Compared with insulin LM75/25, treatment with the basal-plus regimen was associated with lower BG before breakfast (145.9 ± 44.3 vs. 128.1 ± 37.6 mg/dL, P < 0.001) but was higher before lunch (149.2 ± 53.2 vs. 161.4 ± 47.8 mg/dL, P = 0.047) and bedtime (134.9 ± 49.3 vs. 152.8 ± 45.3 mg/dL, P = 0.002). There was no difference in BG before dinner between groups (140.6 ± 49.4 mg/dL in the insulin LM75/25 group and 136.9 ± 50.2 mg/dL in the insulin glargine group, P = 0.536).

Comparison in the blood glucose registered at different times of the day between the insulin lispro mix 75/25 (LM7525) group and the basal-plus group with glargine (mean ± standard error). *P < 0.05.
Total daily dose of insulin (U/kg) was higher in the insulin LM75/25 group (0.34 ± 0.1 U/kg) than in the basal-plus group (0.23 ± 0.1 U/kg; P < 0.001). There was no difference in the supplemental doses of insulin lispro during the hospital stay in both groups.
Hypoglycemia (BG <70 mg/dL) occurred in four patients (16%) in both groups (P = 0.649). Of the 568 glucose readings in the insulin LM75/25 group, there were seven (1.2%) glucose values <70 mg/dL, whereas in the 532 glucose readings in the basal-plus regimen, there were 10 (1.9%) glucose values <70 mg/dL (P = 0.529). In both groups, no glucose values <40 mg/dL were recorded. In all cases, hypoglycemia was corrected with oral dextrose and no episodes were associated with adverse outcomes.
Discussion
This is the first randomized prospective trial comparing the efficacy and safety of a premixed insulin analogue (insulin lispro mix 25, 75% insulin lispro protamine suspension, 25% lispro) with basal-plus regimen with insulin glargine once daily plus corrective doses with lispro before meals in hospitalized patients with T2D. We observed similar improvements in glycemic control in both groups with no differences in the mean daily BG, number of BG readings within aim of treatment, and number of hypoglycemic events.
Hyperglycemia in hospitalized patients is a common, serious, and costly healthcare problem. 22 Evidence from observational and interventional studies indicates that hyperglycemia in critical and noncritical illness is associated with an increased risk of complications such as infections, prolonged hospital stay, disability after hospital discharge, and death. 4 –11 Randomized clinical trials in critically ill and noncritically ill patients have reported that improved glycemic control can reduce the number of hospital complications. 12 –15 Based on this, clinical guidelines from professional organizations recommend the use of subcutaneous insulin as the preferred therapy for glycemic control in hospitalized patients in a non-ICU setting. 16 –18 The most recommended regimen is the basal-bolus insulin therapy. However, this regimen requires subcutaneous administration of basal insulin once or twice daily in combination with prandial and corrective doses of rapid-acting insulin given before meals. The complexity of this approach has limited its acceptance among physicians. 26 –29 Another scheme is the basal-plus regimen, which consists of a single daily dose of basal insulin with supplemental (corrective) doses of rapid-acting insulin analogues before meals. This has a similar efficacy and safety as the basal-bolus regimen. 30,31 However, the basal-plus scheme does not provide prandial coverage of insulin. Therefore, we tested the use of insulin LM75/25 with the hypothesis that use of a premixed insulin analogue is a convenient insulin regimen by providing bolus insulin with meals through a rapid-action component and by fulfilling basal insulin requirements through a protaminated slower release component, and may represent an alternative to the use of the basal-plus regimen in hospitalized subjects with T2D. In the current study, we found that treatment with premixed insulin analogue resulted in similar glucose control as the basal-plus regimen with a prompt and sustained improvement in mean daily BG after the first day of therapy, with a BG aim <140 mg/dL in >70% of patients. These results are similar to those reported in other studies. The basal-plus trial compared the efficacy and safety of a daily dose of glargine plus corrective doses with glulisine before meals against a standard basal-bolus regimen and sliding scale regular insulin in medical and surgical patients with T2D. There was a significant improvement in mean daily BG after the first day of therapy in the intervention groups (163 ± 37 mg/dL for the basal-plus group and 156 ± 36 mg/dL for the basal-bolus group, P = NS). BG aim of <140 mg/dL was achieved in less than half of those groups. 30 A recent study by Bellido et al. compared the efficacy and safety of a premixed human insulin regimen (30% regular insulin and 70% NPH insulin) twice daily with basal-bolus regimen (glargine once daily and glulisine before meals) in medical and surgical patients with T2D and reported a mean daily BG level after the first day of insulin treatment of 179 ± 43 and 175 ± 32 in the premixed human insulin and basal-plus regimens, respectively, with a BG aim between 80 and 180 mg/dL achieved in 54.3% and 55.9%, respectively. 36 In other studies with the basal-bolus scheme, the mean daily BG level after the first day has been reported to range from 145 to 160 mg/dL with a BG aim <140 mg/dL in a range from 45% to 76%. 15,21,22,25,37
Hypoglycemia is an undesirable side effect in hospitalized patients treated with insulin and has potentially harmful outcomes. 38 Hypoglycemia is also the leading limiting factor in improving glycemic control in patients with diabetes. 39 The incidence of hypoglycemia in noncritical patients treated with insulin has been reported to range from 0.2% to 64.1%. 15,21 –25,30,36 In agreement with previous studies, 15,21,22,30 we show that the use of insulin LM75/25 is well tolerated with a low rate of hypoglycemia (BG <70 mg/dL in 16% of patients). There were no patients with severe hypoglycemia (BG <40 mg/dL). However, in the study by Bellido et al., hypoglycemia occurred in 64.1% of patients treated with premixed human insulin regimen during the hospital stay, which resulted in the interruption of the study according to their safety protocol (prespecified stopping rule of >50% of hypoglycemic events). 36 The higher rate of hypoglycemia with the use of premixed human insulin compared with the treatment with premixed insulin analogue in our study is likely the result of a higher dose of insulin (0.3–0.4 U/kg for the premixed human insulin vs. 0.2–0.3 U/kg for the premixed insulin analogue). Furthermore, the pharmacokinetic profile of premixed insulin analogue has less intraindividual variability with a greater glucose-lowering activity and lower risk of hypoglycemia than premixed human insulins. 40 –42 Minimizing the rate of hypoglycemic events is of major importance in hospitalized patients because it has been shown to be an independent risk factor of poor clinical outcome. 38
With respect to the insulin dose used in our study, the dose received in the insulin LM75/25 group was similar to the “conservative protocol” used by Buchs et al. 23 and the insulin glargine dose was calculated according to the proportion of basal insulin received in the insulin LM75/25 group. In both treatment groups, the insulin dose was lower than that used in other studies, but the efficacy and safety in the two schemes was similar to those studies. 21,22,25,30,36,37 The lower insulin glargine dose perhaps also explains the lack of differences between groups and the higher value of glucose before lunch and dinner. However, our findings are similar to those found in the basal-plus trial, in which the basal-plus regimen used half of the insulin dose used in the basal-bolus scheme and both regimens resulted in similar glycemic control with a low rate of hypoglycemia. 30
An important point to consider for the application of insulin in a hospital setting is the changes in oral intake and insulin requirements. In individuals with lack of oral intake or fasting periods, administration of the basal-plus scheme may be preferable. However, if the patient is able to eat without difficulty and does not need fasting, administration of a premixed insulin analogue may be an option.
We recognize several limitations to the study, including the relatively small number of patients recruited and the fact that the study was conducted in a single institution with patients only from a single clinical department. The study also excluded patients admitted to or expected to require ICU admission, patients undergoing cardiac surgery, those with corticosteroid therapy, clinically relevant hepatic disease (Child–Pugh score B or C) or impaired renal function (serum creatinine ≥2.0 mg/dL), and pregnant patients. We also excluded patients with severe hyperglycemia (>400 mg/dL) and patients who were receiving a total dose of insulin >0.4 U/kg/day before admission. For such patients, higher insulin doses or a standard basal-bolus approach may be the preferred approach in achieving glycemic control. In addition, our study was not powered to determine differences in hospital complications across groups and the estimated sample size was possibly insufficient to measure the impact of secondary outcomes. A large, prospective, randomized multicenter clinical trial of glycemic control is certainly needed to address these important issues. These studies should include additional treatment regimens such as the use of basal-bolus regimen with analogue or human insulin and premixed human insulin.
In summary, the results of our pilot study indicate that the inpatient use of a premixed insulin analogue (LM72/25) resulted in a similar improvement in glycemic control and hypoglycemic outcomes compared with the basal-plus regimen. These results indicate that premixed analogue insulin may be an effective alternative in the management of hyperglycemia in hospitalized patients with T2D. However, this result should be interpreted with caution because it included a relatively small number of patients. Further larger controlled studies are needed to validate these findings.
Footnotes
Acknowledgments
The authors thank the contribution of Dr. Joaquin Vargas Peñafiel, who collaborated in the conduction of this study, and Dr. Alejandro Correa Flores, who contributed with his expertise and knowledge. Also, the authors thank Nutritionist Luz Maria Graciela Cuellar Vazquez, for her close cooperation in the nutritional care of the patients.
Author Disclosure Statement
No competing financial interests exist.